
Abstract
Objectives
The aim of the present study was to assess the gamma-aminobutyric acid type A (GABAA) receptor antagonist flumazenil and its effect on the anesthetic activity of the GABAA receptor agonist alfaxalone when administered intravenously in cats.
Methods
A prospective, randomized, blinded, two-period two-treatment crossover study was conducted. Eight (six male, two female) healthy adult neutered cats, 4.5–7.0 kg body weight, owned by IndyVet Emergency and Specialty Hospital were enrolled. Cats were randomly assigned to one of two treatment groups, flumazenil or saline (period 1). During period 2, cats were administered the opposite treatment. Treatment was either 0.1 mg/kg flumazenil or an equal volume of 0.9% sodium chloride. Before treatment, a published, abbreviated alfaxalone protocol was administered, consisting of an intravenous (IV) dose of 2 mg/kg over 1 min, followed by an abbreviated two-step IV alfaxalone infusion of 0.4 mg/kg/min for 10 mins, then 0.3 mg/kg/min for 30 mins. Physiologic parameters, time to lateral recumbency, sternal recumbency and standing, duration of anesthesia, quality of induction and maintenance of anesthesia, and quality of recovery were assessed.
Results
The treatment by time interaction was not significant for any variable. Pulse rate was significantly higher in the flumazenil group than the saline group (mean 176.01 vs 169.57; P = 0.0067).
Conclusions and relevance
Flumazenil administered at 0.1 mg/kg intravenously over 1 min did not antagonize the effects of alfaxalone in cats. Further investigations are required to investigate an appropriate dose or other drug to antagonize alfaxalone and its judicious use in clinical settings.
Introduction
Alfaxalone (3α-hydroxy-5α-pregnane-11,20-dione) is a synthetic neuroactive steroid that interacts with and modulates gamma-aminobutyric acid type A (GABAA) receptors, producing anesthesia and muscle relaxation. Alfaxalone formulated in a preserved, aqueous solution, containing 2-hydroxypropyl-β-cyclodextrin, is a proprietary formulation (Alfaxan Multidose [AMD]; Jurox [a part of Zoetis]) registered and indicated for the induction and/or maintenance of anesthesia in cats and dogs. 1
Alfaxalone has been studied to evaluate its use and efficacy as an intermittent bolus and infusion drug.2 –13 To understand the effective plasma concentration in the cat, Pypendop et al14,15 performed a target-controlled IV anesthesia study with AMD, which calculated the effective alfaxalone plasma concentration required to achieve immobility during stimulation in 99% of non-premedicated cats (EC99) to be 7.6 mg/l. This allowed for pharmacokinetic-based dosing regimen designs in cats. A follow-on study compared two intravenous (IV) anesthetic regimens for target EC99, which found that after an IV alfaxalone bolus, three successive constant rate infusions (CRIs) with fixed-duration step-down decreases was the best technique in cats. 15
There is no known tested and proven drug to antagonize alfaxalone in cats. AMD is an anesthetic drug with a wide safety margin; however, adverse events can occur with its use, including apnea and respiratory and cardiovascular depression, as well as prolonged recovery with muscle tremors, ataxia and post-emergence delirium. If an alfaxalone antagonist could be scientifically verified, it could be used to antagonize adverse and unwanted drug effects. Flumazenil competitively antagonizes drugs at the GABAA receptor. 16 A 2020 study investigated the use of flumazenil as a reversal drug for Egyptian fruit bats treated with alfaxalone and midazolam, concluding that flumazenil decreased the time and improved the quality of recovery. 17 In another study, chicks were administered an intraperitoneal injection of alfaxalone, followed by flumazenil intramuscularly, which found that flumazenil reduced the anesthetic period in a dose-dependent manner. 18
The objective of this study was to assess whether flumazenil would antagonize the effects of alfaxalone at effective plasma concentration using a modified version of the step-down anesthetic protocol established by Pypendop et al.14,15 We hypothesized that the dose of flumazenil administered (0.1 mg/kg IV – a dose equal to a dose previously administered in ketamine-midazolam anesthetized cats) 19 would antagonize the effects of alfaxalone. The flumazenil 0.1 mg/kg IV dose is the typical dose administered to humans for benzodiazepine intoxication. 16
Materials and methods
This study was conducted at IndyVet Emergency and Specialty Hospital (IVESH), using IVESH-owned cats housed on location as part of the closed blood donation colony. Cats were previously obtained from humane societies or shelters as young adults and were vetted. This opportunistic study was performed in compliance with the National Research Council’s Guidelines, 20 utilizing previously established safe doses of AMD and flumazenil in the cat. The IVESH ownership’s informed consent to utilize its cats was obtained by study personnel after final study approval was granted and before execution. Before obtaining approval, each cat was previously scheduled to participate in two anesthetized blood donation collections with a minimum rest period of 6 weeks between each donation.
Eight (six male and two female) healthy adult neutered cats were selected for enrollment based on availability within the donation schedule. Cats were housed with one additional cat within double cages measuring 48 × 24 × 24 inches. Each cage had individual food, water and toileting areas. Communal activities occurred during the day except on treatment days. Cats were fed Advance Premium Adult dry food (Mars Petcare USA) or a prescription diet, twice daily, except on treatment days. Cats received lysine powder supplementation and had free access to fresh potable water. Included cats were aged 23–90 months, with no clinically significant abnormalities on physical examination, complete blood count and biochemistry. Cats weighed a mean (±SD) of 5.8 ± 0.9 kg (period 1) and 5.8 ± 0.8 kg (period 2). Cats were excluded if they had been administered central nervous system active drugs in the 30 days before the study date.
Each cat was assigned an ID and organized into two cohorts. Each cohort was balanced for treatment (ie, two cats were randomly allocated to receive flumazenil and two cats were randomly allocated to receive saline). A treatment schedule was created to determine the order of treatment on each day. The allocation of cats to cohorts, treatment and treatment schedule was determined by a ‘draw from the hat’ method.
Each cat underwent a physical examination no earlier than 24 h before treatment day. The included cats were fasted for at least 10 h preceding the cohort’s treatment period. Drug calculations were performed and verified by two individuals: a blinded primary investigator (PI2) and a non-blinded primary investigator (PI1). PI1 obtained assistance for verification of medication dosages and assignments from a non-blinded person and prepared doses of AMD, flumazenil and saline. Syringes were labeled for each cat, and treatment of either flumazenil and saline was labeled with the cat ID and period number, to maintain blindness of PI2. Cephalic IV catheters were placed before treatment. The previously established standard alfaxalone anesthetic protocol for cats 15 was utilized to produce an induction dose of 2 mg/kg IV over 1 min, followed by an abbreviated, two-step IV infusion of 0.4 mg/kg/min for 10 mins, followed by 0.3 mg/kg/min for 30 mins. During the 30 min 0.3 mg/kg/min CRI, a 60 ml jugular blood collection was performed, along with injections of iron dextran intramuscularly, vitamin B complex subcutaneously and subcutaneous fluids of a balanced crystalloid solution. Once completed (ie, 41 mins after AMD was first administered), PI1 administered flumazenil based on a published dose for the cat within Ilkiw’s 2002 study 19 (0.1 mg/kg, 0.1 mg/ml, Flumazenil Injection; Fresenius Kabi) or saline (1 ml/kg, Vetivex; Dechra) over a 1 min IV infusion.
Accurate infusion times and recorded observations in association with time from treatments being administered were documented. Definitions of anesthesia event times can be seen in the supplementary material. During the abbreviated two-step IV infusion and up to the time of sternal recumbency after treatment, pulse rate (PR; beats/min), respiratory rate (RR; breaths/min), mucosa color, capillary refill time (CRT; s), presence of apnea, palpebral reflex, pupillary position, jaw tone and toe pinch withdrawal were recorded every 5 mins and rectal temperature (°F) every 15 mins. Before starting, each cat was placed on a Gaymar Circulating Thermal Water System to attempt to maintain normothermia. Percentage saturation of hemoglobin with oxygen (SpO2) was assessed with pulse oximetry (Rad-5v Oxygen Saturation Monitor; Masimo) placed on the tongue and recorded every 5 mins for the first 50 mins. If SpO2 was observed to be less than 90%, supplemental oxygen was administered as flow-by.
After treatment (ie, flumazenil or saline) was administered, PI2 observed, evaluated and documented the characteristics of recovery every 5 mins, which included observations for body movements, vocalization and change in behavior until standing or ambulatory. Recovery was completed when the cats were safe to return to the colony when normothermic, able to ambulate without assistance and vital signs were within normal limits. The quality of induction, anesthesia and recovery were assessed and recorded by PI2. The quality of induction was assessed from the start of AMD administration to the time of lateral recumbency. PI2 observed the anesthetic induction period to award an induction score using the subjective visual analog score (VAS) by placing a mark on a line 100 mm long and using the scale of worst possible induction as zero and best possible induction as 100 (see supplementary material). Categorical scores (see supplementary material) were assigned to further evaluate the quality of induction. The quality of anesthesia was assessed from the start of lateral recumbency to completion of AMD administration. PI2 awarded an anesthetic effectiveness score using the subjective VAS. The quality of recovery was assessed every 10 mins starting at 45 mins or approximately 5 mins from the start of treatment with flumazenil or saline until the cat was able to stand without assistance. PI2 awarded a recovery score using a categorical scoring system. The physical variables of jaw tone, palpebral reflex, pupillary position and toe pinch withdrawal were scored for assessment (see supplementary material).
A physical examination was performed no earlier than 24 h after treatment completion. After period 1, cats underwent a 6-week washout period before period 2. Period 2 was performed in an identical manner to period 1, except that each cat was administered the opposite treatment received in period 1.
Statistical analysis
The statistical analysis was performed using SAS statistical software version 9.4 (SAS Institute). Physiological measures collected throughout the anesthetic and treatment period were analyzed through analysis of covariance (ANCOVA), using the baseline values as the covariate. The statistical model included treatment sequence, period, treatment group, time and the treatment group by time interaction as fixed effects, and animal nested in sequence as a random effect. For single data points, including duration of sedation, temperature at sternal recumbency, time to standing, first breath, lateral recumbency and sternal recumbency, as well as data points of jaw tone, palpebral reflex, pupillary position and toe pinch withdrawal, ANOVA was utilized. The model described above, excluding the time component, was used in this analysis. A generalized linear mixed model was utilized to analyze the categorical outcomes associated with the scores for quality of induction, quality of recovery, return to consciousness, environmental interaction and ataxia, as well as the VAS scores for quality of anesthesia and quality of induction. The generalized linear mixed model assumed a multinominal distribution. The model described above, excluding the time component, was used in this analysis. Differences between treatment groups were evaluated with P <0.05 indicating statistical significance.
Results
The recording of data was initiated at baseline and repeated through recovery, providing up to 11 assessments for each time point. Performed assessments included PR, RR, rectal temperature, mucosa color, CRT, SpO2 and presence of apnea, as well as palpebral reflex, pupillary position, jaw tone and toe pinch withdrawal.
Cats were treated with flumazenil or saline immediately after the end of the 41 min AMD protocol, with time points in the range of 45–165 mins included in the statistical analysis using ANCOVA with least squares mean (LS mean) and pooled SEM to summarize results. A limited number of observations occurred after the 165 min mark and were not included. Values collected at the 30 min mark for temperature and 40 min mark for PR and RR were utilized as baseline values. The mean PR was found to be significantly higher in the flumazenil group than in the saline group (176.01 [SEM 5.72] beats/min vs 169.57 [SEM 5.71] beats/min; P = 0.0067) (Table 1, Figure 1). It was determined that RR and temperature did not differ significantly between groups (Table 1, Figures 2 and 3).
Summary of the repeated measures for pulse rate, respiratory rate and rectal body temperature analyzed using ANCOVA and time to event variables analyzed using ANOVA

Values in bold are statistically significant (P <0.05)
The treatment by time interaction was not significant for any of these outcomes, therefore the main effect of treatment was assessed and presented
Significantly different from the SAL group
Time to event variables analyzed using ANOVA
ANCOVA = analysis of covariance; FLU = flumazenil; LS = least squares; PR = pulse rate; RR = respiratory rate; SAL = saline
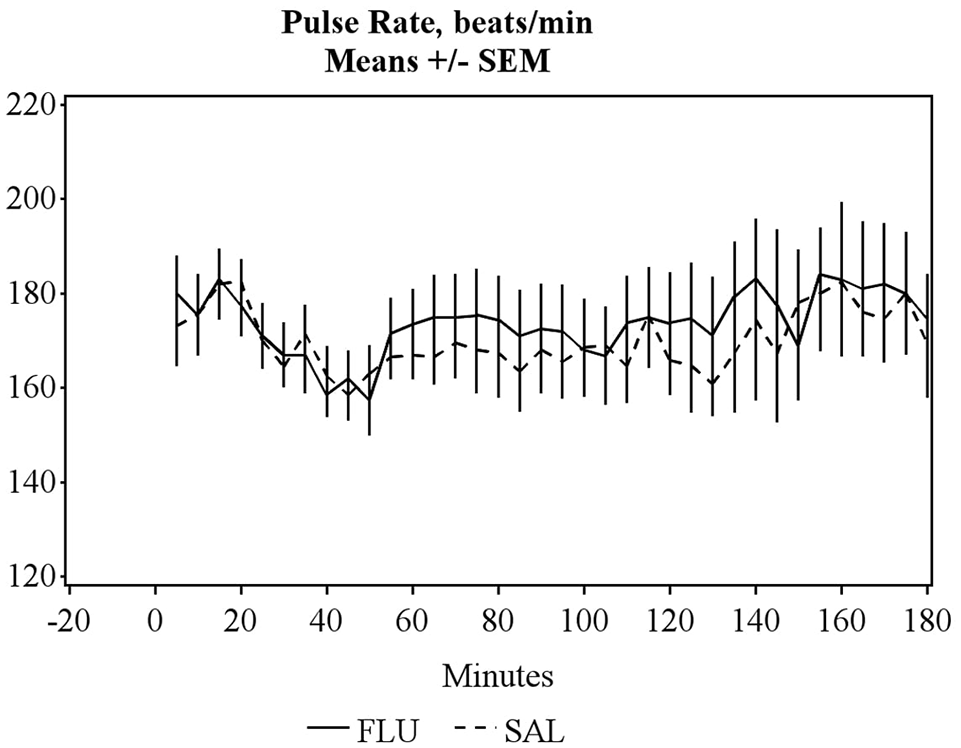
Mean pulse rates vs time in cats anesthetized with alfaxalone. Treatment with either flumazenil (FLU) or saline (SAL), after alfaxalone administration, was performed at the 45 min mark

Mean respiration rates vs time in cats anesthetized with alfaxalone. Treatment with either flumazenil (FLU) or saline (SAL), after alfaxalone administration, was performed at the 45 min mark
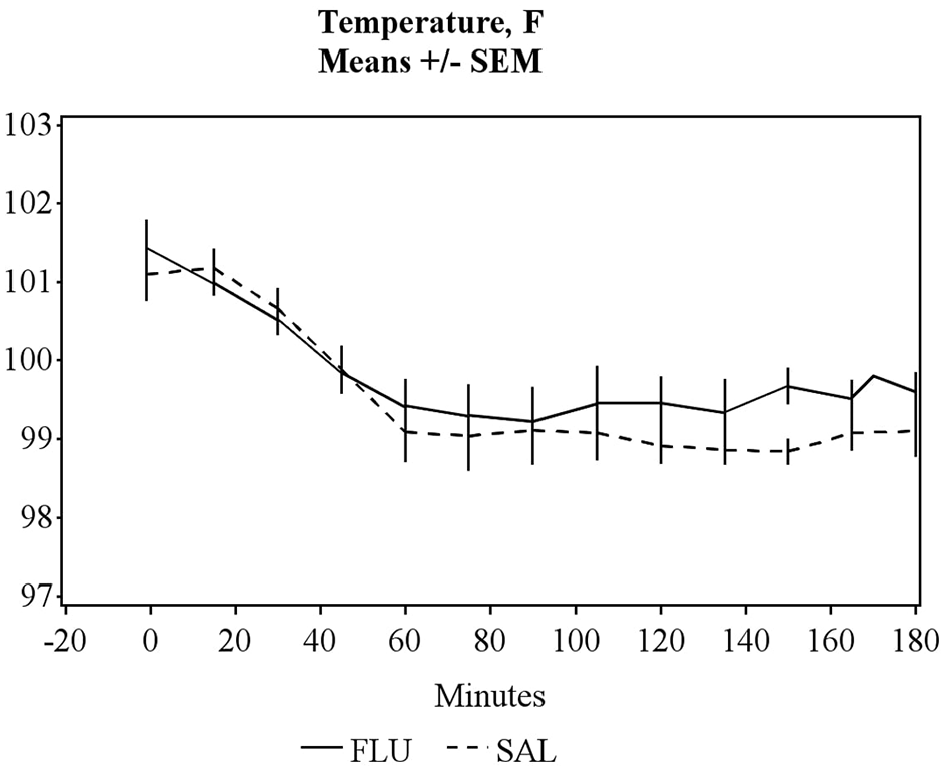
Mean temperatures vs time in cats anesthetized with alfaxalone. Treatment with either flumazenil (FLU) or saline (SAL), after alfaxalone administration, was performed at the 45 min mark
ANOVA was performed on events that included time to first breath, lateral recumbency, sternal recumbency and standing, duration of sedation and temperature at sternal recumbency. After the IV AMD bolus, all cats became laterally recumbent within a mean time of 59.25 ± 10.58 s (range 41–83). The mean time to first breath was 6.69 ± 3.16 s (range 2–13). Apnea was not observed in any cat. No significance was reported between groups for time to event variables (Table 1).
The mean quality of induction of anesthesia categorical score was good at 3.12 (range 2–4) and mean VAS for quality of induction was also good at 88.63 (range 80–100). During induction of anesthesia in period 1, excitation consisting of slight vocalizations, lip licking or biting motions, as well as sit to stand movements, were observed in three cats. During induction of anesthesia in period 2, the same excitation behaviors were observed in three cats, two of which had also exhibited them during period 1. The mean VAS score for quality of anesthesia was very good at 94.4 for flumazenil and 91.0 for saline (SEM 2.0) (Table 2). Quality of induction based on VAS outcome was found to be significantly higher for flumazenil than saline (LS mean 92.3 vs 85.0, SEM 2.3; P = 0.0485) (Table 2). The quality of induction based on categorical score was also found to be significantly higher with flumazenil than saline (median [range] 4 [3–4] vs 2 [2–4]; P = 0.0457) (Table 2).
Summary of the quality of anesthetic induction, anesthesia and recovery from anesthesia scores observations

Values in bold are statistically significant (P <0.05)
VAS values are LS mean and SEM, with categorical score outcomes summarized as median and range
Significantly different from the SAL group
FLU = flumazenil; LS = least squares; SAL = saline; VAS = visual analog scale
SpO2 was measured, with no cats in period 1 having values ⩽90%, while six cats (1, 2, 4, 6, 7 and 8) in period 2 had SpO2 ⩽90%. SpO2 was re-evaluated and tongue probe placement was adjusted to ensure good contact, resulting in 4/6 cats in period 2 having SpO2 values >90%. Cats 7 and 8 had an SpO2 of 89% and 88%, respectively, and flow-by 100% oxygen supplementation was performed with an increased SpO2 by the next assessment time.
The final time to event physical variables were analyzed by ANOVA, for a two-period crossover. None of the variables was found to be significant when comparing flumazenil and saline (Table 3).
Summary of the time to event (mins) physical variables

Data are LS mean and pooled SEM analyzed by ANOVA
FLU = flumazenil; LS = least squares; SAL = saline
Discussion
The aim of the present study was to assess whether flumazenil would antagonize the effects of alfaxalone and shorten the recovery period in cats. This study determined there was no significant difference in recovery quality or duration between flumazenil and saline. Therefore, flumazenil, at this study’s administered dose, did not antagonize the effects of alfaxalone administered at a proven anesthetic dose rate.
The alfaxalone anesthetic protocol chosen for this study was based on a previously published step-wise infusion protocol. 15 This study’s loading dose of 2 mg/kg and infusion rates of 0.4 mg/kg/min and 0.3 mg/kg/min were selected based on previously established pharmacokinetic parameters for alfaxalone and determined to be an adequate protocol for collection of blood from donor cats. Additional alfaxalone supplementation was not required.
This study’s dose of flumazenil was based on a previous study. 19 Ilkiw et al 19 evaluated the effect of flumazenil at varying dosages, after administration of ketamine and midazolam in 18 cats. Each cat received 3/6 dosage regimens of either IV flumazenil at 0.0, 0.001, 0.005, 0.01 and 0.1 mg/kg, 5 mins after being administered 3 mg/kg of ketamine and 0.5 mg/kg of midazolam IV, or 0.1 mg/kg flumazenil IV after 3 mg/kg ketamine and saline IV. Flumazenil was found to have a significant effect, with higher doses causing a more ‘alert’ body position but no shortening of anesthesia duration. The study by Ilkiw et al did not objectively assess PR, RR and temperature, which may have indicated antagonism of midazolam by flumazenil. 19 In our study, vital signs were assessed and only PR was found to be significantly affected, though the clinical difference was only 7 beats/min, which is not clinically significant outside of this study. It would be interesting to revisit the study by Ilkiw et al 19 to assess if the cardiorespiratory parameters changed after treatment with higher doses of flumazenil. In addition, Ilkiw et al’s 19 study assessed a ketamine-midazolam drug combination and reversal of midazolam was anticipated. The overall finding of the study by Ilkiw et al 19 was that flumazenil did not produce a significant decrease in the duration of anesthesia. However, the lack of effect of flumazenil is more likely due to the potent and dominant anesthetic effects of ketamine rather than the lack of effect of flumazenil on midazolam.
Flumazenil is a proven benzodiazepine antagonist, chosen as the hypothesized reversal drug for alfaxalone because of its commercial availability and mechanism of action (MOA). Flumazenil is known to competitively inhibit the binding of GABAA receptor ligands on the GABA/benzodiazepine receptor complex, which is located between the alpha and gamma subunits of the GABAA receptor. Binding only occurs if the receptors contain the gamma 2 and alpha 1, 2, 3 or 5 subunits. 21 Alfaxalone’s MOA occurs by binding GABAA cell surface receptors, commonly on alpha and occasionally beta subunits. This could explain this study’s finding of flumazenil not significantly affecting the recovery response in cats, because of different subunit binding requirements for benzodiazepine agonists/antagonists vs alfaxalone. In addition, the pharmacokinetics and duration of effect of flumazenil in the cat are not known. Flumazenil competes for receptor binding, ‘waiting’ for the spontaneous disassociation of the agonist. If the duration of effect for flumazenil is shorter in cats than in other species, a single dose may not be adequate to antagonize and redosing may be required.
Two previous studies have reported that flumazenil reverses the effects of alfaxalone. Tuval et al evaluated the reversal of alfaxalone and midazolam with flumazenil in Egyptian fruit bats. 17 A total of 10 healthy male bats were randomly selected and anesthetized with a combination of 15 mg/kg alfaxalone and 2 mg/kg midazolam subcutaneously. One hour after treatment, either 0.3 mg/kg flumazenil or an equivalent volume of 0.9% saline was administered subcutaneously, finding flumazenil significantly reduced the recovery time from 45 to 10 mins. In Alatroshi and Naser’s study, 1-day-old male and female Ross broiler chicks were randomly distributed into four groups. 18 All groups were administered 50 mg/kg alfaxalone intraperitoneally with doses of intramuscular flumazenil at 0 mg/kg, 0.05 mg/kg, 0.1 mg/kg and 0.2 mg/kg administered immediately after. They found flumazenil reduced the anesthetic period of chicks in a dose-dependent manner. Both studies show flumazenil reversing alfaxalone effects; however, these results may differ from our results because of the possibility that different subtypes of the GABAA receptor are present between species. There is a common mammalian GABAA receptor structure, (alpha1)2(beta2)2(gamma1), 21 but 16 subunits and 19 genes have been determined to combine and compose the GABAA receptors, which are composed of five protein subunits, each of which can belong to a different subunit class. 22 This genetic diversity increases the heterogeneity of GABAA receptors. In addition, different subtypes of GABAA receptors have been found to exist between mammals. 23 The possibility of differing species subtypes is important to investigate further as they provide multiple types of function, but also multiple responses to drugs having affinity for the GABAA receptor, which include alfaxalone and flumazenil ligands. In addition, the study by Tuval et al 17 is confounded by the bats being treated with both alfaxalone and midazolam, 17 where treatment effect may only be related to the effect of flumazenil on midazolam.
The limitations of this study include it being an opportunistic study which meant a pilot study and power calculation were not performed. The number of cats to be investigated was also limited because of previously scheduled hospital blood donations and the inability to disrupt the schedule. Study cats varied in body weight and body condition. Variations could have affected the depth and effects of alfaxalone with its known peripheral tissue distribution, 24 possibly contributing to slower clearance in heavier cats. An additional limitation was the inability to perform a dose characterization of flumazenil. There was only one opportunity to use the cats; therefore, only one dose of flumazenil, albeit a high dose, could be investigated. Further studies at higher doses or longer exposure times (ie, infusion) may be needed to rule out the reversing effects of flumazenil on alfaxalone. Another study limitation involves the use of non-validated scoring systems for the quality of anesthesia; however, these non-validated scoring systems have been used successfully for the assessment of AMD in cats and its eventual registration with the US Center for Veterinary Medicine. 25
Conclusions
An IV dose of flumazenil at 0.1 mg/kg did not antagonize the anesthetic effects of alfaxalone when administered with an abbreviated two-step infusion. Based on this study, the use of the studied dose of flumazenil to antagonize cats being administered alfaxalone cannot be recommended.
Supplemental Material
Appendix 1
Time to event definitions.
Supplemental Material
Appendix 2
Visual analog scoring of anesthesia.
Supplemental Material
Appendix 3
Quality of induction of anesthesia categorical scores.
Supplemental Material
Appendix 4
Physical variable assessment scores.
Footnotes
Acknowledgements
The authors would like to thank Jurox US (now a part of Zoetis) for its support and for funding the supply of the Alfaxan Multidose used in the study, as well as providing funding for the statistical analysis of the data. The authors would also like to thank Steve Radecki for his expertise and assistance in performing the statistical analysis. In addition, the authors would like to thank IndyVet Emergency and Specialty Hospital and its Blood Donation Center for its permission to use the cats and facilities for this study and providing personnel to assist.
Author note
The results of this study were presented as an oral abstract at the 2022 American College of Veterinary Anesthesia and Analgesia Scientific Session, ACVS Surgery Summit, Portland, OR, USA.
Supplementary material
The following files are available as supplementary material:
Appendix 1. Time to event definitions.
Appendix 2. Visual analog scoring of anesthesia.
Appendix 3. Quality of induction of anesthesia categorical scores.
Appendix 4. Physical variable assessment scores.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by Jurox US (now a part of Zoetis).
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for the procedure(s) undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.