
Abstract
Objectives
The aim of the study was to evaluate the association between triage body temperature (BT) and outcome in cats presenting to the emergency department (ED).
Methods
A retrospective observational study was conducted on cats presented to the ED. BT, clinical diagnosis and outcome were recorded. BT was categorised as follows: normothermia (37.8–39.7°C); hyperthermia (⩾39.8°C); mild hypothermia (36.8–37.7°C); moderate hypothermia (35.6–36.7°C); severe hypothermia (33.1–35.5°C); and critical hypothermia (⩽33°C). Outcome in the ED was categorised as death, euthanasia, hospital admission and discharge. Outcome at hospital discharge was evaluated in patients admitted to the intensive care unit (ICU). Systemic inflammatory response syndrome (SIRS) was identified in patients. No-SIRS cats were divided into three disease categories (urinary system, cardiovascular and miscellanea) and SIRS cats into four categories (urinary system, cardiovascular, trauma and miscellanea). The presence of sepsis was evaluated. Non-parametric statistics were used.
Results
A total of 1440 cats were included. The hospital mortality rate was 21.9%. Hypothermia in the ED was reported in 510 (35.4%) cats, normothermia in 849 (59%) cats and hyperthermia in 81 (5.6%) cats. In the ED, the median temperature in non-survivors (35.4°C, 95% confidence interval [CI] 34.6–36.3) was significantly lower than in survivors (38.2°C, 95% CI 38.1–38.3; P <0.0001). The risk of non-survival in the ED was significantly higher in cats with a decreased BT, progressively increasing with the severity of hypothermia (P <0.0001). Furthermore, BT was significantly associated with a higher risk of mortality in the ICU (P <0.0001). A diagnosis of sepsis was associated with a high prevalence of hypothermia (79/124 cats, 63.7%) and a higher risk of non-survival (odds ratio [OR] 2.62, 95% CI 1.52–4.54; P = 0.0006). The mortality risk significantly increased in SIRS cats with a cardiovascular disease (OR 8.27, 95% CI 4.09–16.68; P <0.0001).
Conclusions and relevance
Hypothermia is common in cats at ED admission and is significantly associated with outcome. Triage hypothermia might identify patients with sepsis or SIRS complicated by comorbidities, such as cardiovascular and urinary diseases.
Introduction
Body temperature (BT) is a vital sign routinely used as a triage tool in the emergency department (ED) to prioritise therapeutic interventions in people. 1 Lower values of BT at ED admission have been associated with high odds of mortality and high risk of admission to the intensive care unit (ICU) for several critical care conditions, including acute poisoning, bacterial infection and sepsis.2–9 Notably, hypothermia has been associated with four- to six-fold greater odds of mortality than hypotension in septic patients presented to the ED. 9
The association of low BT with morbidity and mortality has been reported in specific feline diseases. Hypothermia, indeed, is a typical clinical sign in cats presenting with different critical care conditions, such as shock, sepsis and systemic inflammatory response syndrome (SIRS). 10 Furthermore, in previous studies, decreased BT was associated with the presence of azotaemia 11 and Lee et al 12 demonstrated that hypothermia is a useful predictor of death in cats with acute kidney injury (AKI) in the ED. Moreover, cats with trauma have high odds of mortality if they have low BT upon ED admission, as already reported in dogs and humans.13,14
To our knowledge, the prevalence and prognostic significance of alterations in BT have never been evaluated in cats admitted to an ED. The primary aim of this retrospective study, therefore, was to identify the potential of triage BT to independently predict 1-day mortality in cats referred to an ED. The secondary aims were to evaluate the association between triage BT and the risk for ICU admission and ICU mortality, and to investigate the association between triage BT and specific disease categories.
Materials and methods
All cats presented to the ED of a veterinary university hospital (VUH) between January 2018 and December 2021 were identified by searching the electronic medical record system (Fenice; ZakSoft). Cats presented to the ED were included if the value of BT at triage and the final outcome were recorded in an emergency medical report. Patients discharged against medical advice were excluded.
The medical records were reviewed and the following variables were recorded: signalment (breed, sex, neuter status, age); body weight; heart rate; respiratory rate; non-invasive blood pressure; meteorological seasons of presentation (spring, summer, autumn, winter); and final diagnosis when possible. For the purposes of the current study, hyperthermia and hypothermia were defined by a BT >39.7°C and <37.8°C, respectively, based on the SIRS criteria published for cats. 15 Cats with hypothermia were further classified into four categories according to a previously reported stratification for secondary hypothermia: 16 mild hypothermia (36.8–37.7°C); moderate hypothermia (35.6–36.7°C); severe hypothermia (33.1–35.5°C); and critical hypothermia (⩽33°C). Hypotension was defined by a systolic blood pressure <90 mmHg. Blood pressure was measured through an oscillometer (Suntech Vet30; SunTech) or Doppler ultrasound probes (Minidop ES-100VX; Hadeco). Enrolled cats were grouped according to their age as follows: kitten (0–1 year); young adult (1–6 years); mature adult (7–10 years); and senior (>10 years). 17
The final diagnosis was based on data reported in the medical records and classified focusing on those conditions more frequently associated with BT alterations in critical feline patients. In this regard, the population was divided into cats with SIRS and without SIRS. Patients without SIRS were further classified into three disease categories: urinary system diseases; cardiovascular diseases; and miscellanea (Figure 1). SIRS was defined by previously reported criteria 15 and was further classified into four subgroups based on the primary disease or comorbidity: SIRS-urinary; SIRS-cardiovascular; SIRS-trauma; and SIRS-miscellanea. Furthermore, the diagnosis of sepsis in patients with SIRS was based on the presence of a documented or highly suspected infection. The primary outcome included mortality in the ED, classified as spontaneous death or euthanasia, admission to the ICU or in the general ward (GW), and hospital discharge. The decision to move the patient to the ICU or GW was clinician dependent. Secondary outcomes were ICU mortality, defined as survival to hospital discharge, death or euthanasia.

Flow chart of the study population and classification based on disease categories. BT = body temperature; ED = emergency department; SIRS = systemic inflammatory response syndrome
Statistical analysis
The normality of data was assessed using the D’Agostino–Pearson K² test. Data were reported as median and range (25th and 75th percentile) or mean ± SD, based on their distribution. Non-parametric statistics (Mann–Whitney U-test, Kruskal–Wallis test with post hoc comparison according to Conover) were used to compare the continuous variables between different groups. Categorical variables were compared among groups using Fisher’s exact test. The association between the variables of interest and outcome was examined using a univariate regression analysis, and the variables that were associated with the outcome (P ⩽0.1) were included in the multivariable regression model (stepwise selection); results were presented as odds ratios (ORs) with 95% confidence intervals (CIs). For all tests applied, P <0.05 was considered significant. Statistical analyses were performed using statistical software packages (MedCalc Statistical Software version 19.1.3; MedCalc Software; and GraphPad Prism version 10.0.0 for Windows; GraphPad Software).
Results
Population
A total of 1539 records were reviewed; 99 cats were excluded because they were discharged against medical advice. Finally, 1440 cats that presented to the ED in the study period were included, with 574/1440 (39.9%) castrated males, 413/1440 (28.7%) spayed females, 272/1440 (18.9%) intact males and 181/1440 (12.6%) intact females. The median age was 6.5 years (range 0.2–24): 161/1413 (11.4%) patients were kittens; 544/1413 (38.5%) were young adults; 222/1413 (15.7%) were mature adults; and 486/1413 (34.4%) were seniors. Of the 1440 cats, domestic shorthairs were the most represented (n = 1285, 89.2%), followed by Maine Coons (n = 31, 2.2%), Persian cats (n = 27, 1.9%) and other breeds (n = 97, 6.7%). Regarding the season of encounter, 417/1440 (29%) patients were referred to the ED in summer, 382/1440 (26.5%) in spring, 360/1440 (25%) in winter and finally 281/1440 (19.5%) in autumn. Outcome categories at the ED were discharge (n = 378, 26.2%), hospital admission (n = 964, 66.9%), death (n = 25, 1.7%) or euthanasia (n = 98, 6.8%). Overall, the hospital mortality rate was 21.9% (315/1440 cats): 167 (11.6%) cats spontaneously died and 148 (10.3%) were euthanased.
Triage BT and outcome in the ED
The median triage BT recorded in enrolled cats was 38.1°C (range 37.3–38.8). Normothermia was reported in 849/1440 (59%) cats, while 510/1440 (35.4%) cats had hypothermia and 81/1440 (5.6%) had hyperthermia. Among the cats with hypothermia, 249/510 (48.8%) had mild hypothermia, 107/510 (21%) had moderate hypothermia, 98/510 (19.2%) had severe hypothermia and 56/510 (11%) had critical hypothermia (Figure 2).

Graphical representation of the number of cats admitted to the emergency department, clustered by the different temperature categories: CHT = critical hypothermia; HT = hyperthermia; MHT = mild hypothermia; ModHT = moderate hypothermia; NT = normothermia; SHT = severe hypothermia
The median temperature in non-survivors was 35.4°C (95% CI 34.6–36.3) and was significantly lower than in survivors (38.2°C, 95% CI 38.1–38.3) (Figure 3a). Among the survivors, the cats admitted to the ICU had a significantly lower median BT (37.9°C, range 36.9–38.7) than those admitted to a GW (38.5°C, range 37.8–39) and discharged ones (38.5°C, range 38–39) (P <0.0001). Among the non-survivors, those cats that died spontaneously had a significantly lower median BT (34°C, range 32–36.1) than the euthanased ones (36°C, range 34.3–37.5) (Figure 3b). The distribution of mortality rates in the ED based on BT is shown in Figure 4.

(a) Box plot of body temperature (°C) in survivor and non-survivor cats admitted to the emergency department. (b) Box plot of body temperature (°C) in cats admitted to the emergency department in different categories of outcome. The horizontal bars represent median values, boxes represent interquartile range and whiskers show ranges.

Graphical representation of percentage of survivor (light grey) and non-survivor (dark grey) cats admitted to the emergency department based on different body temperature categories. CHT = critical hypothermia; HT = hyperthermia; MHT = mild hypothermia; ModHT = moderate hypothermia; NT = normothermia; SHT = severe hypothermia
Based on the univariate linear regression analysis, the risk for non-survival in the ED was significantly higher in cats with a decreased BT, progressively increasing according to the severity of hypothermia (Table 1). Other variables significantly associated with higher risk of ED mortality by univariate linear regression analysis included the presence of hypotension (OR 10.86, 95% CI 6.61–17.85), lower heart rate (OR 0.98; 95% CI 0.97–0.99) and belonging to the senior category (OR 1.67, 95% CI 1.02–2.76).
Univariate binary logistic regression analysis results of body temperature categories associated with mortality in cats admitted to the emergency department

Values in parentheses are 95% confidence intervals
OR = odds ratio; RC = regression coefficient; SE = standard error
Triage BT and outcome in ICU
A total of 964 cats were hospitalised in the ICU (n = 764) and GW (n = 200). The mortality rates in the ICU and GW were 198/764 (25.9%) and 19/200 (9.5%), respectively. Spontaneous death occurred in 138/764 (18.1%) cats in the ICU and 6/200 (3%) in the GW. Lower triage BT was significantly associated with a higher frequency and risk of mortality in patients hospitalised in the ICU (Figure 5, Table 2).

Graphical representation of percentage of survivor (light grey) and non-survivor (dark grey) cats admitted to the intensive care unit based on different body temperature categories. CHT = critical hypothermia; HT = hyperthermia; MHT = mild hypothermia; ModHT = moderate hypothermia; NT = normothermia; SHT = severe hypothermia
Univariate binary logistic regression analysis results of body temperature categories associated with mortality in cats admitted to the intensive care unit

Values in parentheses are 95% confidence intervals
OR = odds ratio; RC = regression coefficient; SE = standard error
Triage BT and disease categories
In the final population, 469/1440 (32.6%) cats presented with SIRS. The no-SIRS group (n = 971, 67.4%) was further divided into urinary and cardiovascular diseases, which included 197/1440 (13.7%) and 44/1440 (3.1%) cats, respectively, and miscellanea, with 730/1440 (50.7%) cats. The most common diseases in the miscellanea group were minor trauma (n = 115/730, 15.8%), gastrointestinal diseases (n = 94/730, 12.9%), neoplasia (n = 93/730, 12.7%) and orthopaedic disorders (n = 43/730, 5.9%) (see supplementary material 1).
Cats with SIRS had significantly lower median BT value (37.1°C, range 35.5–38; P <0.0001) compared with no-SIRS cats (38.4°C, range 37.9–38.9). These data were also confirmed when the SIRS group was compared with the no-SIRS disease categories (Figure 6). The presence of SIRS upon ED admission was associated with a higher frequency and risk of non-survival (OR 4.61, 95% CI 2.98–7.12; P <0.0001) (Figure 7).

Box plot of body temperature (°C) of cats admitted to the emergency department in different disease categories. The horizontal bars represent median values, boxes represent interquartile ranges and whiskers show ranges

Graphical representation of percentage of survivor (light grey) and non-survivor (dark grey) cats admitted to the emergency department based on different disease categories. SIRS = systemic inflammatory response syndrome
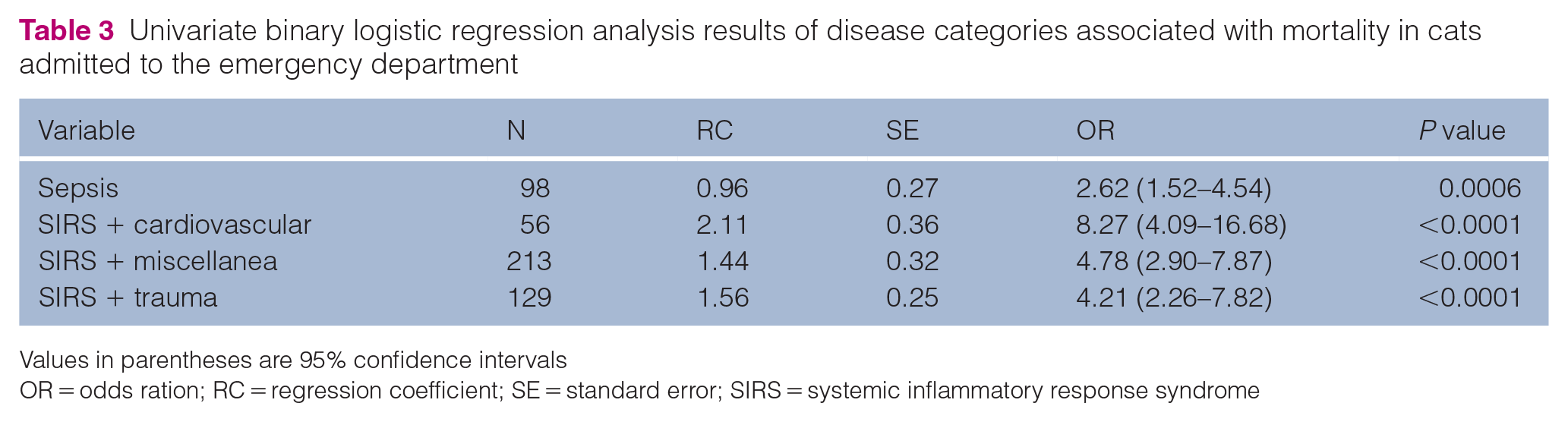
In the 469 cats with SIRS, a diagnosis of sepsis was recorded for 124 (26.4%) cats. The presence of sepsis was associated with a high prevalence of hypothermia (n = 79/124, 63.7%) and with a higher risk of non-survival (Table 3). Cats with SIRS were further categorised based on the underlying disease as SIRS-urinary (n = 78, 16.6%), SIRS-cardiovascular (n = 56, 11.9%), SIRS-trauma (n = 120, 25.6%) and SIRS-miscellanea (n = 215, 45.8%) (see supplementary material 2).
Univariate binary logistic regression analysis results of disease categories associated with mortality in cats admitted to the emergency department
Values in parentheses are 95% confidence intervals
OR = odds ration; RC = regression coefficient; SE = standard error; SIRS = systemic inflammatory response syndrome
The presence of SIRS in cats with cardiovascular disease was associated with a significantly lower median BT (36.4°C, 35–37.05; P <0.0001) and a higher risk of non-survival in ED compared to the presence of SIRS-urinary (37.2°C, 35.9–37.7), SIRS-trauma (36.8°C, 34.9–37.8) and SIRS-miscellanea (37.3°C, 36.1–39) diseases, respectively (Figure 8, Table 3).

Box plot of body temperature (°C) of cats admitted to the emergency department in different categories. The horizontal bars represent median values, boxes represent interquartile ranges and whiskers show ranges
Discussion
In this large population of cats admitted to the ED of a VUH, a lower BT was commonly reported (35.4%) and was independently associated with increased odds of 1-day mortality. Interestingly, a significantly lower BT was observed in cats that died spontaneously compared with those that were euthanased, suggesting a more severe condition in the former. Unfortunately, we could not exclude financial reasons for euthanasia other than a grave prognosis. Nonetheless, our results support the prognostic role of triage hypothermia in feline patients and confirm the association of this condition with the alteration of body homeostasis and severe systemic compromise. 15 Indeed, decreased responsiveness of alpha 2 adrenergic receptors was described in both dogs and cats with decreasing core temperatures. 10 Moreover, untreated low BT, especially when the core BT falls below 34°C, can cause severe multiorgan deterioration characterised by cardiovascular, respiratory, neurological and metabolic dysfunctions and was potentially associated with mortality in critically ill patients.10,15,18–20
Most of the clinical signs observed in the ED are significantly associated with 1-day mortality, 30-day mortality and ICU admission in humans. 2 Interestingly, however, the same triage level is not associated with the same odds for death with respect to the individual clinical sign including BT. 2 Indeed, triage hypothermia is independently associated with mortality despite a low prevalence of non-accidental hypothermia reported as a cause for admission to ED in humans.8,9 Similarly, hypotension and decreased HR were independently associated with a higher risk of 1-day mortality in our population, confirming the prognostic significance of the shock triad (hypothermia, hypotension and bradycardia) in cats admitted to the ED. 15 Decreased depolarisation of cardiac pacemaker cells and baroceptor stimulation of vagal fibres in response to inadequate arterial stretch might justify this hypodynamic state and the frequent absence of a compensatory response in cats with shock. 21
Triage hypothermia in humans has even been associated with major odds of ICU and hospital mortality compared with normothermia.2,3 Lower BT in cats admitted to the ED in our study was significantly associated with a higher rate of ICU hospitalisation compared with GW admission, and a higher risk of ICU mortality. Owing to its great discriminant capacity, BT had already been incorporated into the 5- and 8-variable feline APPLE score to stratify illness severity in hospitalised cats. 22 However, because of the retrospective nature of the study, we were not able to evaluate the outcome prediction performance of the feline APPLE score in our population. Moreover, we recorded only a single BT measurement upon ED admission in this study, precluding the serial monitoring of changes in BT during ICU hospitalisation.
Non-accidental or secondary hypothermia in cats is frequently associated with specific diseases or syndromes, including trauma, congestive heart failure, AKI and sepsis.12,13,23 Thus, triage hypothermia might further help in the diagnostic approach to the critical care feline patient.
In humans, triage hypothermia was frequently reported as the unique clinical sign abnormality and was independently associated with mortality in septic adult and paediatric patients. 9 However, a low prevalence of hypothermia is reported in human patients with severe sepsis or septic shock. 24
In our population, the presence of SIRS was associated with significantly lower BT and higher odds of non-survival compared with the absence of SIRS and presence of other diseases. Moreover, a diagnosis of sepsis was associated with a high incidence of hypothermia and was independently associated with a higher risk of non-survival. These results confirm that cats might be more predisposed to develop hypothermia than humans in response to sepsis. 15 It remains unclear whether hypothermia simply represents a clinical manifestation of severe inflammation or shock, or whether hypothermia itself drives mortality through a still unknown mechanism. 25 In septic humans, cardiovascular dysfunction and endothelium injury might contribute to hypothermia development. 26 In this regard, feline patients could be more susceptible to developing hypothermia during shock owing to their intrinsic characteristics, such as a low blood volume:body mass ratio and a high surface area:body mass ratio, which promotes greater heat loss.11–14 Thus, early identification and treatment of hypothermia might be crucial for managing septic cats.
Similarly, a worse prognosis and lower BT upon admission were reported in a subgroup of our cats with SIRS secondary to trauma. Hypothermia on triage is frequently reported in cats with trauma and its prognostic significance has been recently documented in other studies,13,14 supporting the validity of the present findings. Thus, implementing active rewarming as a priority measure for cats presenting to the ED with hypothermia might improve outcomes in this setting, as has been reported in humans.27,28
Furthermore, once the cats included in our study and classified as SIRS were subgrouped according to a concomitant diagnosis of cardiovascular or urinary diseases, a significantly lower BT and worse prognosis were observed compared with cats affected by the same diseases without the presence of systemic inflammation. Interestingly, the lowest BT and the highest risk of mortality were observed in cats with SIRS that also had cardiovascular disease. 23 Hypothermia and congestive heart failure are frequently associated in cats and a lower BT upon admission is commonly reported in non-survivors.21,23 Hypothermia has already been reported in humans as a marker of heart failure or advanced cardiac disease, contributing to a worse prognosis. 29 Because of the nature of our study, we were unable to perform staging and grading of the severity and chronicity of cardiovascular disease or assess the overall severity of critical illness in the enrolled cats. Thus, we were not able to determine the real impact of hypothermia, systemic inflammation and cardiovascular disease on the final outcome of these subgroups of patients. Further prospective studies focusing on confirming the latter findings in cats with cardiovascular diseases complicated by systemic inflammation are warranted. Similar considerations may apply to the data distribution of BT and outcomes in cats affected by urinary disease in our population, where the incidence and prognostic significance of hypothermia confirmed the findings from previous studies. Indeed, the role of the kidney in thermoregulation is well described in the literature, with hypothermia being a prevalent phenomenon associated with feline uremia. 11 Furthermore, BT was able to predict survival in cats with AKI. 12 Unfortunately, owing to the retrospective design of our study, we could not apply the International Renal Interest Society (IRIS) grading or staging system for AKI and chronic kidney disease, respectively, in enrolled cats with urinary diseases. For the same reason, no additional characterisation of pre-renal, renal or post-renal kidney injury was possible. Thus, we should consider that animals with minimal or no renal involvement could have been included in this category, affecting the overall interpretation of the role of BT and kidney dysfunction in the final outcome.
The present study has other limitations. This is a single-centre study conducted at a VUH offering a 24 h of emergency service and primary care. Thus, the overall population of cats admitted to the ED and included in the present study might not necessarily be comparable to feline populations included in other studies where higher mortality rates were reported. 30 Moreover, in our hospital, the criteria for admission to the ICU are mainly clinician dependent, creating a potential bias in the inclusion of critical care patients in the ICU group of the present study. The use of a scoring system for illness severity would have limited this discrepancy in data comparison. Furthermore, the retrospective design of the study might have limited a complete collection of the data needed for a definitive diagnosis. Thus, we cannot exclude a misclassification of cats in the selected disease categories, and we had to include an elevated number of cats in a heterogeneous group of diseases defined as miscellanea. The criteria to define feline SIRS were adopted from the veterinary literature, and no additional laboratory aid (eg, acute phase proteins) was used to effectively support the presence of systemic inflammation. Moreover, these criteria partially overlapped those used to classify hypothermia and hyperthermia in our study, 15 which may have affected the association between SIRS and changes in BT.
Conclusions
Hypothermia is common in cats presented to the ED, and the odds of non-survival increases progressively with the reduction of triage BT. The association of hypothermia with SIRS and sepsis, along with its correlation to a worse prognosis, might identify it as a possible early sign of shock and systemic derangement; thus, triage BT could serve as a potential screening tool to identify the most critical patients requiring urgent medical care, including active rewarming techniques. Furthermore, the association of triage hypothermia with specific comorbidities, such as cardiovascular or kidney diseases, might guide early screening and diagnostic protocols upon the patient’s admission to hospital. Finally, future prospective studies focusing on specific disease populations, such as sepsis and septic shock, are needed to confirm the predictive value of triage hypothermia for 1-day and overall hospital mortality in cats.
Supplemental Material
sj-docx-1-jfm-10.1177_1098612X241291295 – Supplemental material for Triage body temperature predicts outcome in cats at emergency department admission: a retrospective study of 1440 cases (January 2018 to December 2021)
Supplementary material 1: The most common diseases in the no-SIRS miscellanea group.
Supplemental Material
sj-docx-2-jfm-10.1177_1098612X241291295 – Supplemental material for Triage body temperature predicts outcome in cats at emergency department admission: a retrospective study of 1440 cases (January 2018 to December 2021)
Supplementary material 2: The most common diseases in the SIRS miscellanea group.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The following files are available as supplementary material:
Supplementary material 1: The most common diseases in the no-SIRS miscellanea group.
Supplementary material 2: The most common diseases in the SIRS miscellanea group.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.