
Abstract
Objective
To reveal the value of single lymphocyte subpopulation and their ratios in the progression of sepsis.
Methods
From January 2019 to March 2021, 39 sepsis patients, 16 septic shock patients, and 50 healthy volunteers were recruited in the Second Xiangya Hospital for this cross-sectional study. The absolute quantitation of CD4+T, CD8+T, B lymphocytes, and NK cells in peripheral blood were determined by flow cytometry. SPSS Software was used to analyze the results.
Results
On the whole, the numbers of lymphocytes in the sepsis group and in the septic shock group were lower than that in the healthy control group. Surprisingly, the percentage of CD8+T lymphocytes in the septic shock group was slightly higher than that in the sepsis group. The percentage of B lymphocytes in the sepsis group was higher than that in the healthy control group. The AUC of CD8+T/B was 0.724, with the sensitivity and specificity being 75.00% and 71.79%, respectively.
Conclusion
The immune expression pattern of patients with sepsis was not a simple decrease in the number of lymphocytes. The change in the ratios of lymphocyte subpopulation might be more meaningful along the development and progression of sepsis. The ratio of CD8+T/B could be used to diagnose the progression of sepsis and reduce the misdiagnosis rate to a certain extent.
Introduction
Sepsis is a systemic inflammatory response syndrome caused by infection, a common complication after severe infection, trauma, burn, shock, and major surgery, with a mortality rate of 30%–70%. 1 Meanwhile, it is the main cause of death among Intensive Care Unit (ICU) patients. 2 Its mechanism is related to immune dysfunction, infection, and secretion of inflammatory factors. The imbalance of the homeostasis of pro-inflammatory and anti-pro-inflammatory responses plays an important role in this process.3,4 The natural course of sepsis might be a transition from an early period of pro-inflammatory response to a prolonged period of immunosuppression. As a result of improved treatment, the death rate of sepsis has been significantly reduced. However, with the increased risk of secondary and nosocomial infections which have become a significant risk of late mortality, 5 this situation leads to up to 90% of patients dying from multiple organ failure caused by impaired immune cell function and insufficient tissue perfusion. 6 Immunosuppression and functional impairment of immune cells play prominent roles in the development and progression of sepsis. Clinicians usually need to apply different treatments according to the severity of the patient’s condition. Generally, the severity of the patient’s condition is determined according to the acute physiology and Chronic Health Assessment II (Apache-II). Still, Apache-II requires a certain amount of time and is unable to reflect and update the condition in real time. 7 By measuring peripheral blood lymphocyte subpopulation, the immune state of patients can be effectively indicated. Peripheral blood lymphocyte subpopulation analysis has become an essential tool to assess immune status and pathological diagnosis, 8 which also plays a crucial role in evaluating the immune status of sepsis. However, the results of many studies were inconsistent. Hence, there is no exclusive conclusion that has been drawn out.9–11
In addition, many studies have investigated the epidemiological characteristics of sepsis in black and white races,12–14 but sepsis patients in developing countries, including China, are still poorly described. Therefore, it is imperative to identify an indicator to reflect the host’s immune status in time. This paper described the immune status and progress of sepsis patients in a major teaching hospital in central China. Further, it revealed the changes and diagnostic value of different lymphocyte subsets and their ratios in patients with sepsis and septic shock, and would bring inspiration to clinical treatment and health management.
Materials and methods
Subjects
Basic information about subjects in patients and control groups.

Collection and detection of peripheral blood
Five milliliters of blood was collected using EDTA-K2 anticoagulant vacuum blood vessel and detected within 6 h. The absolute quantitation of CD4+T lymphocytes, CD8+T lymphocytes, B lymphocytes, and NK cells in peripheral blood were carried out by flow cytometry. Serum PCT and CRP were detected by Roche cobasE411 electrochemiluminescence analyzer (Roche, Switzerland). WBC was detected by SYSMEX-XN hematology analyzer (SYSMEX, Japan). Absolute quantification of cell subpopulation was determined by flow cytometry (BD, USA) according to the manufacturer’s protocol.
Statistical analysis
The data was tested to be non-normal distribution, and the median (Q1, Q3) was used to describe the data. The differences between PCT, CRP, WBC, CD4+T, CD8+ B lymphocytes, and NK cells and their ratios among all groups were compared. All ratios were obtained by dividing the absolute number of cells in the two groups by flow cytometry. The AUC and ROC of each variable were further calculated and analyzed. SPSS Software (SPSS, Inc., Chicago, IL, USA) was used to analyze the results. Comparison between two groups was analyzed by Mann–Whitney U test, and Kruskal–Wallis H test was used to test three or more groups. p < 0.05 was considered statistically significant.
Results
Clinical and laboratory characteristics of subjects
A total of 39, 16, and 50 patients were recruited for the sepsis group, septic shock group, and the healthy control group, respectively. There was no statistically significant difference in age between the groups. There was no significant difference in mechanical ventilation, surgical treatment, or ICU stay between the sepsis group and the septic shock group. Overall, the majority of patients had primary infection sites in the lungs (26/45 (57.8%), followed by gastrointestinal tract (7/45, 15.6%). Among the pathogens, fungi (n = 5) and viruses (n = 2, influenza B virus and Epstein2Barr virus) accounted for a small number, while Acinetobacter baumannii was mostly common. The basic clinical information of all subjects was recorded in Table 1.
As shown in Figure 1 and Table 2, T lymphocytes (quantities) (p < 0.001), CD4+T lymphocytes (quantities) (p = 0.007), CD8+T lymphocytes (quantities) (p < 0.001), CD8+T lymphocytes (%) (p = 0.001), NK cells (%) (p = 0.002), and NK cells (quantities) (p < 0.001) in the sepsis group were lower than those in the healthy controls; T lymphocytes (quantities) (p = 0.011), CD4+T lymphocytes (quantities) (p = 0.001), NK cells (%) (p = 0.028), and NK cells (quantities) (p < 0.001) in the septic shock group were significantly lower than those in the healthy controls. B lymphocytes (%) in the sepsis group were significantly higher than those in the healthy control group (p = 0.016) and the septic shock group (p = 0.039). CD8+T lymphocytes (%) in the sepsis group was significantly lower than those in the healthy control group (p = 0.012) and in the septic shock group (p = 0.004). Comparison of single lymphocyte subpopulation in peripheral blood of each group. The data were averaged and tested by Mann–Whitney U test. * indicated that the difference between the two groups was statistically significant (p < 0.05). Frequency description of immune parameters.

The value of single indicators and ratios in the diagnosis of sepsis
Area under ROC curve of each indicator for the diagnosis of sepsis.

Comparison of the cut-off value, sensitivity and specificity of sepsis diagnosed by each variable.


ROC curves for the diagnosis of sepsis for all variables. Left: single indicator of lymphocyte subpopulation, right: lymphocyte subsets ratios.
The value of single indicators and ratios in the diagnosis of septic shock
The values of PCT (ng/mL), CRP (mg/L), and WBC (×10^9) in the sepsis group and septic shock group were 12.80 ± 25.01, 101.35 ± 101.10, 10.62 ± 5.76; 20.46 ± 31.45, 131.50 ± 85.47, 15.63 ± 8.53, respectively. PCT (p = 0.153), CRP (p = 0.136), and WBC (p = 0.109) implied no statistical difference between the two groups.
Area under ROC curve of each indicator for the diagnosis of septic shock.

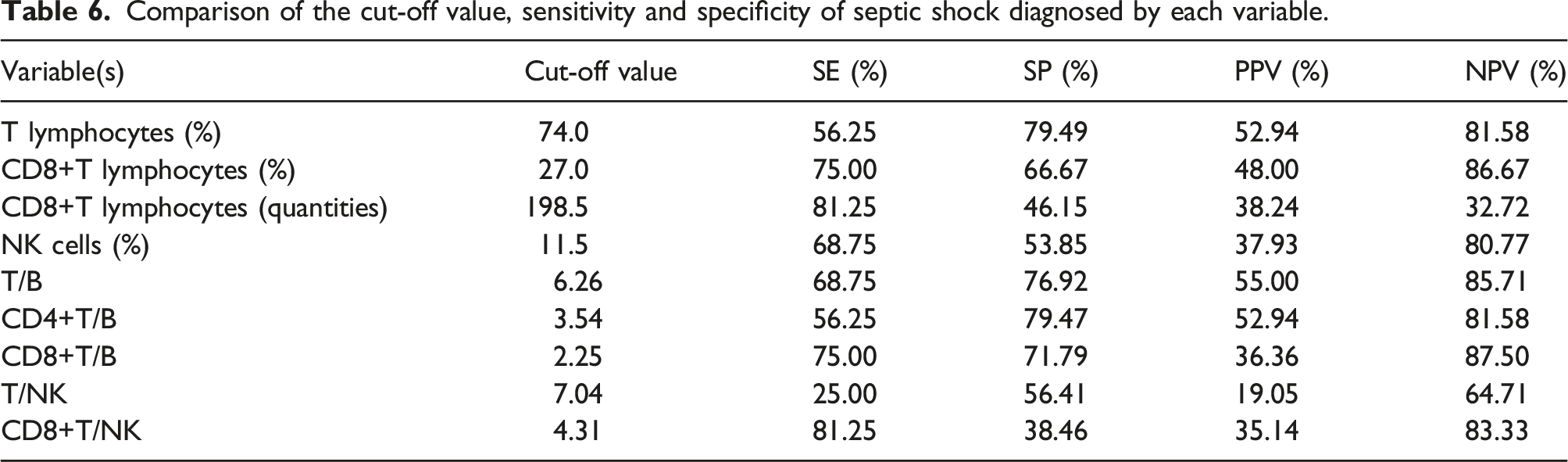
Comparison of the cut-off value, sensitivity and specificity of septic shock diagnosed by each variable.

ROC curves for the diagnosis of septic shock for all variables. Left: single indicator of lymphocyte subpopulation, right: lymphocyte subsets ratios.
Discussion
The primary lesion of patients was mainly lung (57.8%) in this research, and similar results have been found in other studies,19,20 which suggested that clinicians should be aware of the importance of preventing patients with pulmonary infection from deteriorating to sepsis. Our results also showed that the septic shock group was older than the sepsis group. In addition to primary lesion, age and an increased burden of chronic health conditions are also important risk factors for severe sepsis. Previous research displayed that half of septic shock cases occur in people over 65 years of age. 21 Elder population tend to bear more chronic health problems. With the burden of various chronic diseases and underlying genetic factors, they may suffer more complex conditions of sepsis compared to younger people. 12
Lymphocyte is the most basic and essential group of immune cells involved in the immune response of sepsis, and the number of lymphocyte subgroups can directly reflect the immune status of patients. 22 Since immune response is highly dynamic, understanding the variability of lymphocyte’s number and function in sepsis will contribute to developing novel, personalized treatments for sepsis. The main reason of chronic immune paralysis in sepsis patients lies in the impaired T cell response in the host’s environment after sepsis. 19 This research showed that the numbers of T lymphocytes in the septic shock group and in the sepsis group were significantly lower than that in the healthy control group (Figure 1). The numbers of CD4+T cells in the septic shock group and in the sepsis group were significantly lower than that in the healthy control group (Figure 1), and the absolute values of CD4+T cells in the three groups decreased successively. Other studies had also proved that CD4+T cells were the most severely infected subgroup in patients with sepsis.23–27 The number and the ratio of CD8+T cells in the sepsis group were significantly lower than those in the healthy control group (Figure 1), which was consistent with most research results.28,29 However, our research results indicated that the percentage of CD8+ T in the septic shock group was slightly higher than that in the sepsis group (Figure 1). In addition to the decrease of the T lymphocytes number, T lymphocytes dysfunction is also the cause of the failure to eliminate pathogens, as well as the increased mortality and hospital-acquired infections during sepsis. Our study found that in the initial stage of sepsis, there might be a decrease in the number of lymphocytes. As the disease progresses, persistent antigen reactivation could further impair CD8+T cell function. CD8+T cells gradually lost the potential to proliferate or produce effector cytokines, and the expression of coinhibitory receptors PD-1, TIM-3, and LAG-3 gradually increased,30–35 resulting in the continuous deterioration of the disease.
This research indicated that the percentage of B lymphocytes in the sepsis group was higher than those in the healthy control group and in the septic shock group (Figure 4). In the early stage of infection, B lymphocytes would be activated by antigen stimulation and greatly increase in the sepsis group; thus, the percentage of B lymphocytes in the sepsis group would increase. In addition, B lymphocytes may show “depletion” like T lymphocytes under continuous antigen stimulation. A study supported that sepsis resulted in a decrease in naive B cells and an increase in immature B cells,
36
which explained the decrease in the percentage of B lymphocytes in the septic shock group. Some other studies had shown that patients recovering from invasive pneumococcal infection presented defective B cell activation,
37
impaired bacterial clearance, and reduced survival in B cell deficient mice model of septic peritonitis.38,39 Therefore, not only the decrease in number of B cells, but also the accumulation of depleted B cells might contribute to immunosuppression in sepsis. It is suggested that the reduction of immunoactive B cells and their impaired function are related to immunosuppression, whereas the mechanism behind these fundamental immune changes needs to be further explored. The absolute number and percentage of NK cells in the sepsis group and the septic shock group were lower than those in the healthy control group (Figure 1). Persistent NK cell dysfunction was closely related to sepsis induced immunosuppression, making patients more prone to secondary infection or latent virus reactivation and leading to poorerprognosis.40,41 This also explained the sequential decrease in the absolute values of NK cells in the three groups. Comparison of the proportion of peripheral blood lymphocyte subpopulation in each group. The data were averaged and tested by Mann–Whitney U test. * indicated that the difference between the two groups was statistically significant (p < 0.05).
PCT, WBC, and CRP are the most used indicators for clinical laboratory diagnosis of infection. 42 In our study, the differences of these three items between the sepsis group and septic shock group were not statistically significant, which may be related to the nature of these indicators. When the organism is damaged by trauma, infection, and tumor, CRP increases sharply within several hours, so as PCT level 43 and WBC counting, 44 which are endowed with great practical value in the early diagnosis of infection. Their diagnostic value was dramatically reduced once infection progresses, while lymphocyte subpopulation played a unique role in the diagnosis of sepsis progression.
Interestingly, there were no statistically significant differences in individual peripheral blood lymphocyte subsets among the three groups. However, when we compared the ratios of two indicators, there were significant statistical differences, as shown in Figure 1 and Figure 4. This might be attributed to a complex network of immune regulation. Moreover, the combination of two indicators could better reflect the state of organism than a single indicator.
The results implied that lymphocyte subpopulation was unsatisfactory in the diagnosis of sepsis, while they showed unique value in the diagnosis of sepsis progression (Figures 2 and 3 and Tables 3 and 5). The AUC of CD8+T lymphocytes (%) was 0.740, and the sensitivity and specificity were 75.00% and 66.67%, respectively, better than other indicators. The concept of ratio as a laboratory test was interesting, and studies had demonstrated the irreplaceable value of CD4/CD8 in reflecting the immune status of the host organism, where there is a need for preventing lung cancer, 45 diagnosing coronary artery disease (CAD) 46 and ocular sarcoidosis, 47 and evaluating the efficacy of antiretroviral therapy (ART). 48 However, the CD4/CD8 had not shown superior value in the diagnosis of sepsis and its progression. 49 The value of the ratio of the two indicators may be superior to the change of the single indicator to some extent. Therefore, we considered whether the ratios of T cells to NK or B cells could be new indicators to revolutionize the significance of lymphocyte subpopulation for sepsis. The AUC of CD8+T/B was 0.724, with favorable diagnostic efficiency (sensitivity, 75.00%; specificity, 71.79%), better than CD8+T lymphocytes (%), which reduced the misdiagnosis probability in some respects, and the increase of misdiagnosis rate might lead to antibiotics abuse.
In general, the results of this study suggested that laboratory single lymphocyte subpopulation is not sufficient to diagnose or monitor sepsis and septic shock. Nevertheless, the ratio of CD8+T/B showed high diagnostic value, which could be not only used to detect the progress of sepsis, but also to assess the curative effect of clinical therapies. The value of two indicators in assessing immune status was higher than that of a single indicator. When analyzing disease progression, clinical workers should take a comprehensive view and combine the analysis with multiple indicators. More attention should be paid to the value of the concept of ratio in lymphocyte subsets analysis.
However, this study had some limitations. First, this study was a single-center study that could only reflect the situation in the studied area. More extensive studies were needed to confirm whether these indicators would be valuable among different populations and in different regions. Secondly, sepsis patients (both ICU and non-ICU patients) were included in this study to address the lack of diagnostic indicators of sepsis progression in clinical practice and to prompt clinicians to take appropriate measures or interventions. On this basis, healthy volunteers were recruited as controls, and the inclusion criteria of this study were strictly designed. This research excluded blood system diseases, chronic irreversible diseases, tumors, immune defects, transplants, mental illnesses, and other diseases that significantly impacted the immune system, which ultimately resulted in a smaller sample size. However, the outcome of sepsis patients treated in ICU was not the primary focus of this study. It is expected of the clinician to identify characteristics that differ between infected ICU patients and non-infected ICU patients. This research provides a reference for this goal, but further work needs to be performed to analyze changes in lymphocyte subsets and their ratios in the pure ICU population. In addition, the clinical diagnosis of patients was done by experienced clinicians in the Second Xiangya Hospital following Sepsis-3, which might be affected by changes in clinical practice.
Conclusion
Altogether, the immune expression pattern of patients with sepsis was not a simple decrease in the number of lymphocytes, as the change in the function ratio of lymphocyte subpopulation might be more critical in the development and progression of sepsis. Laboratory measurement of single lymphocyte subpopulation was not recommended to diagnose or monitor the diagnosis of sepsis. CD8+T/B ratio could be useful to diagnose the progression of sepsis and reduce misdiagnosis rate to a certain extent, which was expected to be applied to guide clinical medication. It was more important to observe the overall variability of lymphocyte subpopulation in immune responses than to observe changes in individual cell populations.
Footnotes
Author contribution
YP: Writing - Original Draft, Methodology, Software, performed the sample collection, performed the sample analysis, XW: Writing - Original Draft, Software, Data Curation, YP and XW have the same contribution, SY: Writing - Review and Editing, MW: Conceptualization.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from * The Institutional Review Committee/Ethics Committee of The Second Xiangya Hospital of Central South University (APPROVAL NUMBER: XYEYY2021146).
Informed consent
Informed consent was not sought for the present study because * This study conforms to the no-informed consent procedure of the institutional Review Committee/ethics committee of the Second Xiangya Hospital of Central South University and has passed the ethical review. In this study, medical records obtained from previous clinical diagnosis and treatment were used to conduct the study, which was in line with the minimum risk. It does not involve additional blood and other human specimen collection and does not pose any risk to patients. In addition, all patients will be de-identified without disclosing the privacy of the subjects, and the exemption of informed consent will not adversely affect the rights and health of the subjects. In general, the institutional Review Committee/Ethics Committee of The Second Xiangya Hospital of Central South University did not require informed consent of patients for this study.*