
Abstract
Case series summary
A total of 13 cases of cats with a caudal mandibular fracture treated with a novel surgical technique using the Ramus Anatomical Plate system were reviewed. Preoperative, immediate postoperative and a minimum of 8 weeks postoperative CT images were required as inclusion criteria. The outcome and complications were determined from clinical data and radiographic follow-up examinations. All cases achieved adequate anatomical reduction, resulting in a functional and atraumatic occlusion postoperatively. No intraoperative complications were reported. Time to voluntary food intake was in the range of 1–25 days. No evidence of disruptions to the implants or screw loosening was observed in the 8-week postoperative CT imaging, with radiographic evidence of complete osseous union in all fractures. The most common postoperative complication was swelling at the surgical site. Two cats had postoperative exophthalmos due to retrobulbar haemorrhage, and one cat exhibited partial wound dehiscence 5 days postoperatively, which resolved with medical management. Longer-term complications included intraoral plate exposure in one cat, which required plate removal 10 months postoperatively.
Relevance and novel information
In this case series, rigid internal fixation of caudal mandibular fractures using the Ramus Anatomical Plate osteosynthesis system was associated with a minimal complication rate, and satisfactory radiographic and clinical outcomes. The reported outcomes of this novel technique are favourable when compared with previous techniques described for the management of these fracture types.
Introduction
Mandibular fractures in cats are reported to represent 14.5% of all feline fractures, most commonly caused by road traffic accidents, falling from a height or a bite from another animal. 1 A recent study on fracture distribution of craniomaxillofacial trauma in cats has reported the caudal mandibular region as the most commonly affected, defined as the region including the ramus of the mandible (including the coronoid process), the angular process, the neck of the condyle and the condylar head. 2 Accurate anatomical reconstruction of caudal fractures is required to restore normal occlusion and pain-free function, with as little as 2 mm of malalignment preventing the jaw from closing or resulting in temporomandibular joint osteoarthritis. 3
Maxillomandibular fixation (MMF) techniques are commonly employed to manage feline caudal mandibular fractures.3–7 Complications associated with these techniques include difficulty with thermoregulation, long periods of assisted feeding due to slow functional recovery, and an increased risk of aspiration of food or regurgitated stomach contents.3–5 They are contraindicated in patients with nausea, gastric reflux or obstructive airway disease, and carry a high postoperative morbidity rate. 8
Open reduction and internal rigid fixation (ORIF) with titanium miniplates is the standard of care in humans for the treatment of caudal mandibular fractures.9,10 This technique provides accurate fracture reduction to restore anatomical relationships, good fracture fixation to provide stability, an early and safe return to function, and easier maintenance of the patient’s airway and oral hygiene, with improved nutrition. 11 In veterinary maxillofacial surgery, internal rigid fixation with miniplates for the treatment of caudal mandibular fractures in cats has been less commonly reported.12–16 This may be due to the challenges of surgical access, the small surface area and thin bone, and the need for complex contouring of implants due to the curved topography of this area. Similar difficulties with exposure, small size of fragments and maintaining bone fragment stability have been overcome in human condylar neck and subcondylar fractures using techniques such as preoperative plate contouring using three-dimensional models and the development of standardised three-dimensional anatomical plates, which provide precise adaptation to the area of implantation. 17 The development of these specialised osteosynthesis systems has been possible due to the consistency of morphology of this area between different people, and between the two sides of the mandible in an individual. 18 Three-dimensional osteometric analysis studies have shown that there is a high level of consistency in the dimensions of mandibles between cats. 19 This has enabled the development of novel pre-printed miniplates to provide internal rigid fixation of feline caudal mandibular fractures. 20
The aim of this paper was to describe a new technique and report the outcomes of internal rigid fixation in the treatment of caudal mandibular fractures in cats, using a specialised osteosynthesis system: the Ramus Anatomical Plate (RAP; Fusion Implants).
Case series description
Development of the Ramus Anatomical Plate
Plate design was performed by the School of Engineering at the University of Liverpool in 2018. 20 Three-dimensional images from CT scans of 32 feline intact mandibles were used to design a plate shape with a curved profile to match the surface topography of the anatomical area, and with ideal screw placement in areas of greater bone thickness at the rostral and caudal borders of the ramus and in the ventrolateral mandibular body. The CT images were also used to produce three groups based on clusters of ramus height (small: 24.50–26.50 mm, median 25.52 mm; medium: 26.85–28.93 mm, median 27.84 mm; large: 29.42–31.24 mm, median 29.78 mm), resulting in the development of ‘small’, medium’ and ‘large’ plates (Figure 1). A three-dimensional digital model fracture analysis, from clinical cases of feline caudal mandibular fractures, was then performed to both refine the design and assess whether the plate would effectively fix the bone fragments, providing enough screw options to stabilise each piece of bone (Figure 2).

Ramus Anatomical Plate design available in right and left configurations, and in sizes small, medium and large

Lateral fracture lines from reconstructions plotted over the Ramus Anatomical Plate design. Reproduced from Sage J et al.
Plates have a thin profile of 1.2 mm, and screw holes are designed to be used with 1.5 mm cortical screws. The material selected for the product is titanium alloy Ti-6Al-4V due to its low elastic modulus/high deformability, superior biocompatibility and enhanced corrosion resistance. 21 The plates are available in two mirror-image forms: one designed and contoured for the right caudal mandible and the other for the left (Figure 1).
Case inclusion criteria
The medical records of cats that presented to the Dentistry and Oral Surgery Department at Eastcott Referrals, Swindon, UK, part of Linnaeus Veterinary, between March 2019 and September 2023 were reviewed. The inclusion criteria were the presence of a caudal mandibular fracture, treatment with the RAP osteosynthesis system and the availability of preoperative, immediate postoperative and a minimum of 8 weeks postoperative CT images. Data including signalment, body weight, the inciting trauma, description of the fracture, concurrent injuries, size of plate used and number of screws placed were recorded for each patient. The outcome and complications were determined from clinical data and radiographic follow-up examinations.
Surgical preparation and technique
The diagnosis of a caudal mandibular fracture was based on clinical examination and CT scan findings. The preoperative CT scan of each cat was used to print a mirror-image three-dimensional model of the contralateral healthy mandible, using an Ultimaker S3 three-dimensional printer with polylactic acid filament. Using measurements taken from CT images, fracture lines were drawn on to the printed model. The size of plate (small, medium or large) was then selected by identification of the most appropriate to most closely match the contours of the three-dimensional model (Figure 3). Screw hole location was also compared with the fracture configuration on the model to ensure that at least three screws could be placed in each fracture fragment. After plate selection, a minor contouring adjustment was performed, if required, for the individual patient. The three-dimensional printed model was sterilised for use as a template during surgery.
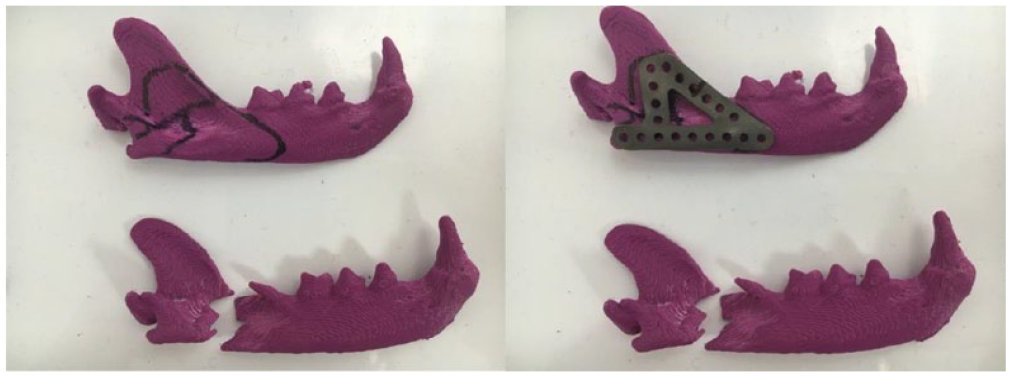
Mirror-image three-dimensional model of the contralateral healthy mandible (top) used to preoperatively select the most appropriate plate size, check plate contouring and ensure appropriate screw placement
Anaesthetic protocols consisted of premedication with methadone (Comfortan; Dechra) 0.2 mg/kg IV, medetomidine (Sedator; Dechra) 0.005 mg/kg IV and ketamine (Narketan; Vetoquinol) 0.5 mg/kg IV. General anaesthesia was induced with either alfaxalone (Alfaxan; Zoetis) or propofol (Propoflo Plus; Zoetis) given intravenously to effect to facilitate successful tracheal intubation. Maintenance of anaesthesia was via isoflurane (Isoflo; Zoetis) vaporised in 100% oxygen and delivered by a correct-sized non-rebreathing system. Once the depth of anaesthesia was appropriate, a transmylohyoid intubation was performed to allow intraoperative evaluation and accurate positioning of occlusion during surgery. Locoregional anaesthesia was performed via an ultrasound-guided trigeminal nerve block with bupivacaine 0.5% (Marcain; AstraZeneca). A constant-rate infusion of ketamine 0.01 mg/kg/min was given intraoperatively, with intravenous doses of cefuroxime (Zinacef; GlaxoSmithKline) 20 mg/kg or amoxicillin-clavulanic acid (Augmentin; GlaxoSmithKline) 20 mg/kg administered 30 mins before the start of surgery and repeated every 90 mins until the completion of all surgical procedures. All patients had an oesophageal feeding tube placed either at the time of the preoperative CT or postoperatively.
Cats were positioned for surgery in lateral recumbency with the fractured mandible uppermost. Hair was clipped and the skin was aseptically prepared over both mandibles and the ipsilateral maxilla, masseteric, zygomatic, periorbital and temporal regions. The oral cavity was rinsed with a 0.12% chlorhexidine solution (Hexarinse; Virbac). An extraoral ventrolateral surgical approach to the caudal part of the body and the ramus of the mandible was made through the skin and subcutaneous layers, often involving an incision through the attachment of the digastricus muscle and the buccinator muscle. The masseter muscle was elevated from its insertion on the ventral border of the mandible, or a partial masseterotomy was performed, depending upon fracture location, to enable exposure. If the fracture could be reduced, the plate was positioned to check that the size and contouring had been adequately determined from the three-dimensional model. When the fracture could not be easily reduced due to the small size of fragments, or due to the comminuted nature of the fracture, the pre-selected plate was used as a guide to manipulate the fragments and anatomically reduce the fracture in alignment with the contours of the plate. The plate was held in position with bone-holding forceps, pilot holes were drilled using a 1.1 mm drill bit and 1.5 mm cortical screws were placed in as many holes as possible to complete fixation of the plate (at least three screws in each fracture fragment) (Figure 4). Screw lengths 1 mm greater than the measurements identified by use of a depth gauge were selected. This length was selected to avoid perforation of the oral mucosa on the lingual aspect of the mandible, due to the minimal soft tissue covering this area of the ramus. The surgical site was closed in three layers with simple interrupted 4-0 Glycomer 631 (Biosyn; Ethicon) sutures in the masseter and 4-0 poliglecaprone 25 (Monocryl; Ethicon) subcutaneous and intradermal sutures. Immediate postoperative CT imaging was performed to assess the accuracy of the reduction and position of the screws, and the occlusion was checked before recovery from anaesthesia (Figure 5).

Intraoperative photographs from two cases showing plate positioning and screw placement

Immediate postoperative CT images from case 5
Postoperative care
All cats received a combination of methadone (Comfortan; Dechra) 0.1–0.2 mg/kg IV or buprenorphine (Bupracare; Animalcare) 0.02 mg/kg IV, and meloxicam (Metacam; Boehringer Ingelheim) 0.05 mg/kg via the feeding tube while hospitalised, with the meloxicam continued orally for approximately 4 weeks after surgery once discharged. Additional analgesics were provided based upon the individual patient’s requirements. All patients were fed via an oesophagostomy tube until they were voluntarily eating their full resting energy requirements. Owners were advised to confine the cats indoors for 8 weeks, and to offer only soft food. It was recommended that toys and chewing on hard objects be restricted for 6–8 weeks.
Outcome
Follow-up examinations were performed at a minimum of 8 weeks postoperatively, and in all cases, CT imaging was carried out. The images were evaluated for radiographic evidence of implant failure (eg, screw loosening or plate failure) and fracture healing with evidence of increased bone mineral density and bridging callus across the fracture lines. The clinical parameters assessed included occlusion, range of motion of mouth opening and any evidence of chronic infection. Additional assessments were also undertaken dependent upon patient progress or complications.
Results
A total of 13 cats met the inclusion criteria. Summary data for the cats are provided in Table 1. Breeds included 11 domestic shorthairs, one Bengal and one Maine Coon (age range 1–12 years; body weight range 3.1–9 kg). There were eight male cats and five female cats, and all were neutered. The pathogenesis of fractures included vehicular trauma (n=9), dog bite trauma (n = 2), a fall indoors (n = 1) and unknown (n = 1). All caudal mandibular fractures were associated with other craniomaxillofacial injuries, including maxillary/mandibular symphyseal separation (n = 11), dentoalveolar trauma (n = 8), nasopharynx/maxillary/nasal/orbital fractures (n = 5), mandibular condylar fractures (n = 5), temporomandibular joint subluxation (n = 3), degloving injuries (n=3), tongue laceration (n = 1) and ocular trauma (n=2). Distant comorbidities resulting from trauma included brachial plexus injury (n = 1), pneumomediastinum (n = 1), perineal swelling (n = 1) and hindlimb digit laceration with nail avulsion (n = 1). The size of RAP used in cats included small (n = 6), medium (n = 5) and large (n = 2). Seven right plates and six left plates were used. A range of 7–11 screws was used. No intraoperative complications were encountered in any patient. Occlusion was functional and atraumatic in all but one case postoperatively, thought to be a result of a concurrent temporomandibular joint subluxation. Assessment of immediate postoperative CT scans revealed anatomical reduction with no screw placement concerns in all 13 patients. The number of days until patients were eating postoperatively was in the range of 1–25 days.
Data summary for 13 cats with a caudal mandibular fracture treated with the RAP osteosynthesis system

FN = female neutered; MN = male neutered
At the second postoperative examination, all cats were found to have a functional, atraumatic occlusion. CT imaging documented radiographic evidence of complete osseous union in all fractures, with the presence of increased bone mineral density and bridging callus across the fracture lines (Figure 6). There were no disruptions to the implants (including implant failure, bending or infection) and no evidence of screw loosening in any of the 13 patients.

(a) Preoperative, (b) immediate postoperative and (c) 8-week postoperative CT images of the medial aspect of the left mandible of case 12
The most common postoperative complication was swelling at the surgical site, which occurred in all cases and resolved with supportive care within 7 days. Immediate postoperative complications included neuropraxia of the mandibular branch of the trigeminal nerve (n = 2), exophthalmos due to retrobulbar haemorrhage (n = 2) and a traumatic occlusion necessitating elective dental extractions (n = 1). One cat exhibited partial wound dehiscence 5 days postoperatively due to self-trauma, which was treated with medical management and healed by second intention. Longer-term complications included intraoral plate exposure 10 months postoperatively in one cat, necessitating the need for plate removal, and temporomandibular joint ankylosis in one cat related to a concurrent traumatic injury.
Discussion
This is the first report on a series of cats that underwent fixation of caudal mandibular fractures using the RAP system. All 13 cats were successfully treated to restore a functional, atraumatic occlusion.
Three-dimensional anatomical plates are commonly used to treat mandibular subcondylar fractures in humans.9,10,17,22 The plates in these systems are pre-printed and designed to match the complex topographical features of the region. In a similar fashion, the RAP system allows an excellent match to the contours of the caudal mandible of cats, enabling the use of ORIF to treat fractures in this location. The precise adaptation to the area was optimised by the development of three plate sizes from studies of healthy feline mandibles, and an appropriately sized plate could be selected from the RAP system for a good fit to achieve fracture stabilisation and accurate anatomical reduction in all 13 cats in this series.
The use of three-dimensional modelling as an aid in the surgical planning of repair of caudal mandibular fractures in cats has been reported previously. 15 This technique reduces intraoperative surgical time and improves the accuracy of contouring. In our case series, a three-dimensional printed model of the mirror image of the intact mandible helped to confirm the selection of the most suitable RAP size before surgery, and to check for fit and contouring. Previous studies have validated this technique by demonstrating a high level of mandibular symmetry in the cat. 19 The range of plate sizes available allowed us to select a plate that closely matched the contours of the caudal mandible in all cases. Therefore, the need for additional plate pre-contouring was minimal, and in the majority of cases was not required at all. This preoperative preparation facilitated accurate anatomical reduction while ensuring that screw placement was located in bone of greatest cortical thickness and strength. Screw performance is strongly correlated with bone quality, and the scarcity of bone stock in the caudal mandible of cats was an important consideration in plate design. There were no cases of screw failure in any of the patients in this case series during the follow-up period evaluated.
Ensuring appropriate plate size selection and anatomical fit before surgery enabled the plate to be used as an intraoperative guide for the reassembly of fragments. In challenging cases with comminution and small, fragile fragments, this method allowed accurate fracture reduction and restoration of an atraumatic occlusion. This exemplifies the use of three-dimensional printing as a surgical planning tool. It should be noted that the RAP manufacturer recommends using the ramus height measured from the preoperative CT scan as a guide for selecting plate size. As the cases in our series required either minimal or no plate pre-contouring, this may justify selection of a plate without three-dimensional modelling. Further studies would be needed to evaluate the correlation of the two methods in choosing plate size, to assess whether similar outcomes are achieved.
Although the previous literature has reported the use of ORIF to repair caudal mandibular fractures in cats,12–16 most studies have tended to focus on either external skeletal fixators or various forms of rigid or semi-rigid MMF. These include modified labial buttons, a bignathic encircling and retaining device, composite bonding of canine teeth or tape muzzle.3–7 These techniques have all been associated with multiple complications, including poor tolerance by the patient, an extended period of assisted feeding, risk of aspiration after vomiting or regurgitation, and postoperative malocclusion, malunion or non-union. In our cases treated with the RAP system, swelling was the most common minor postoperative complication, occurring in all patients, and resolved with supportive care alone. Two cases (cases 8 and 12) had immediate postoperative retrobulbar haemorrhage resulting in exophthalmos ipsilateral to the fracture repair. This was suspected to be a result of iatrogenic trauma from the drill during the intraoperative period. The authors recommend the use of an orthopaedic drill stop device to avoid similar complications in future cases. Both cases of exophthalmos resolved within 48 h with ocular lubrication and anti-inflammatory analgesia, and no longer-term effects were reported within the follow-up period evaluated. This case series shows that ORIF with the RAP system, in comparison with other reported techniques for the treatment of caudal mandibular fractures in cats, has lower patient morbidity postoperatively.
Major complications have been previously defined as those patients requiring surgical revision of the fracture repair technique or a post-fixation malocclusion requiring further treatment. 23 The incidence of major complications has been reported to be as high as 20–57% in previous studies with MMF techniques.4,6 Intraoral plate exposure in case 5, 10 months postoperatively, was the only major surgical postoperative complication observed in this series. Fracture healing and bone consolidation was already complete; therefore, plate removal had no effect on the clinical outcome in this case. A study documenting the outcome of miniplate fixation of mandibular and maxillary fractures in dogs and cats reported an explantation rate of 11%, 12 and is similar to the explantation rate documented in miniplate repair of mandibular fractures in humans.24,25 Further studies with a larger cohort of patients and a longer follow-up time would be required to validate the complication rate compared with previously reported methods of repair.
Time to voluntary food intake postoperatively was in the range of 1–25 days. Two cats (cases 5 and 6) with neuropraxia of the mandibular branch of the trigeminal nerve, likely a result of the initial trauma, had an extended time until eating (25 days and 10 days, respectively) as grasping food was challenging. These nerve injuries were difficult to assess preoperatively due to the multiple craniomaxillofacial injuries present in all cases. Interestingly, the trauma aetiology in both cases was a dog attack, which could suggest that penetrating crushing injuries, in comparison with high-impact vehicular trauma, carry a higher risk of causing concurrent traumatic peripheral nerve injuries. Further research would be required to look for any associations between trauma aetiology and nerve injuries in relation to craniomaxillofacial trauma in cats. Both cases of neuropraxia fully self-resolved within 3–4 weeks with a combination of physiotherapy and appropriate analgesia. Case 9 had a traumatic occlusion visible on immediate postoperative CT imaging. The malocclusion was thought to be a result of a concurrent temporomandibular joint subluxation, as imaging confirmed accurate anatomical reduction of the caudal mandibular fracture achieved with the RAP system. The owner was given the option of semi-rigid MMF or elective extractions and opted for the latter. The same case had facial nerve deficits present as a result of the initial trauma that were likely to have also contributed to an extended time until eating (15 days). Without these three cases that had additional injuries affecting the ability to grasp food, time until eating postoperatively was in the range of 1–7 days, with the majority eating within 2 days.
The RAP system uses a non-locking construct with 1.5 mm cortical screws. Accurate plate contouring is important for reducing the risk of implant failure when using non-locking constructs. If a non-locking plate does not passively fit the contours of the bone, the underlying bone will be pulled towards the plate when applying screws, causing a corresponding shift at the occlusal level and a resultant malocclusion. This would adversely affect jaw function, as well as resulting in implant failure due to exerting abnormal leverage and subsequent loosening. In comparison, in a locking construct, the screws are locked into threaded screw holes in the plate when they are tightened, resulting in a fixed-angle construct. Therefore, screws are less likely to loosen, and screw insertion does not affect fracture reduction. Biomechanical evaluation of locking vs non-locking configurations for internal fixation of mandibular fractures in cats showed that a locking construct was mechanically stronger with superior biomechanical properties compared with a non-locking construct. 14 Another study assessing biomechanical properties of locking vs non-locking L-shaped miniplate fixation of caudal mandibular fractures in cats showed no significant difference in stiffness between the two constructs. 16 Future development of a locking RAP system may have some advantages, such as limited stress shielding effect creating a more stable fixation over time, and less precision required in plate adaptation. Further biomechanical studies would also be useful in determining whether the use of a RAP provides any biomechanical advantage over other reported ORIF techniques for caudal mandibular fractures in cats such as the L-miniplate.
The main limitation of this case series is that it is retrospective and therefore factors such as the lack of standardisation of the procedure and clinical decision-making between cases and between clinicians may have influenced outcomes. There will have been a surgical learning curve regarding technique, being a novel system, which may have also had an impact on outcomes. A longer follow-up time would have been beneficial to avoid underestimating longer-term complications; similar human studies show that most complications occur within the first 12 months.24–26 Despite these limitations, this is the first case series to date that reports the use of the RAP system in clinical cases and can lead the way for more in-depth biomechanical and larger prospective trials in the future.
Conclusions
Rigid internal fixation of caudal mandibular fractures using the RAP osteosynthesis system is associated with a minimal complication rate with excellent radiographic and clinical outcomes in this case series. Precise anatomical adaptation and screw placement allowed accurate fracture reduction in all cases. The reported outcomes are favourable when compared with previous techniques described for management of these fractures. The RAP system offers a novel and successful approach for the repair of caudal mandibular fractures in cats.
Footnotes
Conflict of interest
JS, who developed the RAP system as part of an MSc thesis, is employed by Fusion Implants, which manufactures and sells the system commercially. Linnaeus Veterinary is part of Mars Veterinary Health.
Funding
Linnaeus Veterinary Limited supported the costs of the open access publication charges.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.