
Abstract
Objectives
The aim of the present study was to report the outcome of fractures of the body of the mandible stabilized with wire-reinforced interdental bis-acryl composite splints (WRICS) in cats.
Methods
The medical records of two referral institutions were reviewed. Only cats with mandibular body fractures at or distal to the mandibular canine tooth and treated with WRICS were included. Type of fracture, type and extension of the splint, healing time, dental injuries and treatment complications were retrieved from the medical records.
Results
A total of 13 mandibular fractures were encountered in 12 cats in a 21-year period. The most frequent location of fractures was between the canine tooth and the third premolar tooth. Multiple WRICS configurations were used. The mean ± SD healing time was 49.8 ± 18.9 days. No healing complications were observed in cases with or without dental treatment. Periodontal disease and inflammatory tooth resorption were considered complications secondary to the WRICS.
Conclusions and relevance
WRICS are a suitable technique to repair mandibular fractures in tooth-bearing areas in cats with minimal complications. Additional dental and periodontal care is warranted secondary to the initial trauma or sequela of the WRICS.
Introduction
Cats that sustain maxillofacial trauma often have mandibular fractures (86.7%) among other maxillofacial injuries, with approximately one-third of these fractures affecting the canine, premolar and molar regions. 1 Fracture repair methods for the mandibular body are limited owing to the small size of the patient and the volume of bone available for implant placement, the presence of tooth roots and the location of the mandibular canal. 2 Early stabilization of the bone fracture is advised to obtain a quick return to oral function, optimize bone healing and reduce pain. Non-invasive and minimally invasive maxillomandibular fixation techniques can keep the mouth in occlusion by limiting mouth opening during several weeks of healing.3,4 These techniques do not prevent motion of the caudal bone fragment due to masticatory muscle contraction, have the risk of aspiration and death if the patient vomits, affect thermoregulation and the patient’s ability to eat, and prevent a quick return to function. 5 A lingual arch bar has been described for rostral mandibular fractures distal to the canine teeth, showing good healing outcomes; however, malocclusion and soft tissue injury were frequently reported. 6
Titanium miniplates are an excellent option for the repair of caudal mandibular fractures; however, they may not be the first choice for fractures in the tooth-bearing mandibular body if the screws cannot avoid penetration of the tooth roots.7,8 Intraosseous wires often do not provide sufficient stabilization, and also have the potential to cause dental damage and may be useful only for specific fracture types. Wire-reinforced intraoral composite splints (WRICS) are frequently used for the treatment of mandibular fractures in dogs. 9 WRICS is a non-invasive technique routinely used by veterinary dentists to align tooth-bearing parts of bone fragments in the lower and upper jaws.9,10 Studies have shown that WRICS is an excellent treatment option in dogs.9,11,12 However, studies on the use of WRICS for fractures of the mandibular body in cats are scarce. 13 Previously reported healing times of mandibular fractures in cats vary depending on fracture location, with an average of 10 weeks of healing for mandibular body fractures and 6 weeks for fractures distal to the canine teeth.2,6
The aim of this study was to report the various designs of WRICS and the outcome of mandibular body fractures repaired with WRICS.
Materials and methods
The medical records of cats with fractures of the body of the mandible that presented to two different veterinary hospitals (Veterinary Hospital of the University of Pennsylvania [VHUP] and Facultade de Medicina Veterinaria de Lisboa [FMVL]) between 2004 and 2024 were retrospectively reviewed. Cats were included in this study if a WRICS was used for stabilization of the mandibular fracture and follow-up for removal of the splint was available. Cats with splints used only for treatment of symphyseal separation and parasymphyseal fractures were excluded.
The data collected included signalment of the patient, cause of the mandibular fracture, diagnostic imaging findings, location of the fracture, interdental wire configurations in WRICS (Stout multiple loop, Risdon and modified Risdon with sutures) and extension of the splint. Fractures were classified as simple (one fracture line) or multiple (more than one fracture line), and favorable (fracture line runs from the alveolar margin to the ventral aspect of the mandible in a caudorostral orientation) or unfavorable (fracture line runs from the alveolar margin to the ventral aspect of the mandible in a rostrocaudal orientation). Additional imaging findings to evaluate healing and complications were collected at recheck evaluations and at the time of splint removal. Healing time was considered as the days between WRICS placement and removal. The WRICS was removed if the fracture was stable on palpation and osseous bridging between fragments was noticed on dental radiographs. If these findings were not present, the owner was instructed to come back 3–4 weeks later for further healing evaluation.
Teeth involved in the bone fracture line were grouped based on the classification system described by Schloss and Manfra Marretta (Figure 1). 14

Classification of teeth in the fracture line based on the classification system described by Schloss and Manfra Marretta 14 adapted for the mandibular canine and premolar teeth. (a) Type I: the fracture line runs along the periodontal ligament and reaches the apex. The teeth have the blood supply to the pulp affected and will develop endodontic disease. Luxated teeth were included in this category. (b) Type II: the fracture line runs along the periodontal ligament but does not reach the apex. The blood supply to the tooth is not affected. (c) Type III: the fracture is incomplete. It affects the blood supply to the tooth. Endodontic disease is likely. (d) Type IV: the fracture line runs between teeth without compromising the periodontal health but affects the alveolar bone and may affect the vascularization to the apex if the inferior alveolar vessels are transected. (e) Type V: the fracture line runs along the periodontal ligament, crosses the alveoli from mesial to distal and continues to the ventral margin of the mandible. Endodontic disease is possible. (f) Type VI: the fracture does not affect the periodontal ligament or the dental blood supply. Types I, II and V have periodontal involvement. Types I and III will develop endodontic disease and require endodontic treatment or extraction at the time of splinting or splint removal. Types IV and V may have vascular compromise and develop endodontic disease. Monitoring and dental treatment are warranted as needed
The descriptive analysis was reported as percentages, means ± SD and ranges. An unpaired t-test was used to evaluate the differences in healing time between the two referral institutions, the presence/absence of a visible fracture line at the time of WRICS removal and whether healing time was different between cases with or without additional required treatment of teeth in the bone fracture line. Differences were considered significant if P <0.05. No further statistics were performed because of the low number of cases.
Results
A total of 12 cats with 13 mandibular body fractures at or distal to the canine tooth were treated with WRICS. Seven cases from VHUP (2004–2024) and five cases from FMVL (2015–2024) were included. All patients were domestic shorthair cats. Their mean age and weight were 4.9 years (range 0.3–13.5) and 4.2 kg (range 1.3–7.9), respectively. The main cause of the fracture was a fall from a height (n = 6, 50%), followed by unknown cause (n = 3, 25%). Other causes were animal altercation (n = 1, 8.3%), vehicular accident (n = 1, 8.3%) and jumping from the couch (n = 1, 8.3%).
Fractures were localized at or between canine and third premolar teeth (n = 8, 61.5%), between the third and fourth premolar teeth (n = 2, 15.4%), between the fourth premolar and first molar teeth (n = 2, 15.4%), and between the canine and fourth premolar teeth, extending ventral to the third premolar tooth (n = 1, 7.7%). Most fractures were simple (n = 11, 84.6%) and unfavourable (n = 9, 69.2%). Symphyseal separation was also present in three (25%) cats. All cats had dental radiography performed at the time of injury and at WRICS removal. Six (50%) cats had a CT scan performed at the time of presentation. Additional fractures were identified in the midface (n = 5, 41.6%), ipsilateral or contralateral temporomandibular joint (n = 5, 41.6%) and ramus of the mandible (n = 2, 16.6%). Three (25%) cats did not have other diagnosed fractures apart from in the mandibular body.
WRICS were anchored in canine, premolar and molar teeth. One to three teeth were included in WRICS in the caudal bone fragment (one tooth = 23.1%, two teeth = 23.1%, three teeth = 53.8%) and up to four teeth in the rostral fragment (one tooth = 7.7%, two teeth = 69.2%, three teeth = 15.4%, four teeth = 7.7%). Mandibular incisors were included in the splints in seven (58.3%) cats. In the remaining cases (n = 5, 41.7%), the wire was twisted between the canine teeth lingual to the incisor teeth. WRICS stabilized the symphyseal separation in two cats; the remaining case was stabilized with a circumferential wire, without including the canine teeth in the WRICS.
The main wiring configuration was a Stout multiple loop (n = 8, 61.5%), although this configuration was possible only at the level of the premolar and molar teeth. The other areas were spanned with twisted wire and the wire was looped around the canine teeth. Other configurations were modified Risdon with sutures (n = 4, 30.7%) and Risdon (n = 1, 7.7%). The size of the wire was in the range of 24–28 G, with the 28 G closer to the gingival margin than the other two sizes. The wires were covered with bis-acryl composite (Protemp Plus; 3M) (n = 10, 76.9%) or dental flowable composite (Charisma Flow; Kulzer) (n = 3, 23.1%). All cases had buttons and bridges of dental flowable composite to avoid slippage of the wire coronally during wire placement (Figures 2 and 3).
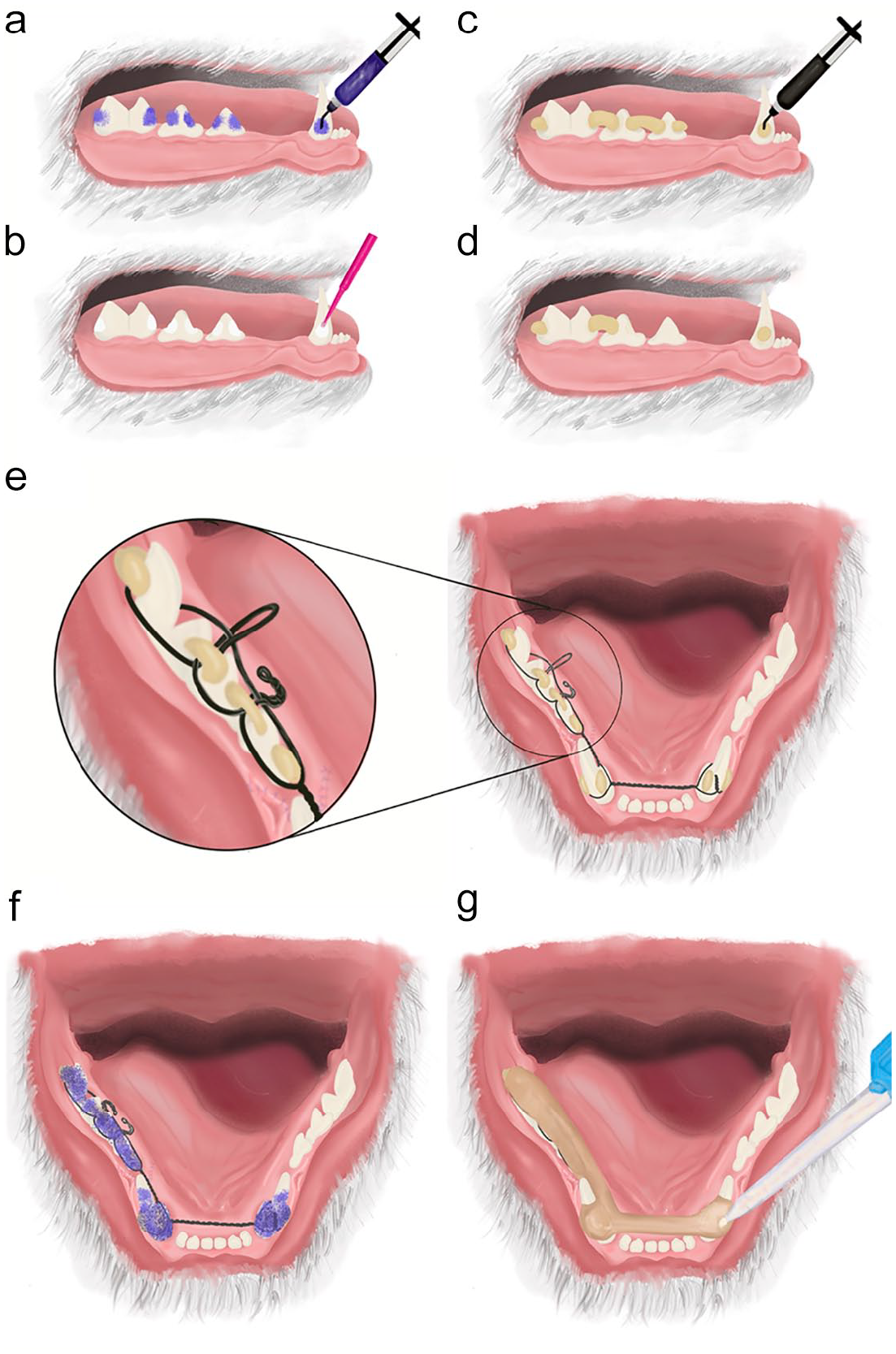
Placement of wire-reinforced interdental bis-acryl composite splints (WRICS) from the left mandibular canine to the right mandibular first molar teeth. Step-by-step process. (a) Acid etching of the tooth surface for 20–30 s with 40% orthophosphoric acid gel to place buttons and bridges made of dental composite. The acid gel is rinsed off and the tooth surface is dried with an air water syringe. (b) Application of a dental adhesive specific for the dental composite (following the manufacturer’s instructions). The authors use a fifth-generation light-cure adhesive. (c) Buttons and bridges for Stout, Risdon or modified Risdon configuration. In the canine teeth, the buttons are placed on both sides of the tooth (labial and lingual). A light-cure flowable dental composite is applied on the same areas where the adhesive was applied before. The buttons and bridges of composite help keep the wire around the teeth during its placement. (d) Buttons and bridges for a modified Risdon wiring configuration with sutures. Only one bridge between the first molar and fourth premolar teeth is needed to loop the wire around the mandibular first molar tooth. (e) Stout multiple loop configuration. The wire is looped under the button on the first molar tooth. The part of the wire located lingual to the teeth (static wire) is kept along the dental arch. The part of the wire located buccal and labial to the teeth (dynamic wire) is passed under the bridges back and forth to create lingual loops. The static wire is passed through the lingual loops. The static and dynamic wires are hand-twisted to span the diastema between the third premolar and canine teeth and between the canine teeth lingual to the incisor teeth. The wires are looped around the canine teeth under the buttons and tightened with wire twisters on the labial aspect of the left canine tooth to avoid interference with the occluding maxillary canine tooth. (f) Repeat etching of the dental surface for 20–30 s, followed by rinsing and drying. (g) Bis-acryl composite (Protemp Plus; 3M) is applied from the first molar tooth area towards the canine teeth, over the dental surface and the wires. It is placed primarily on the lingual aspect to avoid interference with the occluding maxillary teeth. The bis-acryl composite fully sets in about 5 mins. After setting, it can be shaped with an acrylic dental bur or a diamond tapered bur to remove rough areas that could traumatize the soft tissue and to allow complete closure of the mouth. If a flowable dental composite is used instead of the bis-acryl composite, an adhesive should be applied before the dental composite (b,c)

Additional wiring configurations. (a) Original Risdon configuration. One main wire is used on each mandible, looped around a tooth of choice and hand-twisted rostrally on the lingual aspect of the incisor teeth until both wires meet in the midline, where they are tightened together. Both wires could be tightened labial to the incisor teeth instead of lingual. Additional shorter and thinner wires are used to anchor the premolar and canine teeth to the main wires. The twists of the additional wires (*) are bent away from the tongue to create the support for the bis-acryl composite. (b) Wire placement for the modified Risdon configuration with wires or with sutures. The wire is looped around the first molar tooth and then hand-twisted lingual to the cheek teeth until reaching the ipsilateral canine tooth; each end of the wire is looped around the canine tooth and hand-twisted again to span the distance between the right and left canine teeth lingual to the incisor teeth. (c) Modified Risdon configuration. Additional shorter and thinner wires are looped around each individual premolar tooth and secured to the main wire. When they are tightened, the twists are bent away from the tongue (*) to create a base for the bis-acryl composite. (d) Modified Risdon with sutures. A 4-0 or 3-0 synthetic suture is secured in the gingiva and looped around the twisted wire
The mean healing time was 49.77 ± 13.92 days (range 32–71). The mean healing time for VHUP cats was 44.1 ± 14.48 days and for FMVL cats it was 56.3 ± 10.8 days; the difference was not statistically significant (P = 0.11). Bony callus and stability of the fracture were present in all cases at the time of splint removal. However, the bone fracture line was still visible in total or partially on dental radiographs in seven (53.8%) cases. The radiopacity between the fracture fragments was increased at follow-up, indicating bone deposition bridging the fragments (Figures 4 and 5). Only one (7.7%) case was noted to have instability of the fracture site at the initial recheck (45 days); it was re-evaluated 26 days later and the WRICS was removed 71 days after placement. The difference in mean healing time between cases with the fracture line visible (50.1 ± 17.7 days) and not visible (49.3 ± 9.4 days) at the time of WRICS removal was not statistically significant (P = 0.9). The mean healing time of bone fractures that had and did not have dental treatment was 50 ± 15.5 days and 49.6 ± 13.7 days, respectively; the difference was not statistically significant (P = 0.9) (Table 1). Fracture of the splint (with no displacement of bone fragments) was present in two cases at the time of WRICS removal (Figure 4b).
Healing time (time between WRICS placement and removal) of 13 mandibular body factures in 12 cats
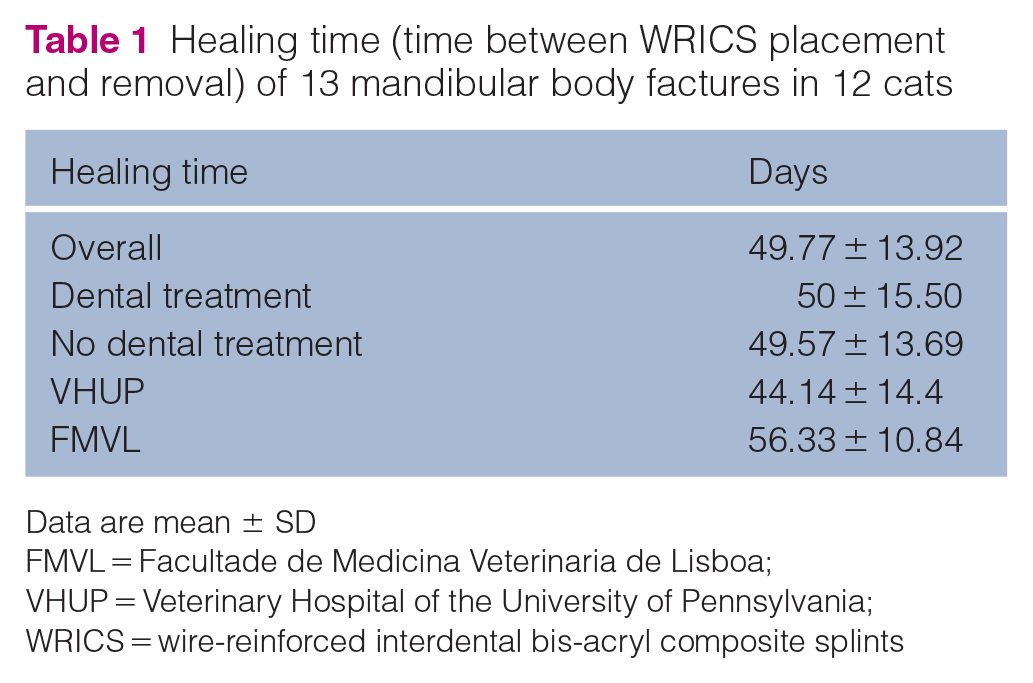
Data are mean ± SD
FMVL = Facultade de Medicina Veterinaria de Lisboa; VHUP = Veterinary Hospital of the University of Pennsylvania; WRICS = wire-reinforced interdental bis-acryl composite splints

Dental radiographs of a 1.6-year-old domestic shorthair cat with a bone fracture located at the left mandibular canine tooth. (a) Intraoperative radiograph at wire placement and before bis-acryl composite application. The fracture line (*) is well defined. (b) Radiograph at WRICS removal 46 days later. The fracture site is remodeling. (c) Occlusal radiograph of the rostral lower jaw. The fracture was stabilized with a Risdon wiring configuration. The excess of twisted wire (orange bar) was ultimately removed and not included in the final WRICS. (d) Radiograph 46 days later. The fracture site appeared healed. A 6-month radiographic follow-up was recommended to evaluate the vitality of the left mandibular canine tooth. WRICS = wire-reinforced interdental bis-acryl composite splints
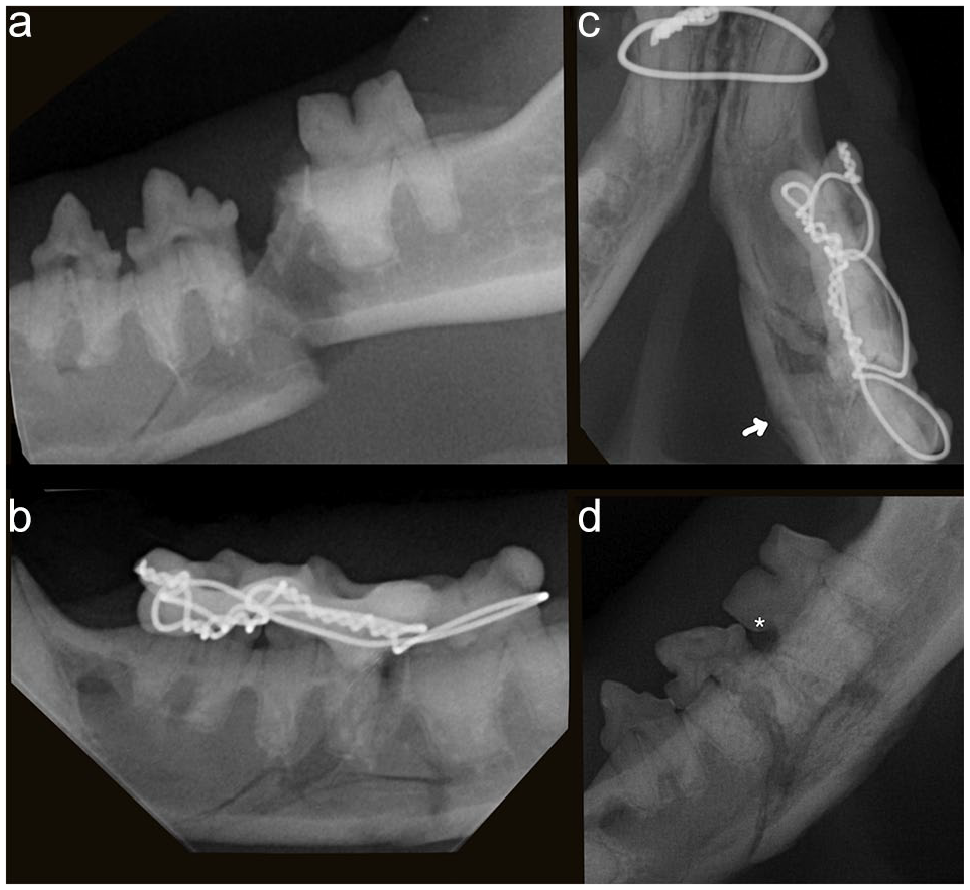
Dental radiographs of a 9-year-old domestic shorthair cat with a mandibular fracture between the left fourth premolar and first molar teeth. (a) The fracture is displaced. Another fracture line extends in a rostroventral direction underneath the third premolar tooth. (b) Stabilization with WRICS using Stout multiple loop wiring. (c) Radiograph 34 days postoperatively. A small bony callus is visible along the ventrolingual aspect of the mandible (arrow) and the line of fracture is less defined than at initial presentation. (d) Radiograph after WRICS removal at 34 days. Only the transverse fracture line between the fourth premolar and first molar teeth is no longer visible. There is periosteal proliferation along the ventral margin of the mandible. A defect at the cementoenamel junction of the first molar tooth (*) is consistent with tooth resorption that may have been minimally present at the time of WRICS placement, which may have progressed during the following month due to inflammation secondary to the fracture or iatrogenic injury secondary to WRICS placement. WRICS = wire-reinforced interdental bis-acryl composite splints
Six (46%) teeth in the bone fracture line had periodontal involvement (type I or II) and seven (56%) teeth did not (type IV or VI). The teeth in the bone fracture line were classified as type I (n = 4, 30.7%), type II (n = 2, 15.4%), type IV (n = 5, 38.5%) or type VI (n = 2, 15.4%). Of these, one canine tooth was extracted because of extrusive luxation and another canine tooth had orthograde root canal treatment performed after WRICS removal. In addition, another canine tooth (not in the bone fracture site, but included in the WRICS) with a complicated crown fracture was extracted. One incisor tooth with severe periodontal disease was extracted next to the fracture site as well as a non-vital first molar tooth secondary to the placement of an intraosseous wire at another facility. The latter had not been extracted at the time of WRICS placement so that it could be used as the only anchor tooth in the distal fragment of the mandibular body fracture. One cat had malocclusion that was treated with selective tooth extraction. The malocclusion was secondary to multiple maxillofacial fractures. Two (16.6%) cases developed inflammatory tooth resorption in areas of contact with wire (Table 2). Periodontal disease was recorded in all cases at the time of WRICS removal, but the description was not sufficient to evaluate the progression of disease secondary to WRICS.
Teeth in or near the bone fracture line that needed dental treatment at the time of WRICS placement or removal

Fracture line spanned the bone between teeth 404, 407 and 408
No evidence of periapical lucency at the time of WRICS removal
Not included in healing time of fractures with teeth that had dental treatment because they were not in or near the fracture line
WRICS = wire-reinforced interdental bis-acryl composite splints
One (8.3%) case had a feeding tube placed for the first 4 weeks because of severe maxillofacial trauma; two (16.7%) other cases showed inappetence in the immediate postoperative period that resolved with pain management (n = 1) and discontinuation of systemic antibiotics (n = 1). Soft food was offered to all cats during the postoperative period. Nine cats were prescribed antibiotic therapy, and a multimodal analgesic protocol was selected for every patient and modified according to the patient’s health status.
Discussion
The results of this study support the application of WRICS for mandibular body fractures mesial to the first molar tooth in cats. Despite the high number of fractures reported in the literature, 1 treatment with WRICS in cats was not a frequent choice of repair based on the rather low number of cases found in the medical records of two referral institutions during a period of 21 years. Other techniques, such maxillomandibular fixation or salvage mandibulectomy, were used in several cases. Furthermore, mandibular fractures are more frequent in the caudal part of the body and ramus of the mandible, for which WRICS is not indicated. 1 The low number of cases also makes the proper management of injured patients challenging, as clinicians may not be exposed to this clinical presentation and thus not be confident enough to employ this technique.
Within the mandibular body, the most frequent fracture location in the present study was between the canine and third premolar teeth, allowing enough teeth rostral and distal to the fracture site to be included in WRICS. Historically, at least two teeth in each fracture fragment should be included in WRICS; 15 however, three cases had only one tooth in the caudal fragment. Although contraction of the masticatory muscles causes displacement of the caudal fragment in a dorsal direction, WRICS in the cases included in the present study were sufficient to align, stabilize and counteract the forces of the masticatory muscles. Other factors, such as reduced masticatory force in the postoperative period and behavioral modification, may have acted in favor of healing.
The preferred wiring technique was the Stout multiple loop in the premolar and molar tooth area, but large diastemas with no teeth (between the third premolar and canine teeth) and gaps between quadrants (between the canine teeth) were spanned by hand-twisting the wire. A study showed that areas with no tooth surfaces incorporated in the WRICS reduce the stability (strength and stiffness) of the Stout multiple loop wiring technique. 12 This may not have enough clinical implication when looking at the population of cats included in the present study, as healing is affected by multiple factors, such as the support provided by the contralateral mandible, type of fracture, vascularization, patient’s biological response and the forces applied to the mandible.
The mean healing time (1.6 months) of mandibular body fractures of the cases in the present study was shorter than that previously reported in dogs and cats (2.3 months).2,9 We compared the healing time at both institutions because follow-up evaluations under anesthesia were performed at different time intervals. The fracture line was still noted radiographically after 2 months of healing in some cases. We did not find a cutoff time for identification of the fracture line, but that may be related to the type of fracture and the presence of a gap between the bone fragments. Regardless, an increased radiopacity indicative of bone deposition was present in all cases. Furthermore, healing occurred despite dental injuries secondary to trauma. Contrary to our results, mandibular fractures in dogs with teeth in the fracture line requiring treatment took longer to heal than fractures where no dental treatment was performed (2.3 vs 1.4 months). 9 Anatomical differences, such as masticatory forces, patient activity, size of the mandible, relative size of the teeth in relation to the mandibular height, volume of the mandible occupied by tooth roots and fracture location, may be contributing factors for these differences.9,16,17 Bone healing occurred by callus formation and further remodeling characteristic of secondary bony healing. 18 The callus formation observed in the dental radiographs of cats in the present study confirms that WRICS allow some degree of interfragmentary motion.
Dental trauma is a common finding in patients with maxillofacial trauma. 19 None of the cats in the present study had obvious bone-healing complications, but dental treatment was needed in some cases directly related to the maxillofacial trauma. The accumulation of plaque and food debris between the oral mucosa and WRICS can cause gingivitis and periodontitis, and inflammatory root resorption could be a possible complication secondary to periodontal disease.20,21 All other complications noted in this study were considered secondary to the maxillofacial trauma, including the malocclusion, which has been associated with severe maxillary, mandibular and temporomandibular joint fractures. 22 Reduction of the fracture fragments during application of WRICS can be a challenge, and mild malalignment of the fragments during splint fabrication bears the risk of causing malocclusion. The follow-up times in the present study were too short to evaluate the cases for the full extent of potential bone-healing complications; however, dental injuries can be a potential source of pain and inflammation and should be treated to maintain good oral health.
The main limitations of the present study are the low number of cases, which prevented the investigation of possible associations between various configurations of WRICS, further bone healing and long-term complications; the lack of multiple standardized radiographic examinations and use of cone-beam CT to determine the progression of healing and possible delayed unions; and insufficient medical records describing the severity of periodontal disease and its progression after WRICS removal. Despite these limitations, the manuscript adds information to the veterinary literature and is useful for veterinary practitioners, who can use this manuscript as a guide for the clinical management of patients with mandibular body fractures.
Conclusions
WRICS is an excellent option for the treatment of mandibular body fractures in cats. The healing of bone fractures at that location occurred in approximately 7 weeks. Complications secondary to WRICS are few, but further studies to evaluate the involvement of WRICS in gingival inflammation and periodontitis are warranted.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.