
Abstract
Practical relevance:
Feline head trauma injuries are common in general practice, often resulting in mandibular fracture. An understanding of the recent advances in the field of mandibular fracture repair will facilitate evidence-based decision-making in clinical practice.
Clinical challenges:
Feline maxillofacial and oral anatomy brings unique challenges in comparison with dogs. It has been commonplace to adapt techniques and equipment that are better suited to other body regions or are species-inappropriate for use in feline maxillofacial surgery, and this has traditionally resulted in high morbidity.
Aims:
This review presents an overview of the diagnosis of, and decison-making for, maxillofacial trauma in cats, specifically with reference to the feline mandible. The challenges associated with the management of these injuries are presented. Techniques for repair that can be employed in general practice, as well as more advanced surgical options, are discussed, as well as the indications for invasive vs non-invasive management. Underutilised methods involving composite dental materials and their versatility for the repair of mandibular fractures in cats, and miniplates for caudal mandibular fractures in cats, are specifically covered, as well as other recent advances in the field, including three-dimensional printing and custom-printed implants.
Evidence base:
Management of feline facial fractures is an often neglected topic, with very few published studies choosing to focus on head trauma outcomes in cats. Where available, however, this review draws on the published literature, as well as the authors’ own clinical experience.
Keywords
Prevalence of mandibular fractures
In a hospital treating both primary care and referral patients, one study described the location and distribution of craniomaxillofacial fractures in 45 cats that had sustained head trauma. 1 It was found that 57.5% of cats presenting with head trauma had a symphyseal separation or parasymphyseal fracture. All of the cats with symphyseal separation or parasymphyseal fracture had additional maxillofacial fractures, and the chance of other mandibular fractures was 85%. Of cats with the latter, 14.3% had a mid-body or caudal mandibular body fracture, 5.9% had a fracture of the ramus and 11.1% had a fracture of the condylar neck. The overall median number of fractured maxillo-facial regions per cat was eight. These results demonstrated that mandibular fractures are common following head trauma, and cats with symphyseal separations will invariably have other injuries that are likely to require management.
Assessment of maxillofacial trauma cases
In the initial assessment of maxillofacial trauma (Figure 1), it is important to look beyond obvious visible injuries for other problems that may go unnoticed such as pneumothorax, diaphragmatic hernia and a ruptured bladder.

Cat with maxillofacial trauma presenting with a midline palatal separation, associated oral mucosal wound and uncomplicated crown fracture of the right maxillary canine tooth
Diagnostic imaging is necessary to visualise fracture sites and identify dentoalveolar injuries; one study showed that 72% of patients presenting with maxillofacial fractures had at least one dentoalveolar injury. 2 Conventional radiography has numerous limitations regarding diagnosis in this region; for example, the overlapping nature of the bones of the skull and the bilateral anatomy reduces the clinical usefulness of plain radiographs because of the superimposition of structures. Dental radiography can be useful, particularly for assessment of mandibular trauma where parallel dental radiography techniques can be employed (for a review of feline dental radiography and radiology see Niemac 3 ). CT has been shown to be superior for diagnosis of maxillofacial fractures (Figure 2) and can identify up to twice the number of maxillofacial injuries in comparison with skull radiographs alone. 4
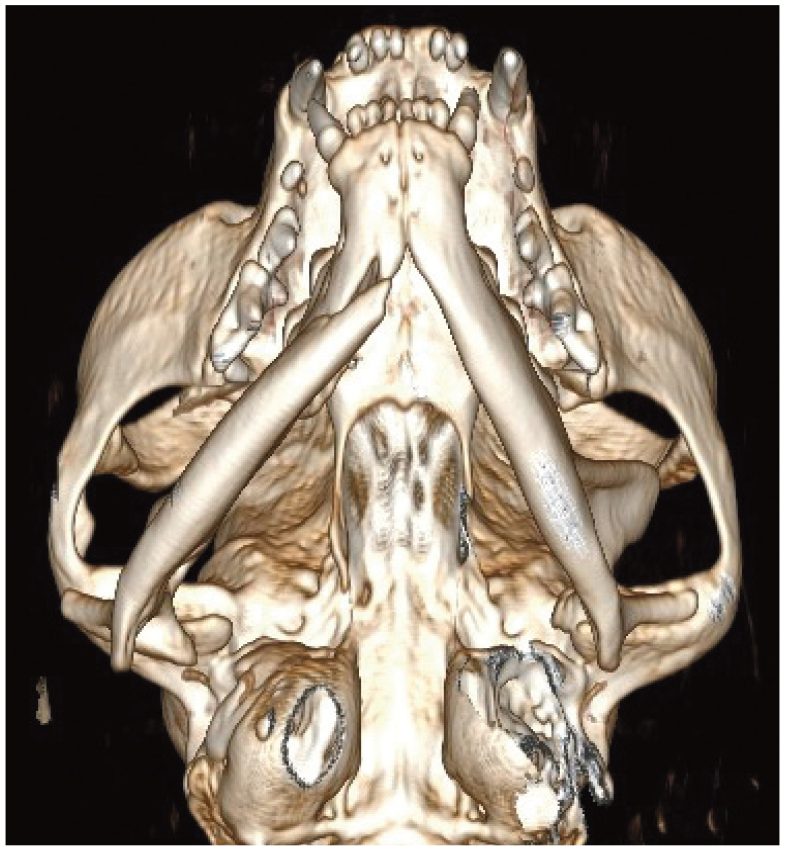
Three-dimensional volume rendering CT image of a feline head trauma patient with a right mid-body mandibular fracture and temporomandibular joint luxation
Nutritional support should be considered (see Taylor et al for guidelines on management of the inappetent hospitalised cat 5 ). It is routine at the authors’ practice to place an oesophageal feeding tube (most commonly while the patient is anaesthetised for CT scanning) at the earliest opportunity in feline patients with maxillofacial trauma that are not voluntarily eating.
Mandibular fracture repair
The basic principles of mandibular fracture repair are well documented6,7 and are described in the box.
Putting principles into practice: why is this a challenge in the feline mandible?
When repairing mandibular fractures in cats, there are several difficulties that can be encountered when applying the principles described in the box.
✜ Muscle insertions and the presence of other structures such as the facial nerve and parotid duct make access to the fracture site challenging during invasive repair techniques.
✜ Occlusion can be difficult to monitor perioperatively if conventional endotracheal intubation is performed (see the ‘Avoiding malocclusion’ box on page 3).
✜ The presence of teeth limits the application of fixation devices at the tension surface.
✜ Tooth roots occupy a large volume of bone in the region in which they are located, and they reduce the volume of bone available in which screws can be placed.
✜ Neurovascular structures in the infraorbital and mandibular canals further limit screw or implant placement.
✜ There is limited quality and thickness of bone, especially at the ramus. At least 1-2 mm of bone is required to place screws for a neutralisation plate. 11
✜ The caudal mandible is highly contoured.
✜ Fractures can be highly comminuted, and it can be difficult to achieve accurate anatomical reduction of small fragments.
While various methods of invasive fracture repair for feline mandibular fractures (summarised later) have been described in the literature, such as the use of miniplates and screws, intramedullary or interfragmentary pins, external skeletal fixators, cerclage wires and interfragmentary wires,12-16 some of these techniques have significant limitations when considering the principles of mandibular fracture repair.
With techniques that require the placement of pins or screws, adequate purchase can be difficult to achieve, as in cats the thickness of bone in the mandible is commonly only around 1-2.5 mm. This can result in premature pin or screw loosening, pull-out, infection and delayed healing, all of which are encountered commonly in the feline mandible.12,17 Further, there is little or no space to insert pins in the mandible rostral to the mandibular first molar teeth in cats because the neurovascular structures in the mandibular canal and roots of the mandibular canine, premolar and molar teeth occupy a large proportion of the volume of the mandible in the dentate regions.


(a) Cat with an uncomplicated crown fracture of the left mandibular canine tooth, a right mandibular lip avulsion and oral mucosal wounds associated with a symphyseal separation. (b) The cat’s oral mucosal wounds were repaired with monocryl 5-0 simple interrupted sutures prior to (c) stabilisation of the symphyseal separation with an intraoral wire and composite splint
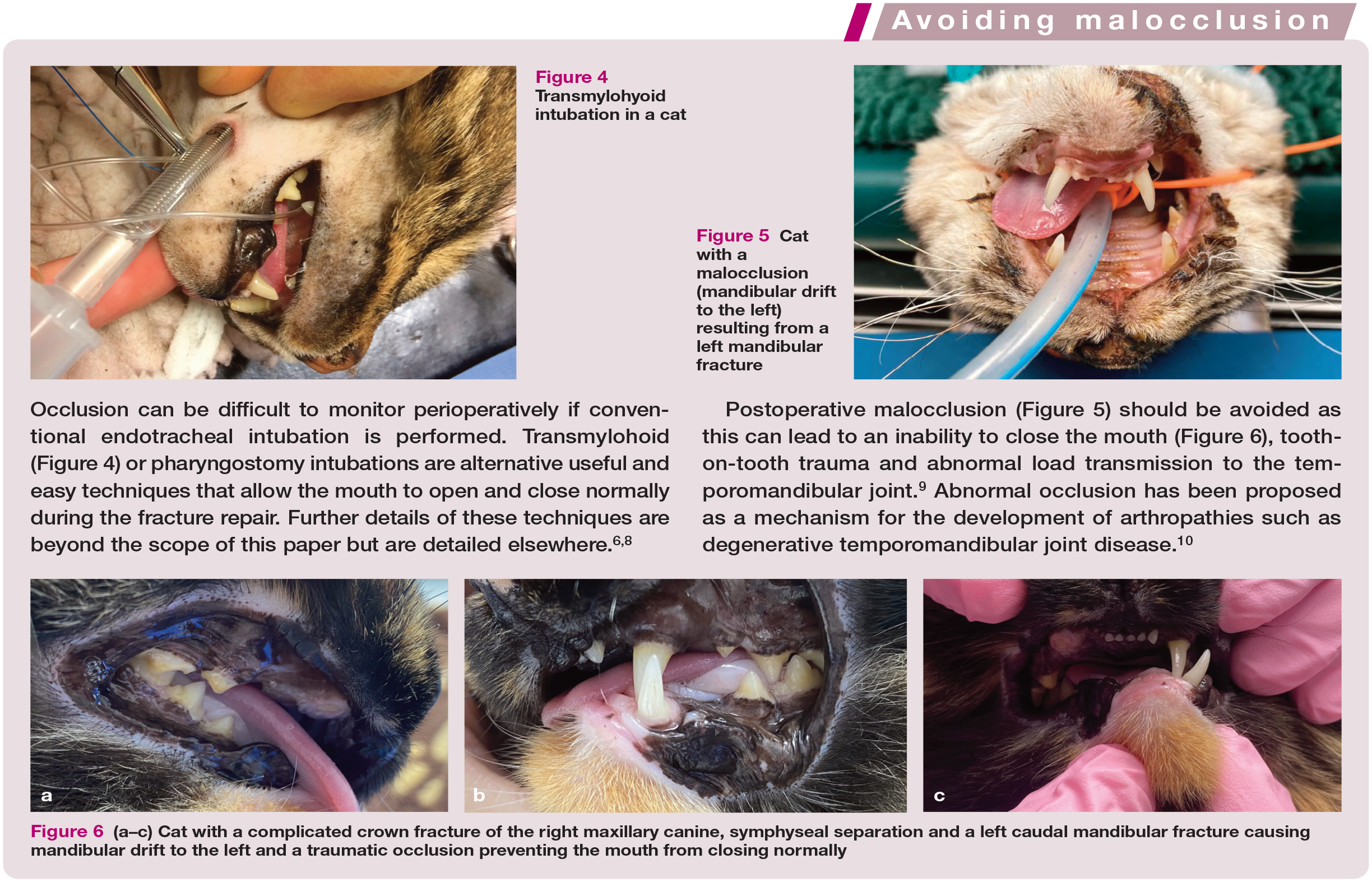

Transmylohyoid intubation in a cat

Cat with a malocclusion (mandibular drift to the left) resulting from a left mandibular fracture

(a-c) Cat with a complicated crown fracture of the right maxillary canine, symphyseal separation and a left caudal mandibular fracture causing mandibular drift to the left and a traumatic occlusion preventing the mouth from closing normally

External skeletal fixators can be large and bulky and have been shown to prevent normal eating, drinking and grooming behaviours while the appliance is in situ. 19 Normal feline behaviour is particularly restricted when the patient has a mandibular bumper bar construct (Figure 7). 14 In a case series where external skeletal fixation was used for jaw fracture repair, 3/7 (42%) cats developed complications that required further surgery (see box on page 7). 17 Many of the pins engaged two mandibles by crossing the intermandibular space, which is likely to lead to compromised tongue function and further damage to soft tissues in that region.7,25-27

(a) Radiograph and (b) photograph of an external skeletal fixator with a bumper bar construct immobilising mandibular fractures in a cat. Images courtesy of Richard Meeson
Interfragmentary wiring tends not to be suited to the thin, fragile bones of the feline mandible and the presence of tooth roots in the rostral mandible and premolar/molar regions is an obstacle to placement of a wire at the alveolar margin - the only location where it can effectively neutralise bending forces according to the tension band principle. 6 When it is possible to apply the first wire, a second, more ventral, wire is usually required to counteract rotational or shear forces. 6 In addition, iatrogenic dental trauma during wire placement is hard to avoid. In a study of rigid internal fixation with interfragmentary wire for mandibular fractures, over 60% of patients developed complications, with the most common being malocclusion (see box on page 7). 23 At the ramus, the bones are subject to shear as well as tension forces and, therefore, neutralisation of these forces with two interfragmentary wires is not possible. 6
As a result of the unacceptably high rate of complications and patient morbidity, the authors consider external skeletal fixators and interfragmentary wires to be unsuitable methods for repair of mandibular fractures in cats.
A modification of an intraoral and circummandibular wiring technique, where a lingual arch bar was secured to the mandibles using circummandibular cerclage wires, was documented in a series of 16 cats. 13 Five out of the sixteen cats developed either malocclusion or non-union (see box on page 7). 13 Despite the reduced incidence of damage to neurovascular structures of the mandibular canal and bony structures or teeth, the resultant soft tissue injuries would be significant and likely to result in loosening of the circummandibular wires and increasing instability of the construct over time. This technique was recommended as being particularly useful in edentulous patients where an intraoral wire and acrylic splint could not be used; 13 in these circumstances, a titanium miniplate (see later) would offer more rigid immobilisation and better fracture reduction with a much lower risk of postoperative malocclusion or non-union.11,19,21
Which fracture repair techniques are most appropriate for the feline mandible?
Much of the previous literature on the subject of mandibular fractures in cats has focused on external skeletal fixation or interfragmentary wires despite the poor outcomes of published case series; in addition, the impact that fracture fixation devices typically have on the welfare of the patients has not typically been considered. While some of these techniques may be more familiar to the surgeon, they should not be performed when high levels of morbidity have been documented. Techniques that have been reported to have greater success rates are described in the following sections.
Titanium miniplates
Rigid internal fixation of maxillofacial fractures with titanium miniplates (Figure 8) is gaining popularity among specialist veterinary dentists/maxillofacial surgeons and is commonly used by the authors for mandibular fracture repair in cats. There are several published case series documenting mandibular fracture repair in cats using miniplates. Miniplate fixation of mandibular repair in cats was originally pioneered by Boudrieau and Kudisch in 1996 11 : a single miniplate was used for fixation of mandibular fractures in three cats and resulted in excellent outcomes with rapid return to function and good to excellent postoperative occlusion. This was followed by a case series of three cats, two of which had mandibular fractures stabilised with four-hole miniplates. 20 Biomechanical cadaver studies have also shown that six-hole miniplates can be successfully applied to the ventrolateral caudal mandible.19,28

Rigid reconstruction and reestablishment of normocclusion immediately improves both the comfort of the patient and jaw function. Miniplate fixation of feline mandibles is challenging, however, due to the difficulties associated with accurate fracture reduction and plate contouring. An open fracture or a fracture with a high degree of comminution does not necessarily preclude the use of a titanium miniplate. The presence of tooth roots limits the use of internal rigid fixation to the caudal mandible in dentate patients.
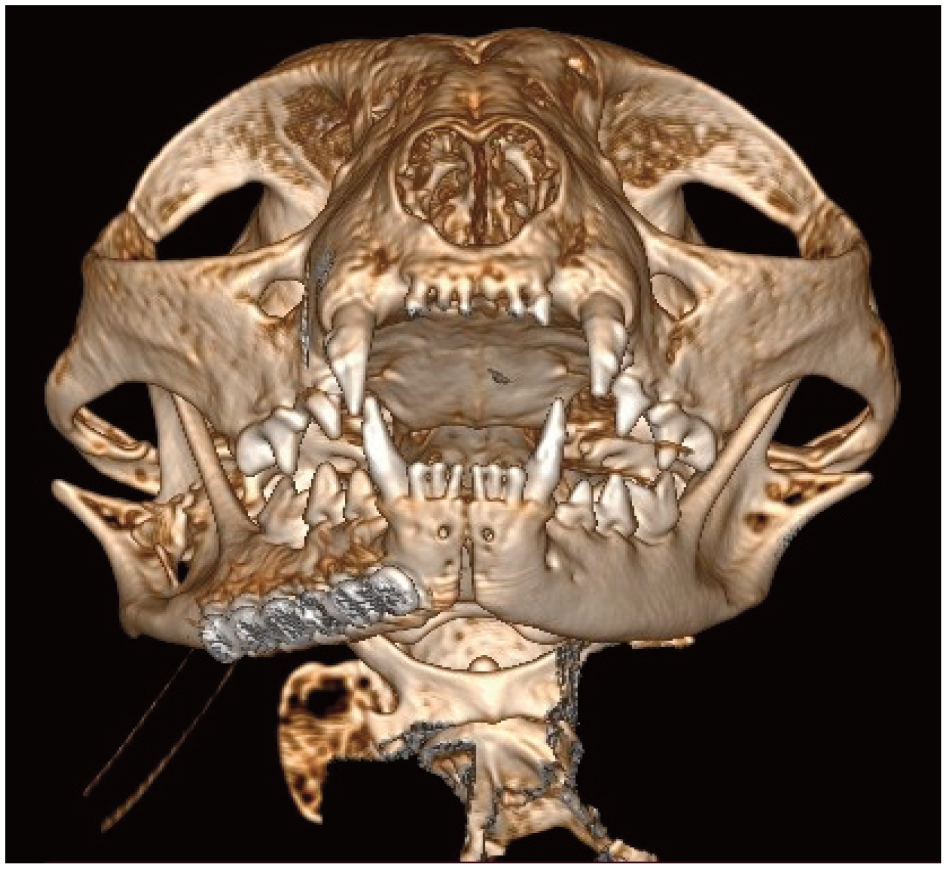
Three-dimensional volume rendering CT image showing a six-hole titanium miniplate for repair of a mid-body mandibular fracture in a cat
Three-dimensional (3D) printing is a useful adjunct and has numerous applications in pre-operative planning in maxillofacial surgery, including planning for fracture repair (Figure 9). 29 One case report described the production of 3D-printed models as templates for pre-contouring implants; the models were based on the mirror image of the intact contralateral mandibles in two cats with complex unilateral caudal mandibular fractures. Plate location was adjusted on the model to ensure the screw holes were optimally positioned to prevent iatrogenic damage. 21 Both cats achieved normal jaw function and occlusion with a rapid return to function and no post-operative complications.

Three-dimensional (3D) printing can be helpful when planning for fracture repair. A 3D printer, such as the Ultimaker shown in (a), can be used to print a PLA study model (b) from a 3D volume rendering CT image, such as that shown in (c), where the cat has a comminuted right caudal mandibular fracture
Rigid internal fixation in the form of miniplates and screws results in excellent anatomical reduction and decreased patient morbidity (see box on page 7) with rapid return to function and is one of the best treatment options for caudal mandibular fractures; however, use is generally limited to those in referral practices who have the necessary skills and equipment.11,19,20,21
Intraoral wire and composite splints
Although the presence of teeth is a hindrance to some methods of fracture repair, it facilitates the use of intraoral techniques that incorporate the crowns of the teeth into fixation devices. These fall into the category of non-invasive management techniques and they take advantage of the biological basis of wound healing using closed reduction. These can broadly be divided further into techniques that aim to semi-rigidly stabilise the fractures and techniques that do not rigidly stabilise the fractures but rely on the inter-digitation of the teeth to maintain occlusion while indirect fracture healing occurs. Of the aforementioned techniques providing semirigid stabilisation, wire and composite splints provide the highest levels of rigidity and accurate anatomical reduction (Figure 10). In the authors’ opinion, this is the treatment of choice for mandibular fractures rostral to the mandibular fourth premolar due to the relatively accurate anatomical reduction that can be achieved while minimising the risk of iatrogenic damage to other structures in the oral cavity. Use of a wire and composite splint is not restricted to simple transverse mandibular fractures, although if used for immobilisation of comminuted mandibular fractures, accurate reduction of fracture fragments and application of the splint is more challenging.

Wire and composite splints for repair of a (a,b) mid-body right mandibular fracture, (c) midline palatal separation and maxillary fracture and (d) left rostral maxillary fracture. Note in (a) the modified stout loop wire that has been applied to create the framework for the intraoral splint
Although application of an intraoral wire and composite splint requires specific equipment and training, the equipment and materials are relatively inexpensive and easy to acquire, and the basics of the techniques are easy to learn and can be applied by skilled general practitioners - see Smith and Legendre for further detail. 30 The most common wire configurations are the crossover technique and the modified stout loop technique (Figure 10a), both of which have been shown to be biomechanically similar. 31 Lingual and buccal wires weave around the crowns of the teeth in the oral cavity; the wire is then reinforced with composite (Figures 10b-d), with the resulting construct stronger than either wire or composite alone. 32

Intraoral wire and composite splint for stabilisation of a mandibular symphyseal separation as an alternative to a circummandibular wire
An intraoral wire and composite splint is an excellent alternative to circummandibular cerclage wires, and is often used for stabilisation of symphyseal separation (Figure 11 and see box) or parasymphyseal fractures. Circummandibular wires have many disadvantages including traumatic injury to the soft tissues, pain and subsequent loosening of the wire once soft tissue swelling has subsided. When used for repair of mandibular symphyseal separations, tightening of circummandibular wire tends to cause the dorsal mandibles to rotate medially, resulting in the crowns of the mandibular canine teeth becoming more upright. This leads to malocclusion with the incisors or mucosal tissues of the incisive region, which can prevent normal closing of the mouth and cause abnormal loading of the temporomandibular joints. The malocclusion can be compounded if the patient has concurrent maxillary fractures.

Only a single case report has been published where an intraoral wire and composite splint was the sole method of fracture repair in a cat, despite this being a technique that is used commonly by veterinary dentists. 33 However, a study investigating the healing of a series of small breed dogs with mandibular fractures undergoing primary repair with intraoral wire and acrylic splints reported a major complication rate (significant postoperative malocclusion or requirement for surgical revision) of 15.4% (2 /13 dogs). This compares favourably with published complication rates of other fracture repair methods while maintaining normal jaw function without sacrificing optimal oral and dental health. 34
Conservative management (salvage) techniques for when splints or titanium miniplates cannot be used
Other conservative management techniques, such as composite maxillomandibular fixation (MMF), 22 bignathic encircling and retaining devices (BEARDs), 24 modified labial buttons 35 or muzzle coaptation (Figure 12) 36 rely on the immobilisation of the mandibles relative to the maxilla (or vice versa) in order to restore normal occlusion and reduce movement of bone ends at the fracture site as much as possible. When referral for more advanced surgical fixation is not possible, these techniques can be relatively easily utilised by general practitioners to achieve an acceptable outcome, but it is important to note that rigid fixation of the fracture site is unlikely to be achieved and the rate of longer term complications will therefore be higher.11,20,37
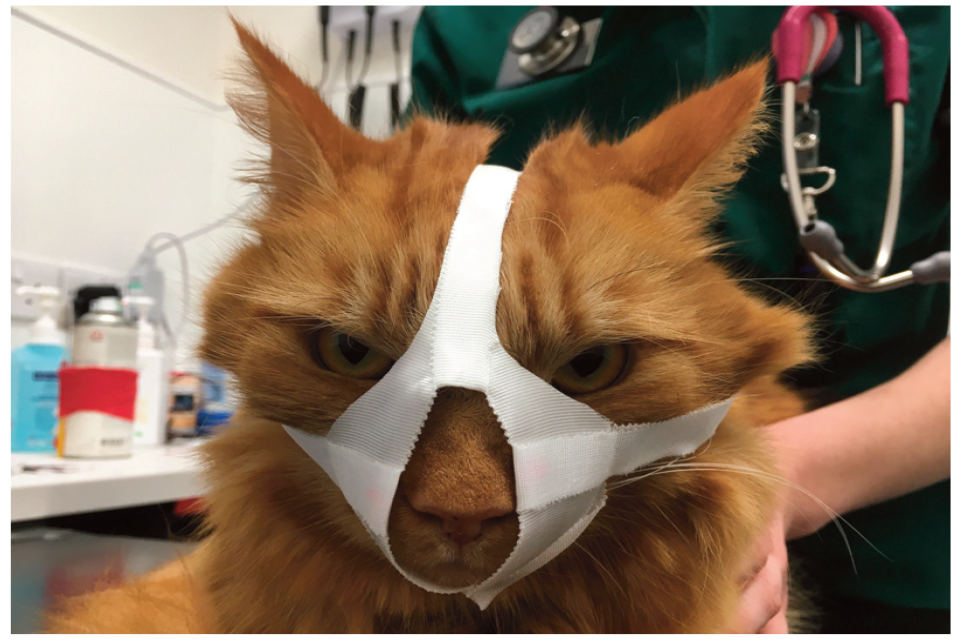
Muzzle coaptation for stabilisation of a mandibular fracture
In addition to the major complications described in the box, other complications that can arise following the use of conservative techniques such as MMF, BEARD, modified labial buttons and tape muzzle include:
✜ Delayed return to normal eating
✜ Higher risk of post-fixation malocclusion, malunion or non-union
✜ Long duration of hospitalisation
✜ Increased risk of aspiration
✜ Tooth injury during removal of composites
✜ Dermatitis from tape muzzle/BEARD
Where treatment with intraoral wire and composite splint or miniplate fixation is not possible, composite MMF (see box on page 8) should be considered as the next best alternative, and in preference to MMF with external skeletal fixation. The authors consider MMF, BEARD, modified labial buttons or muzzle coaptation to then be salvage procedures, performed where more accurate anatomical reduction is unachievable.
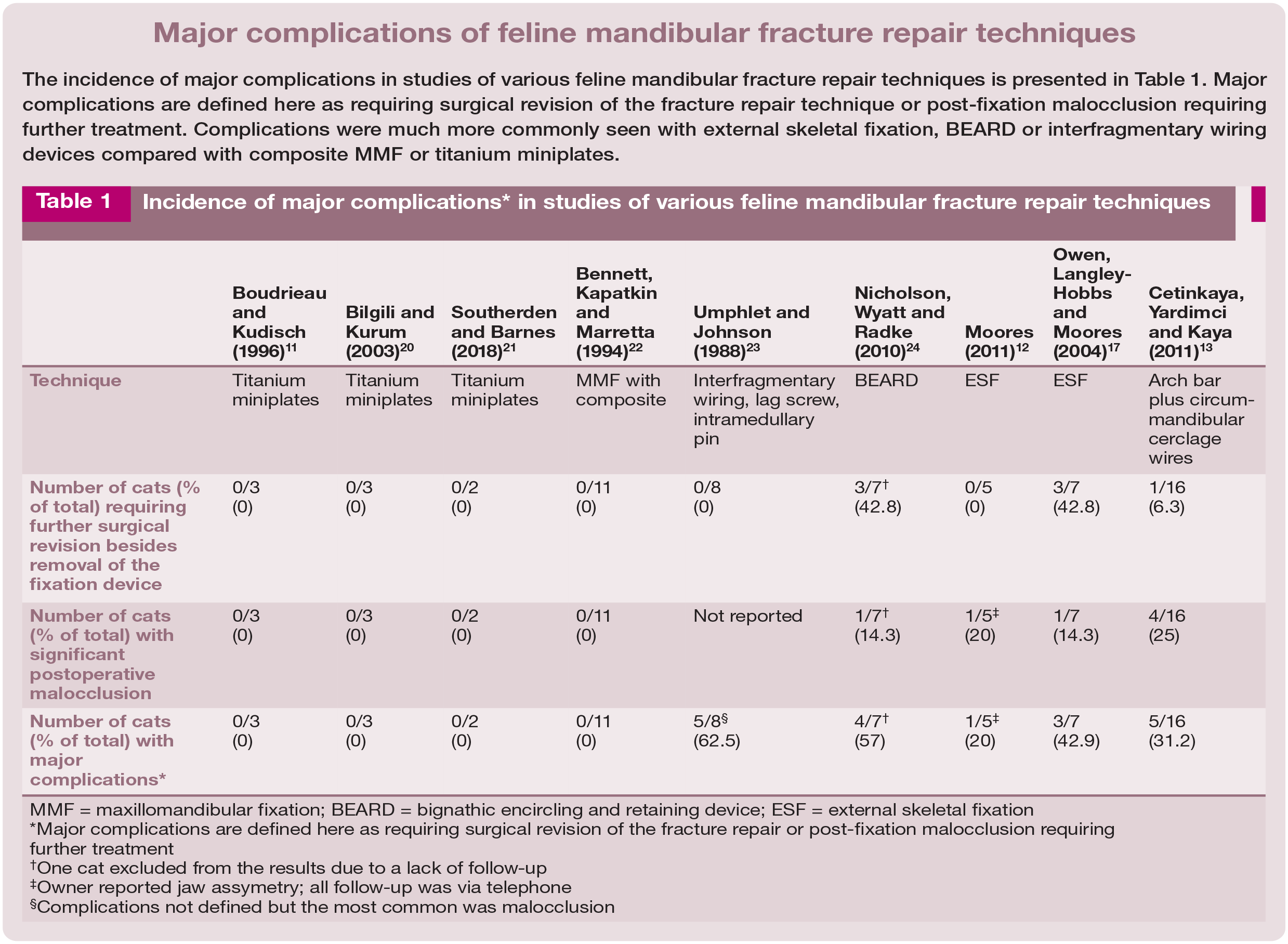
Incidence of major complications* in studies of various feline mandibular fracture repair techniques

MMF = maxillomandibular fixation; BEARD = bignathic encircling and retaining device; ESF = external skeletal fixation
Major complications are defined here as requiring surgical revision of the fracture repair or post-fixation malocclusion requiring further treatment
One cat excluded from the results due to a lack of follow-up
Owner reported jaw assymetry; all follow-up was via telephone
Complications not defined but the most common was malocclusion


(a) Conventional composite maxillomandibular fixation (MMF) and (b) MMF applied between the left canine teeth only. In both, the MMF has been combined with an intraoral wire and composite splint between the mandibular canine teeth to repair a symphyseal separation
What does the future hold?
Feline maxillofacial fracture repair is a rapidly evolving field. As in other veterinary orthopaedic fields, the use of additive manufacturing is giving rise to a variety of new implants that are contoured to specific anatomical regions. Recent advances include the manufacture of feline-specific pre-printed titanium implants in a variety of sizes that are contoured to the feline caudal mandible for repair of fractures of the ramus and caudal mandibular body (Figure 14), 38 and a conceptual model of a mandibular prosthesis for use in repairing mandibular body frac-tures. 39
It is likely that techniques at the forefront of human maxillofacial fracture repair will continue to gradually filter down into veterinary max-illofacial surgery. It may not be long before we are using 3D planning for all complex head trauma cases and producing the high-performance titanium alloy or resorbable composite patient-specific osteosynthesis plates that are becoming the standard of care in human surgery.40-42
Whichever method is chosen for treating traumatic facial injuries, it should be remembered that, alongside the fracture repair principles, the veterinarian should first seek to do no harm when selecting an appropriate method for fracture fixation.

Pre-treatment planning and application of feline-specific pre-printed titanium implants. (a) Titanium ramus anatomical plate selected using three-dimensional PLA model during pre-surgical planning. (b) Lateral view of the left mandible and (c) ventrodorsal view of the mandibles showing a titanium ramus anatomical plate stabilising a left caudal mandibular fracture combined with an intraoral wire and composite splint
KEY Points
✜ Fractured teeth should not be ignored as such damage is likely to cause patients long-term pain and discomfort. Endodontic treatment or extraction should be undertaken as soon as possible, ideally during the initial surgery along with management of other maxillofacial injuries.
✜ Techniques with documented high levels of morbidity should not be used, even if they may be more familiar to the surgeon.
✜ Due consideration should be given to feline anatomy, and dental trauma and damage to neurovascular structures during pin placement should be avoided. Teeth should only be used to anchor screws if no other options are available, and in such circumstances endodontic treatment of the tooth should be performed first.
✜ The biomechanics and ideal placement of locking titanium miniplates in the feline mandible have been established and tested in the veterinary literature and can be considered for any mid-body or caudal mandibular fractures.
✜ Non-invasive fracture repair techniques such as intraoral wire and composite splints are particularly good options for rostral mandibular fractures or symphyseal separations.
✜ The incidence of complications following fracture repair using composites or miniplate fixation is among the lowest of all the techniques discussed.
✜ In patients with fractures not amenable to treatment with composite and wire splints or miniplate fixation, composite MMF should be considered as the next best alternative for its high success rates and maintenance of occlusion with minimal collateral trauma to dentoalveolar structures during application.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.