
Abstract
Objectives
The aim of the study was to describe clinical examination and thoracic CT (TCT) findings in cats after trauma, and to identify physical examination findings associated with both abnormalities on TCT and the need for therapeutic interventions.
Methods
A multicentre, retrospective, observational study was conducted. Cats admitted to the participating hospitals with a history of blunt trauma and that underwent TCT were eligible. Data were collected on signalment, history, physical examination, TCT findings and subsequent interventions.
Results
In total, 137 cats were included. Road traffic accidents (RTAs) were the most frequently reported cause of trauma (69%). Tachypnoea (32%), pale mucous membranes (22%) and dyspnoea (20%) were the most common abnormal findings on thoracic examination. The most frequently identified thoracic pathologies on TCT were atelectasis (34%), pulmonary contusions (33%), pneumothorax (29%) and pleural effusion (20%). Thoracocentesis was the most commonly performed intervention (12%), followed by chest drain placement (7%). A total of 45 (33%) cats had no physical examination abnormalities but did have abnormalities detected on TCT; six of these cats required interventions. Increasing numbers of thoracic abnormalities on clinical examination were associated with increasing likelihood of having abnormal findings on TCT (odds ratio [OR] 2.04, 95% confidence interval [CI] 1.21–3.44, P = 0.008) and of requiring an intervention (OR 1.82, 95% CI 1.32–2.51, P <0.001).
Conclusions and relevance
RTAs were the most common reported cause of blunt trauma. Atelectasis, pulmonary contusions and pneumothorax were the most common abnormalities identified on TCT, and thoracic drainage was the most utilised intervention. TCT may be useful in identifying cats with normal thoracic physical examination findings that have significant thoracic pathology, and a high number of abnormal findings on thoracic examination should raise suspicion for both minor and major thoracic pathology. The results of this study can be used to assist in selecting appropriate cases for TCT after blunt trauma.
Introduction
Survey CT has gained popularity in the early assessment of human trauma patients, due to its speed and sensitivity in identifying injuries.1–11 However, this practice remains controversial, with some studies suggesting that it has no effect on treatment or mortality rates,12 –15 while increasing the risks associated with radiation exposure and limited access to critically injured patients. The use of CT as a screening tool in veterinary patients is further confounded by the need for chemical restraint in potentially unstable patients, as well as the cost implications. 16 Nonetheless, previous studies have advocated consideration of its use as a first-line diagnostic test in trauma patients.16,17
Traumatic injury is one of the most common reasons for feline patients presenting in the emergency setting,18–20 with road traffic accidents (RTAs), bite wounds and so-called ‘high-rise syndrome’ among the most frequent causes. Thoracic injuries are reportedly the most common injuries in veterinary polytrauma patients;19,21 –24 injuries can be life-threatening, and early identification and intervention is essential in attaining positive outcomes.
Thoracic CT (TCT) has been shown to have a greater sensitivity in detecting pathology than more traditional imaging techniques, such as radiographs and thoracic focused assessment with sonography for trauma (TFAST). 25 However, the clinical relevance of this additional information in trauma patients has been questioned, with research suggesting that despite CT enabling the diagnosis of more minor pathologies, this has no effect on either treatment plans or survival.16,26
Physical examination has long been the cornerstone of assessing and triaging veterinary patients. 27 Thoracic auscultation is predictive of thoracic findings on radiographs, 19 but the correlation between physical examination findings and CT abnormalities in trauma patients has not yet been evaluated in the veterinary literature and may indicate whether CT should be utilised as a first-line diagnostic test in these patients. The objectives of the present study were to describe clinical examination and TCT findings in cats after blunt trauma, and to identify physical examination findings associated with both abnormalities on TCT and the need for therapeutic interventions.
Materials and methods
This was a multicentre, retrospective, observational study, involving three private referral hospitals in the UK. Cats admitted to any of the participating hospitals between January 2012 and December 2022, with a history of either witnessed or suspected blunt force trauma, and that subsequently underwent TCT were eligible for the study.
Records were reviewed and data were collected on signalment, including breed, age, sex and neutering status, as well as the nature of the trauma. The nature of the trauma was recorded in specific categories if it was either witnessed or highly suspected based on history and examination. Physical examination findings were collated based on clinical examination at the time of presentation at the participating hospital. Parameters that were not specifically commented on within the clinical notes were presumed to be within normal limits. CT scans were performed under chemical restraint; the decision to either sedate or anaesthetise patients was made on a case-by-case basis by the attending clinician or anaesthetist. For participants undergoing CT of other anatomical regions in addition to the thorax, anatomical study locations were documented. Abnormalities detected on TCT and any therapeutic interventions implemented after TCT were recorded.
Ethical approval was sought from the University of Nottingham’s ethical review panel.
Statistical analysis
All variables were summarised using descriptive statistics. Fisher’s exact tests were used to explore the associations between physical examination findings and TCT abnormalities, between physical examination findings and subsequent intervention, and between specific abnormal TCT findings and having abnormalities identified on thoracic physical examination. Stepwise binary logistic regression models were used to identify predictors of TCT findings based on physical examination, as well as the requirement for intervention based on TCT findings. A binary logistic regression was also used to relate the presence of abnormal CT findings and of interventions to the number of abnormalities on physical examination. Statistical significance was set at P <0.05. Clinical and TCT findings identified in fewer than 10 cases were excluded from analysis.
Results
A total of 139 cats met the inclusion criteria. Of these, two cats were later excluded as no physical examination findings were recorded due to the temperament of the animals on presentation, leaving 137 cats in the analysis. Breeds comprised domestic shorthair (n = 109), domestic longhair (n = 6), British Shorthair (n = 5), Bengal (n = 4), Ragdoll (n = 3), British Blue (n = 2), crossbreed (n = 2) and one each of Siamese, Maine Coon, Russian Blue, Tonkinese, Norwegian Forest Cat and one was unknown. There were 83 male cats (79 neutered, four entire) and 50 female cats (48 neutered, two entire). Four cats did not have their sex recorded. The median age was 41 months (range 1–216).
RTAs were the most common cause of trauma, with 94 (69%) cats presenting for this reason; 37 (27%) had an unknown history and six (4%) had experienced a fall.
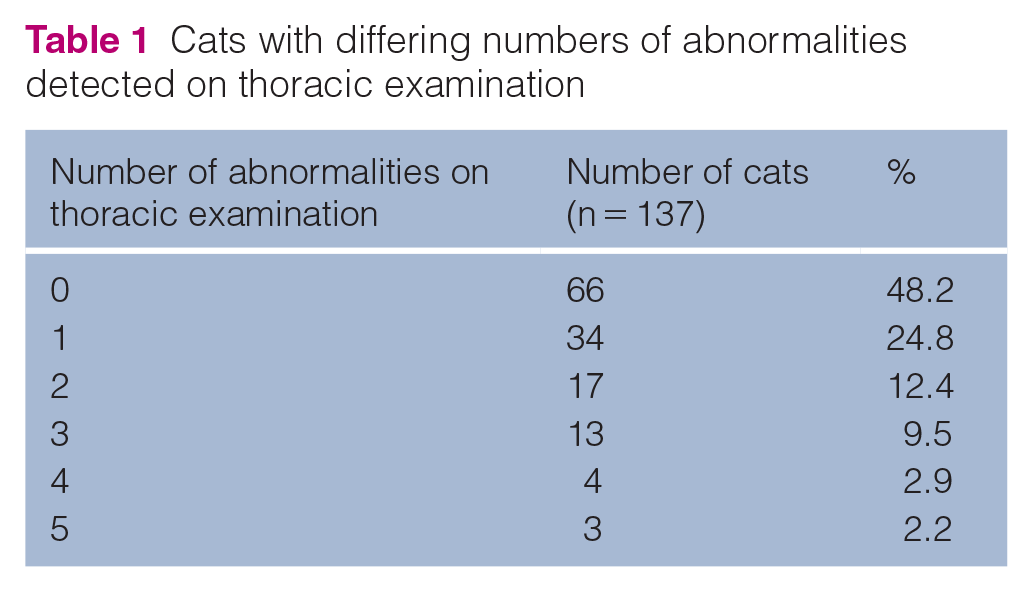
The most common abnormal findings on clinical examination were as follows: tachypnoea (n = 44, 32%); pale mucous membranes (n = 30, 22%); dyspnoea (n = 28, 20%); tachycardia (n = 23, 17%); altered mentation (n = 19, 14%); reduced lung sounds (n = 15, 11%); pain on abdominal palpation (n = 9, 7%); harsh lung sounds (n = 7, 5%); external thoracic wounds (n = 7, 5%); external abdominal wounds (n = 6, 4%); and weak pulses (n = 5, 4%). Cats were further categorised by the number of abnormalities detected on thoracic examination (Table 1).
Cats with differing numbers of abnormalities detected on thoracic examination
Other anatomical regions examined on CT at the same time as the thoracic study included the pelvis (n = 75), head (n = 66), abdomen (n = 61), regions of the appendicular skeleton (n = 36) and neck (n = 24).
In total, 31 (23%) cats had a completely normal TCT, while 106 (77%) had abnormalities detected. The most common abnormalities identified on TCT are summarised in Table 2.
Number of cats with abnormal findings on TCT (cats could have more than one abnormality, so percentages do not add up to 100%)

TCT = thoracic CT
A total of 21 (15%) cats had no abnormalities identified on either thoracic physical examination or TCT; 63 (46%) had abnormalities on both examination and TCT; 45 (33%) had no physical examination abnormalities but did have abnormalities detected on TCT – six of these required an intervention. Eight cats (6%) had abnormalities detected on clinical examination, but a normal TCT.
Fisher’s exact tests were used to identify physical examination findings associated with abnormal findings on TCT and found tachypnoea to be the only significant finding (P = 0.004).
Several TCT abnormalities were significantly associated with the presence of one or more abnormalities on thoracic examination, including pneumothorax (P <0.001), subcutaneous emphysema (P <0.001), pneumomediastinum (P = 0.006), pulmonary contusions (P = 0.006) and rib fractures (P = 0.049). Pulmonary collapse, atelectasis and pleural effusion were not significantly associated with an abnormal physical examination.
An increasing number of thoracic abnormalities on examination was a significant predictor of the presence of abnormal findings on TCT (odds ratio [OR] 2.04, 95% confidence interval [CI] 1.21–3.44, P = 0.008). The results of stepwise binary logistic regressions of individual TCT findings on individual physical examination findings are displayed in Table 3.
Stepwise binary logistic regression of abnormal TCT findings on physical examination findings

CI = confidence interval; OR = odds ratio; TCT = thoracic CT
In total, 28 (20%) cats in the study required an intervention after TCT. A total of 17 (12%) cats required thoracocentesis based on the TCT findings: 10 (7%) had a chest drain placed and seven (5%) required surgery – two for diaphragmatic hernia repair, three for repair of a tracheal injury and two for repair of fractured thoracic vertebrae. One cat had a bronchoalveolar lavage due to an incidental finding of suspected chronic bronchitis. In total, 109 (80%) cats did not require any kind of intervention after TCT.
The presence of dyspnoea on physical examination was significantly associated with ultimately requiring an intervention (P <0.001), as was the presence of tachypnoea (P = 0.003) and reduced lung sounds (P = 0.003). When modelled using binary logistic regression, reduced lung sounds was the only significant predictor (OR 6.29, 95% CI 2.03–19.50, P = 0.001).
A highly significant association was found between an increasing number of abnormal physical examination findings and the ultimate need for intervention (OR 1.82, 95% CI 1.32–2.51, P <0.001).
Discussion
This study describes the findings of physical examination and TCT after blunt trauma in a large population of cats. Witnessed or suspected RTAs were the most common cause of trauma seen in this study, which is in line with figures reported in previous literature. 19
Approximately half (48%) of the cats in this study did not have any abnormalities detected on thoracic examination, while 77% of cats had abnormalities detected on TCT, suggesting that physical examination may lack sensitivity for identifying thoracic injuries. Six cats with a normal thoracic examination went on to require a therapeutic intervention, demonstrating that even significant pathologies could be missed if cats were selected for TCT based on clinical findings alone. Unfortunately, due to the retrospective nature of the study, it is impossible to know the reasoning behind the interventions being implemented, and it is therefore feasible that these were due to a clinical deterioration as opposed to the imaging findings.
Despite the high prevalence of abnormalities identified on TCT, only 28 (20%) cats in this study ultimately required a therapeutic intervention on the basis of these findings, of which thoracic drainage (either by thoracocentesis or chest drain placement) was by far the most common.
This study identified pulmonary contusions and pneumothorax to be the most commonly diagnosed thoracic injuries on TCT, which supports the findings of previous studies in dogs after blunt trauma21,22 and radiographic findings in cats. 28 While atelectasis was the most commonly identified abnormality, as has been described in the previous literature, 29 it is challenging to interpret the clinical relevance in this context. While in some cases this may have been a result of the preceding trauma, atelectasis can also be seen as a result of general anaesthesia and sedation. 30
TCT findings of pneumothorax, subcutaneous emphysema, pneumomediastinum, pulmonary contusions and rib fractures were all significantly associated with abnormalities on examination. Conversely, pulmonary collapse, atelectasis and pleural effusion were not. While atelectasis and pulmonary collapse may be attributed to sedation or general anaesthesia, pleural effusion is more likely to have occurred before examination; therefore, this suggests that physical examination may not be a good predictor of the presence of pleural effusion. The binary logistic regression of TCT findings on physical examination findings identified an association between dyspnoea and both contusions and subcutaneous emphysema. In addition, there was an association between both tachypnoea and reduced lung sounds and the presence of a pneumothorax. This may be useful when examining trauma patients and may raise the clinician’s suspicion of these specific pathologies if these physical examination findings are identified.
Dyspnoea, tachypnoea and reduced lung sounds were all significantly associated with cats ultimately requiring a therapeutic intervention. There was also a strong association between increasing numbers of thoracic abnormalities on examination and the presence of abnormalities on TCT, as well as the requirement for a therapeutic intervention. This may be useful in guiding decision making in trauma patients, and concerns for thoracic pathology should be raised with increasing numbers of abnormalities detected on examination.
TCT is useful as a screening tool and may identify thoracic injuries that were not suspected on clinical examination alone. However, other imaging modalities, such as radiography and ultrasonography, can also be successfully utilised in detecting these injuries,19,23,31 and may require less risk to the patient at a reduced cost. Clinicians should consider history, examination and the availability and results of other diagnostic imaging modalities in order to appropriately select patients for TCT to maximise outcomes while minimising unnecessary procedures and risk to patients.
The main limitations of this study are due to its retrospective nature. This led to a reliance on complete contemporaneous clinical notes. In addition, there is a degree of subjectivity to physical examination findings between individual clinicians. Furthermore, there was no standardisation in interventions before the original recorded examination, and therefore the original stabilisation and analgesia by the referring clinician may have impacted physical examination findings. The data in this study may also be subject to a case selection bias, given that the inclusion criteria required all cats to have had a TCT.
This study did not address long-term outcomes, and future studies comparing outcomes of trauma patients in which TCT was used as a primary diagnostic test with those that had thoracic radiographs and ultrasound may be useful in understanding the true clinical value of TCT in assessing trauma patients. Furthermore, while this study focused on imaging of the thorax, studies into the value of whole-body CT may be useful in the veterinary emergency setting.
Conclusions
RTAs were the most common cause of blunt trauma to cats in this study. Atelectasis, pulmonary contusions and pneumothorax were the most common abnormalities identified on TCT, and thoracic drainage was the most frequent therapeutic intervention required for these animals. A high number of abnormal findings on thoracic examination should raise clinician suspicion for both minor and major thoracic pathology. The results of this study may be useful in selecting appropriate cases for TCT after blunt trauma, and highlights that even patients without abnormal physical examination findings may benefit from early assessment with TCT.
Footnotes
Acknowledgements
The authors would like to thank Tim Sparks (Waltham Petcare Science Institute) for his statistical support.
Conflict of interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Linnaeus Veterinary Limited supported the costs of the Open Access publication charges.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.