
Abstract
Objective
Laparoscopic cholecystectomy (LC) has become a popular method in the treatment of gallbladder calculi incarceration (GCI). This study aimed to investigate the effect of early and delayed LC on patients with GCI to determine the optimal timing for LC.
Methods
The clinical data of 639 patients with GCI who had received LC were analyzed retrospectively. According to the duration of symptoms before admission and that from admission to LC, the patients were divided into different groups. The relationship between conversion and postoperative complications was compared among the different groups.
Results
Seventy-two patients (11.27%) underwent conversion to laparotomy, and 65 patients (10.17%) had postoperative complications. Patients in the LC > 15 d group were older (p < 0.001), had a longer operation time (p < 0.001), had a longer duration of hospitalization (p < 0.001), had a higher proportion of conversion (p < 0.001), and had a higher incidence of postoperative complications (p < 0.001). Type 2 diabetes mellitus (T2DM) (RR = 1.701; 95% CI: 1.410–2.047; p < 0.001) and duration from admission to LC (RR = 7.072; 95% CI: 3.044–16.431; p < 0.001) were independent risk factors for conversion. Older age, T2DM, CRP, duration of symptoms before admission >3 m, and duration from admission to LC > 15 d were independent predictors of postoperative complications.
Conclusion
For patients younger than 65 years without contraindications, early operation should be performed within 3 d after admission to reduce the operation time, hospitalization time, conversion, and postoperative complications.
Keywords
Introduction
The number of gallstone diseases is constantly growing worldwide. 1 Overall, approximately 10%–20% of adults carry gallstones in the United States. 2 Although the incidence of cholecystolithiasis in patients with symptoms only affects up to 1%–4% per year, 3 it is still a frequent and high-cost problem. Once gallstones are embedded in the neck of the gallbladder, most will cause acute obstructive cholecystitis (AOC). Local inflammation of Calot’s triangle caused by gallbladder calculi incarceration (GCI) is more serious than that of general acute cholecystitis. The local anatomical structure is unclear, and the operation is more difficult in GCI. Thus, most patients with GCI require emergency surgery. 4
In the past two decades, the progress of laparoscopic cholecystectomy (LC) has revolutionized the treatment of gallstones and acute cholecystitis. 5 Laparoscopic cholecystectomy treatment can not only shorten the recovery time but also reduce the cost of treatment. 6 Laparoscopic cholecystectomy has become the first choice for the treatment of cholecystolithiasis. 7 However, many problems persist in treating GCI with LC. The main cause is that GCI is often accompanied by acute inflammation of the gallbladder, easily leading to hydrops of the gallbladder, edema of the gallbladder wall, gangrene, and even perforation. 8 In recent years, with the continuous development of laparoscopic technology, GCI treatment has become a critical choice. Therefore, the choice of operation time is the key factor in determining the degree of difficulty and success of the operation.
However, no consensus exists on the optimal timing for LC to treat GCI. This study aimed to retrospectively investigate the impact of different durations of symptoms before admission and durations from admission to LC on the conversion to laparotomy and postoperative complications. We hope to provide insights into both clinical practice and study design for the treatment of GCI patients in the future.
Method
Study design and sample size
In this single-center retrospective cohort study, the clinical data of GCI patients treated at Tianjin Nankai Hospital from July 2018 to July 2020 were collected. By analyzing the clinical data of GCI patients with different durations of symptoms before admission or durations from admission to LC, the optimal operative time and factors affecting the conversion of laparotomy and postoperative complications were analyzed. This study was approved by the Hospital Ethics Committee of Tianjin Nankai Hospital (Ethics number: NKYY_YXKT_IRB_2019_004_01). All treatments and assessments were performed after informed consent was obtained from the patients in accordance with the Declaration of Helsinki.
Before the study, we first calculated the minimum sample size. According to the retrospective cohort study, the sample size calculating software G power (3.1.9.6; Franz Faul, University Kiel, Germany) was used to determine the minimum sample size for which the test level α was 0.05 and the degree of assurance 1 - β was 0.95. The minimum number of samples was 395 subjects.
Inclusion and exclusion criteria
1. The inclusion criteria were as follows: (1) patients diagnosed with GCI (sudden onset right upper quadrant pain, and cannot relief in 48 h, GCI confirmed by emergency ultrasound, CT, or MRI); (2)a diagnosis of AOC based on Tokyo Guidelines 2018 criteria, which comprised local, systemic clinical manifestations (Murphy’s sign, tenderness in right upper quadrant, nausea, vomiting, and fever), and imaging evidence (thickened gallbladder wall, stones, enlarged gallbladder, edema, and abscess)9; (3) age ≥18 years; and (4) benign lesions of the gallbladder. 2. The exclusion criteria were as follows: (1) Charlson comorbidity index ≥4 and the American Society of Anesthesiologists physical status classification ≥3; (2) combined with nervous system and respiratory system insufficiency; (3) jaundice (total bilirubin ≥35.4 μmol/L)10; (4) complicated with intrahepatic and extrahepatic bile duct stones, and acute pancreatitis.
Subjects
In total, 789 GCI patients were admitted to our hospital from July 2018 to July 2020. All the patients were diagnosed with GCI by ultrasound or CT. Among the 789 patients, 52 had undergone percutaneous transhepatic gallbladder drainage, and 41 were discharged with drainage tubes because they could not tolerate the operation (poor nutritional status, severe cardiovascular diseases, hemorrhagic disease, and anesthesia contraindications). Thirty-five patients had undergone laparotomy after admission. And, the symptoms disappeared after non-invasive treatment in 22 patients. They also had no intention of operation or could not tolerate the operation. The flowchart of this study is shown in Figure 1. Flowchart of this study. GCI, gallbladder calculi incarceration; LC, laparoscopic cholecystectomy.
Finally, 639 LC patients were included in this study, including 304 (47.57%) male and 335 (52.43%) female patients, with an average age of 55.2 ± 13.19 years (range, 18–82 years). The operation time of all the subjects was 20–323 min, with an average of 73.9 min. The average length of stay was 7.7 days (range, 1–49 days). The history ranged from 5 h to 30 years.
Grouping method
1. The subjects were divided into the following four groups according to the duration of symptoms before admission: (1) < 3 d group, 165 (25.82%) patients; (2) 4 d–14 d group, 129 (20.19%) patients; (3) 15 d −3 m group, 154 (24.10%) patients; (4) > 3 m group, 191 (29.89%) patients. 2. All the subjects were also divided into the following three groups according to the time from onset to operation: (1) LC < 3 d group, 204 (31.92%) patients; (2) LC 4 d–14 d group, 341 (53.36%) patients; (3) LC > 15 d group, 94 (14.71%) patients.
Collection of clinical data
The clinical data of each group were collected, including the sex and age of the patients, preoperative laboratory examination (the highest result), ultrasound imaging examination, the operation time (measured from the introduction of anesthesia to the position of the last suture on the skin), duration of hospitalization (calculated from the date of admission to discharge), conversion rate of operation to laparotomy, and incidence of postoperative complications. Conversion to laparotomy was measured as a percentage of the total number of laparoscopic operations. If Calot’s triangle cannot be displayed within 30 min after the start of the operation, conversion to laparotomy will occur. Moreover, conversion was considered when there was no progression.
The subjects were required to return to the clinic for follow-up at 7 d and 1 m after surgery. The incidence of postoperative complications was followed up. For patients with complications, extended follow-up times were performed.
Operation
The subjects were admitted to the hospital for standard perioperative management. Patients with high levels of total bilirubin (>34.2 μmol/L) or common bile duct >8 mm underwent magnetic resonance cholangiopancreatography (MRCP) or endoscopic retrograde cholangiopancreatography (ERCP) to exclude bile duct stones. After the preoperative examination and comprehensive condition evaluation, LC was performed, and the gallbladder was completely removed.
Statistical analysis
The statistical description of categorical data used the constituent ratio, and comparisons between groups were carried out using the chi-squared test or Fisher’s exact test. The statistical description of quantitative data used one-way ANOVA. Multivariate logistic regression analysis was used to analyze independent risk factors for conversion and positive complications, and dummy variables were used to analyze the effect of the duration of symptoms before admission and duration from admission to LC on conversion and positive complications. The statistical significance level was α = 0.005, and SPSS software (version 20.0; SPSS Inc., Chicago, IL, USA) was used for statistical calculation.
Results
Characteristics of all patients
Characteristics of all the subjects in this study.

ALP, alkaline phosphatase; ALT, alanine transaminase; BMI, body mass index; CRP, C-reactive protein; LC, laparoscopic cholecystectomy; T2DM, type 2 diabetes mellitus; WBC, white blood cell.
Prognosis of subjects with different durations of symptoms before admission
Characteristics of the subjects with different durations of symptoms before admission.

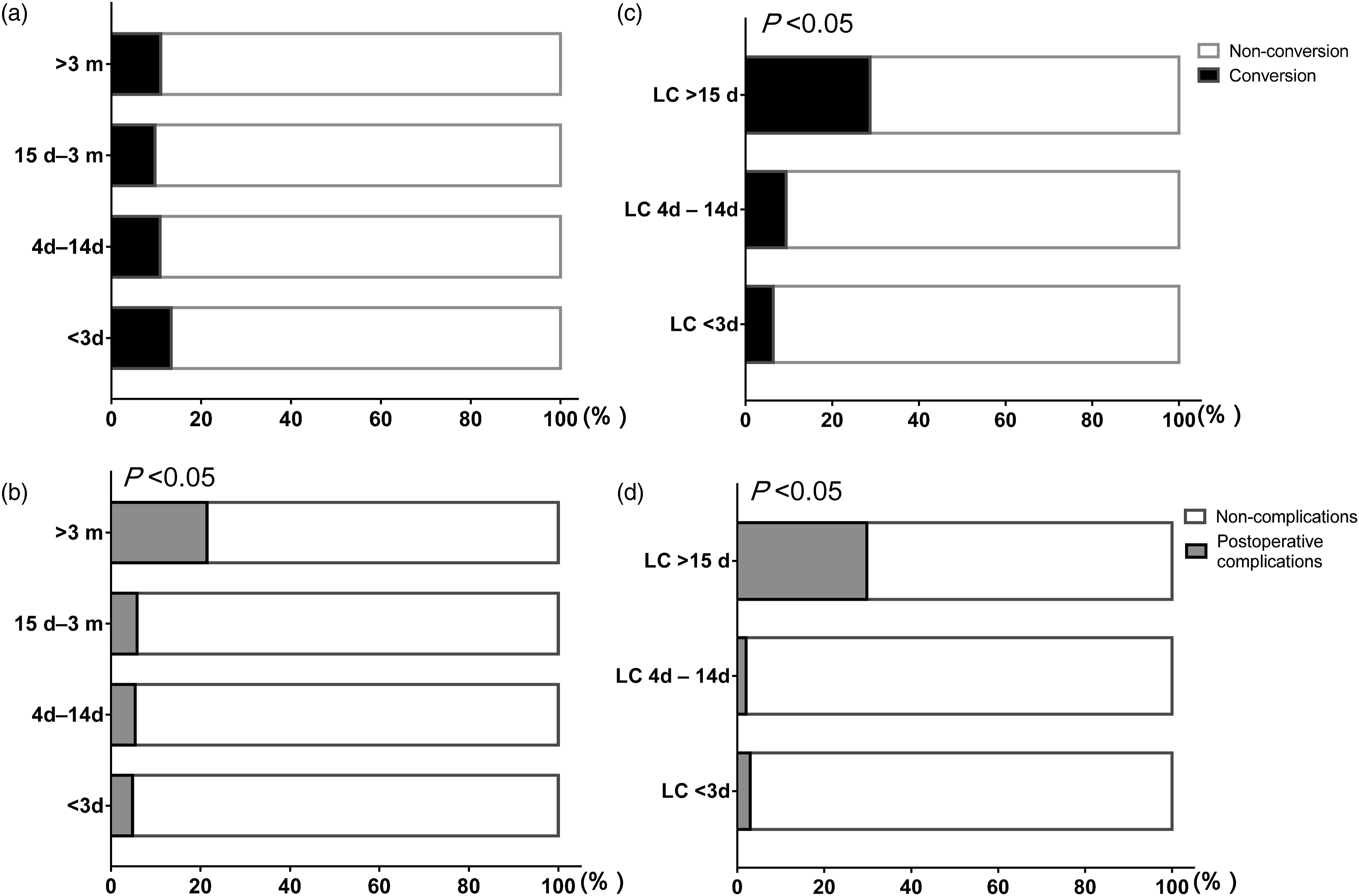
Percentage of subjects with conversion or postoperative complications. A. Conversion for different duration of symptoms before admission. B. Conversion for different durations from admission to LC groups. C. Postoperative complications for different durations of symptoms before admission. D. Postoperative complications for different durations from admission to LC groups.
Prognosis of subjects with different durations from admission to LC
Characteristics of the subjects with different durations from admission to LC.

Independent risk factors for conversion
Univariate and multivariate logistic analyses for independent risk factors for conversion.

Independent risk factors for postoperative complications
All the subjects were divided into two groups according to the incidence of complications within 30 d after the operation: the postoperative complication group (n = 65) and the no-complication group (n = 574). In the present study, infection was the most common postoperative complication (n = 38, 58.46%), including pneumonia (n = 21), superficial surgical site infection (n = 11), urinary tract infection (n = 4), and other infections (n = 2). According to the Clavien–Dindo classification, most postoperative complications were Grade I–II.
Univariate and multivariate logistic analyses for independent risk factors for postoperative complications.

Discussion
Laparoscopic cholecystectomy has become the standard procedure for the treatment of GCI. The main concerns are safety and feasibility, which are reflected in the risk of conversion and postoperative complications. Our study found that a long duration of symptoms before admission and a long duration from admission to LC were strongly associated with conversion and postoperative complications for subjects with GCI. Therefore, LC should be performed as soon as possible for GCI patients.
The optimal time of cholecystectomy is already known. However, because of the particularity and scarcity of GCI, no large sampling volume study is available. Cholecystitis caused by GCI can make it difficult to identify the cystic duct, common hepatic duct, cystic artery, right hepatic artery, and right hepatic duct. Also, the congestion and edema around the gallbladder and gallbladder triangle are serious in GS incarceration patients. Therefore, LC has a high risk and is prone to bile duct injury, vascular injury, bleeding, and other serious complications. So the operation of GS incarceration is more difficult than routine cholecystectomy. Previously, AOC was considered a contraindication for LC.11,12 However, with the development of surgical techniques, AOC is no longer the absolute contraindication for LC. 13 We retrospectively studied the clinical data of 639 GCI patients with LC. According to the right upper quadrant pain physical examination, emergency ultrasound, CT, and MRI, all GCI patients were newly diagnosed. To our best knowledge, our study is the largest sample size study on GCI.
To explore the optimal timing for LC to treat GCI, we conducted hierarchical analysis according to the time from onset to operation and duration of symbols before administration. In our study, 204 patients were treated with LC within 3 d after admission. The conversion rate in the LC < 3 d group was lower than that in the LC > 15 d group. The postoperative complications were also lower. Additionally, the operation time and hospital stay in the LC < 3 d group were lower than those of the other two groups. An RCT study on the operation time for AOC patients who had received LC showed that the patients who had received early operation (within 72 h) had a longer operation time, but lower conversion and complication rates, and a shorter hospital stay, than those who had received LC after conservative treatment for more than 1 week. 14 Thus, for patients who meet the operation indications, LC can be performed early after excluding operation contraindications.
However, the subjects in the LC < 3 d group were significantly younger than those in the other groups. Therefore, for the elderly, carefully assessing the risk of LC is necessary, and early treatment should not be blindly pursued. Studies have shown that experienced physicians and standardized techniques can reduce intraoperative risks and postoperative complications. 15 According to our experience, accurate identification of the gallbladder triangle can improve the outcome and prognosis of LC. The natural history of cholecystitis caused by GCI was 2 weeks to 3 months. In the acute stage of GCI, edema subsided, gallbladder swelling reached a balance, and the surrounding inflammation was completely wrapped. Even if gallbladder perforation occurs, diffuse peritonitis does not appear. In this case, most patients consider themselves “recovered,” and some are less willing to undergo surgery; they prefer to wait for the next acute attack before deciding to accept surgery. Therefore, the fact that 532 (83.26%) cases in this study had thinner gallbladder walls is understandable.
The literature data show that 2%–15% of LCs are converted for various reasons. 16 Most of the reported conversion rates are approximately 5%. 17 The rate of conversion to open surgery for GOC patients in the present study was 11.27% (72/639), which was high. Because of gallbladder wall fibrosis, the thickness of the muscular layer, nonobvious edema of the serosa layer, and the formation of a fibrous adhesion cord around the gallbladder, the gallbladder must be separated layer by layer to be exposed. After exposure of the gallbladder, Calot’s triangle is mostly fused with the common hepatic duct and common bile duct, and most of the serous layer and muscularis mucosa layer can be separated. The serous layer should be reserved on the surface of the right hepatic artery, right hepatic duct, and common hepatic duct to prevent injury to important vessels and the hepatic duct. The Hartmann bag is closely adhered to the right side of the common bile duct, making it difficult to be peeled off. If the situation is challenging, the gallbladder should be excised from the neck so that part of the gallbladder wall remains on the side of the common bile duct, the inner cavity of the cystic duct should be confirmed, and the cystic duct should be sutured. For type II Mirizzi syndrome, we suggest to switch to laparotomy in time, preserve the posterior wall of the gallbladder, and repair the common hepatic duct and common bile duct. Considering many variations of obstructive cholecystitis exist after compression of GCI, CT or MRI should be used to detect the situation of cystic duct entering the common bile duct and the course of bile duct before operation.
The incidence of postoperative complications was 10.17% (65/639). However, compared with previous studies, the incidence of postoperative complications is relatively low because of the absence of GOC, which is approximately 3.6%–7.7% as reported previously. 18 Using univariate and multivariate logistic analyses, we also showed that the incidence of postoperative complications was higher in older patients, patients with a longer duration from admission to LC, and patients with a longer duration of symptoms before admission. Many studies have shown that if early LC cannot be performed, LC can be considered after 6 weeks of onset, with high safety.19–21 However, incarceration of gallstones in the neck of the gallbladder causes chronic obstructive cholecystitis and changes in surrounding structures, including scar contracture of the gallbladder triangle tissue and abnormal adhesion, leading to changes in the anatomical structure and causing improper treatment during surgery and serious complications. In the present study, patients with a duration of symptoms before admission of more than 3 months were included, and the incidence of postoperative complications was increased. The reasons may be that the Hartmann bag of the gallbladder pressed the gallbladder bed for a long time, the local inflammation of the gallbladder was stimulated for a long time, and the gallbladder atrophied, resulting in severe scarring of the gallbladder triangle and significant shortening of the cystic duct (less than 5 mm).
This study has limitations. First, because of the retrospective nature of the study from a single center, the study may not be representative of all patients. In the process of retrospective analysis, there are differences in the age of patients in different groups, which may lead to heterogeneity among patients and bias in the results. We performed a propensity score matching study according to the age of patients and show the results in the Supplement Tables because the results of propensity score matching study are consistent with the present results. Moreover, we want to emphasize that the duration of symptoms before admission and duration from admission to LC were longer for older patients. Therefore, more attention needed to be paid to the older patients; second, the size and incarceration position of the gallbladder neck stones are findings that are difficult to visualize in each case; third, the history of the patients ranged between 5 h and 30 years. These findings indicate that patients with chronic cholecystitis symptoms that are probably complicated with the onset of acute cholecystitis were also included. This issue brings about the possibility of bias in patient selection. Finally, because our hospital is a top hospital for gallbladder diseases in our region, the characteristics of the patients included were more typical, and more patients with a duration of symptoms before admission >3 m were included. Therefore, prospective multicenter verification is needed to confirm our findings.
Conclusion
The incidence of postoperative complications is high when the incarceration time of gallstones in the neck of the gallbladder is more than 3 months. Early operation (within 3 days after admission) should be recommended for patients younger than 65 years without surgical contraindications, leading to not only reduced operation and hospitalization times but also a reduced incidence postoperative complications and a reduced conversion rate.
Supplemental Material
sj-pdf-1-eji-10.1177_20587392211051945 – Supplemental Material for Optimal timing for laparoscopic cholecystectomy in the treatment of gallbladder calculi incarceration
Supplemental Material, sj-pdf-1-eji-10.1177_20587392211051945 for Optimal timing for laparoscopic cholecystectomy in the treatment of gallbladder calculi incarceration by Jian-Heng Bao, Yu-Jie Wang, Hai-Tao Shang, Cheng-Fei Hao, Jun-Jian Liu, De-Lin Zhang, Shu-Wang Han and Zhong-Lian Li in European Journal of Inflammation
Footnotes
Authors' contributions
All authors contributed significantly to this study. JH B, YJ W, and ZL L designed the trial. HT S, CF H, JJ L, and DL Z conducted the work and were involved in data collection. JH B, YJ W, JJ L, and ZL L analyzed the data. SW H, YJ W, and ZL L interpreted the data. JH B and YJ W wrote the manuscript. All the authors revised the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Scientific Research Projects in Key Fields of Traditional Chinese Medicine of Tianjin Health Committee (2019003).
Ethics approval
Ethical approval for this study was obtained from the Ethics Committee of Tianjin Nankai Hospital (Ethics number: NKYY_YXKT_IRB_2019_004_01).
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
This randomized clinical trial was not registered because the retrospective observational study nature of the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.