
Abstract
Acalculous cholecystitis caused by gallbladder torsion is a rare condition. Only 500 cases have been reported since the first diagnosed case in 1898. We present the case of a 89-year-old woman with sudden onset of severe epigastric pain, radiating across her right costal margin, associated with nausea. Her abdomen was soft, mildly distended, Murphy’s negative but with epigastric tenderness and palpable mass. Computed tomography and ultrasound demonstrated significant acute cholecystitis, with the common bile duct measuring 7 mm. Due to the patients’ comorbidities, conservative treatment was initiated, until she was becoming increasing worse, so a laparoscopic cholecystectomy was performed. The operation revealed gallbladder torsion causing complete gallbladder necrosis and perforation with intraperitoneal biliary spillage. Gallbladder torsion should be a high differential if an elderly female patient presenting with sudden onset of abdominal pain, tender epigastric/right upper quadrant mass and a distended gallbladder on imaging. A laparoscopic cholecystectomy must be performed promptly to reduce the likelihood of gallbladder rupture and reduce the mortality and morbidity associated with this condition.
Introduction
Acalculous cholecystitis accounts for 2%–15% of acute cholecystitis cases and is diagnosed as gallbladder inflammation without evidence of gallstone cystic duct obstruction. 1 Gallbladder torsion (GT) is a rare cause of acalculous cholecystitis which was first diagnosed in 1898, 2 with approximately 500 cases reported since 3 and an incidence of 0.1% in patients with acute cholecystitis. 4 GT occurs more commonly in elderly females and is associated with increased morbidity and mortality if diagnosis is delayed. 3 Here, we report a case of an elderly female patient who was successfully treated for acute necrotising acalculous cholecystitis as a result of GT.
Case presentation
A 89-year-old woman presented with sudden onset of severe epigastric pain, radiating across her right costal margin towards her back. The pain was associated with nausea but no vomiting, bowels had opened the day before, no association with food and no other symptoms. The patient had a background medical history of a previous upper gastrointestinal bleed, gastro-oesophageal reflux disease, hiatus hernia, chronic constipation, hypertension and emphysema. She was a non-smoker and non-drinker.
Physical examination revealed a mildly distended, soft abdomen with normal bowel sounds, marked epigastric tenderness and palpable mass in epigastrium; Murphy’s negative. Vital signs were within normal limits and she was afebrile. Blood biochemistry was essentially normal: bilirubin 5 µmol/L, alkaline phosphatase (ALP) 41 U/L, gamma-glutamyl transferase (GGT) 31 U/L, alanine transaminase (ALT) 15 U/L, aspartate transaminase (AST) 20 U/L, C-reactive protein (CRP) 2 mg/L, white cell count (WCC) 11 × 109/L and lipase 18 U/L. Computed tomography (CT) imaging revealed significant acute cholecystitis, associated with a moderately dilated gallbladder (4.5 cm diameter), thickened gallbladder wall, pericholecystic free fluid and fat stranding (Figure 1). An upper abdominal ultrasound done the following day revealed acute acalculous cholecystitis with the common bile duct measuring 7 mm in diameter, no intrahepatic duct dilatation and did not report on blood flow.
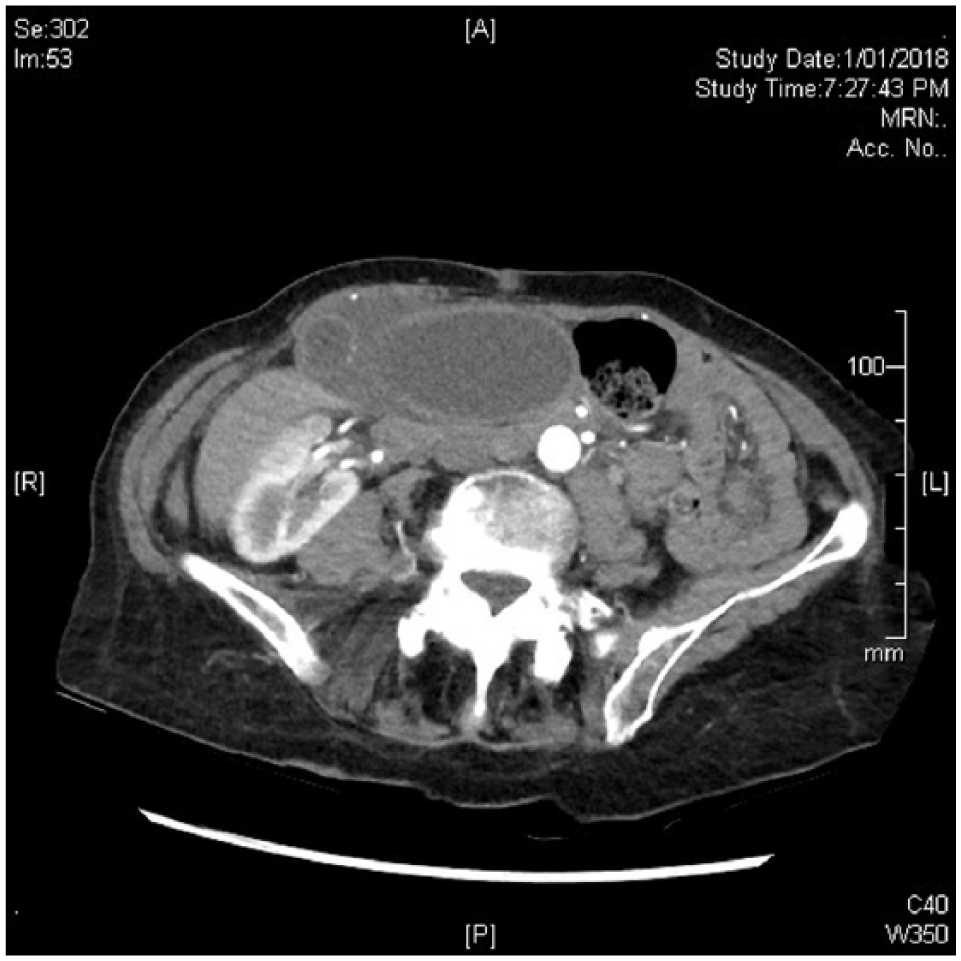
Computed tomography image demonstrating significant acute cholecystitis, associated with a dilated and thickened wall gallbladder plus pericholecystic free fluid and fat stranding.
Her ASA-PS (American Society of Anesthesiologist Physical Status) score was III and CCI (Charlson comorbidity index) score was 5, which made her a high-risk surgical candidate. Therefore, she was initially treated conservatively as acute cholecystitis with intravenous antibiotics, until day two post-admission she become increasingly unwell and underwent a laparoscopic cholecystectomy. Operative findings were of a pedicled, suprahepatic gallbladder on a narrow cystic duct stalk which appeared acutely torted with consequent complete gallbladder necrosis and perforation (Figure 2). Intraoperative cholangiogram demonstrated normal biliary anatomy, long cystic duct and nil dilation or filing defects. Histopathology showed features of acute necrotising cholecystitis, without gallstones, a large amount of haemorrhagic fluid in lumen and two areas of stricture in the region of the gallbladder neck (19 and 34 mm from cystic duct margin). The patient was discharged 5 days after the operation.

Intraoperative photo demonstrating gallbladder (GB) torsion and associated GB necrosis. Note position of GB situated upon the diaphragmatic hepatic surface instead of within the GB fossa. Also note the thin and suspended GB pedicle which contained both the cystic duct and artery, and which was the axis of torsion, thus producing resultant GB ischaemia.
Discussion
GT is a rare and potentially life-threatening condition if not promptly diagnosed and treated. Since GT was first diagnosed in 1898, 2 approximately 500 cases have been reported 3 and occurs at a rate of 0.1% in patients diagnosed with acute cholecystitis. 4 GT is a result of the gallbladder becoming pedunculated, with its only attachment to the liver by the cystic mesentery; this phenomenon is referred to as ‘floating gallbladder’. 2
The gallbladder can rotate either clockwise or anticlockwise. The most common direction for torsion is clockwise and is thought to be related to gastric (clockwise) or colonic (counterclockwise) peristalsis. 5 The degree of torsion determines the severity of GT. Type I is less than 180 degrees, allowing limited blood supply, and type II is more than 180 degrees, causing complete obstruction. 6 The gallbladder can undergo infarction, gangrene and/or perforation, when blood supply is affected.
Case studies over the years have reported numerous risk factors, signs, symptoms and investigations to help diagnose GT. Elderly patients are at greater risk of the gallbladder becoming separated from the liver, due to loss of visceral fat and elasticity with increasing age. 7 Clinical findings indicative of GT include sudden onset of abdominal pain, early emesis and tender mass in the right upper quadrant. 8 When comparing the biochemistry of acute cholecystitis and GT, GT often has normal liver function and biliary enzyme but elevated inflammatory markers. 9 Preoperative imaging usually involves a CT scan demonstrating a distended gallbladder, with high attenuation and a circular structure to the right of the gallbladder. 10 GT can theoretically be ruled out if a Doppler ultrasonography shows normal blood flow. 11 A more reliable diagnostic test is a magnetic resonance cholangiopancreatography (MRCP). The findings positive for GT include gallbladder fundus towards the abdominal centre, V-shaped extrahepatic duct and cystic duct torsion.5,9 Although we are aware of the above points of diagnosis, the pre-operative diagnosis of GT is not commonly achieved and is not diagnosed until a cholecystectomy is performed.
This case report demonstrates the importance of keeping the differential diagnosis of a GT at the top of the list in an elderly female with acalculous cholecystitis. In hindsight she had clinical and radiological signs suggestive of GT, which could have lead us to perform an MRCP for a prompter diagnosis. Early diagnosis or suspicion of GT can lead to a more rapid definitive treatment (cholecystectomy) and reduce the risk of the potentially fatal sequel of gallbladder necrosis and perforation.
Conclusion
When a patient suffers from sudden onset of abdominal pain, a tender epigastric mass and a distended gallbladder on imaging, the differential diagnosis of GT must be kept in mind to reduce morbidity and mortality. A laparoscopic cholecystectomy must be performed promptly to reduce the likelihood of gallbladder rupture.
Footnotes
Acknowledgements
N.S. and S.P. oversaw the diagnosis and clinical care provided to the patient. B.E.W., J.T. and N.S. performed the literature review and wrote the manuscript. All authors read, edited and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Informed consent was obtained from the patient for the publication of this case report and accompanying images.