
Abstract
The ‘2023 AAFP/IAAHPC Feline Hospice and Palliative Care Guidelines’ are authored by a Task Force of experts in feline hospice and palliative care convened by the American Association of Feline Practitioners and the International Association for Animal Hospice and Palliative Care. They emphasize the specialized communication skills and ethical considerations that are associated with feline hospice and palliative care, with references to other feline practice guidelines for a more complete discussion of specific diseases, feline pain management best practices and cat friendly interactions. A comprehensive, multi-step hospice consultation allows for tailoring the approach to both the cat and the family involved in the care. The consultation includes establishing ‘budgets of care’, a concept that greatly influences what can be done for the individual cat. The Guidelines acknowledge that each cat and caregiver will be different in this regard; and establishing what is reasonable, practical and ethical for the individual cat and caregiver is important. A further concept of the ‘care unit’ is introduced, which is extrapolated from human hospice and palliative care, and encourages and empowers the caregiver to become a part of the cat’s care every step of the way. Ethical considerations include a decision-making framework. The importance of comfort care is emphasized, and the latest information available about how to assess the quality of a cat’s life is reviewed. Emotional health is as equally important as physical health. Hence, it is fundamental to recognize that compromised physical health, with pain and/or illness, impairs emotional health. A limited discussion on euthanasia is included, referring to the AAFP’s End of Life Educational Toolkit for recommendations to help the caregiver and the veterinary professional ensure a peaceful passing and transition - one that reflects the best interests of the individual cat and caregiver.
Keywords
Introduction
Hospice and palliative care for cats address the physical, psychological (emotional) and social needs of patients with long-term and/or life-limiting diseases. 1 Familiarity with best practices in communication skills, how to provide a hospice/palliative care consultation, and comfort care options is essential to meet the needs of feline patients and their caregivers. It is important to recognize that compromised physical health, which may include pain and/or illness, impairs emotional health. Bond-centered care, which meets the non-medical needs of people while simultaneously meeting the medical needs of their cats, protects, strengthens and honors the human-animal bond, and is fundamental to reaching the goals of feline hospice and palliative care.
Hospice and palliative care definitions
Hospice and palliative care have been a growing field within veterinary medicine since the early 2000s. As human hospice and palliative care have evolved and the human-animal bond has strengthened over time, cat families have embraced similar end-of-life philosophies of care for their cats.
✜
✜

Unit of care
One of the fundamental shifts for the veterinary team in hospice and palliative care work is the expansion of the ‘unit of care’. Rather than the feline patient being the sole focus of care, the care unit includes caregivers and their needs. Utilizing this approach pairs veterinary professionals with social workers, charities and mental health professionals to facilitate open communication about treatment preferences and goals of care. That is one of the foundations of contemporary end-of-life care. End-of-life care requires an interdisciplinary approach, as veterinary teams alone are not trained to deliver care to, and cater to the psychological, social and spiritual needs of, people. Other members of the interdisciplinary hospice and palliative care team can include groomers, cat sitters, clergy, extended family members and various members of the veterinary team who are familiar with the cat, including general practice veterinarians, specialists, veterinary technicians, and dedicated hospice and palliative care providers.
Honoring the human-animal bond is one of the central guiding principles of hospice and palliative care. A primary goal of care is ensuring the relationship between the cat and their family is not strained or severed during the intensive caregiving that can be required during the end-of-life stage. A commonly cited motivating factor for many veterinarians in the hospice and palliative care field is helping to provide the family with support throughout the end-of-life journey, and after the loss of their cat, so that they are able to process their grief in a healthy manner and might consider adopting additional cats in the future. The strength of the human-animal bond prompts more and more families to seek out hospice and palliative care services. Allowing that bond to guide decision-making and caretaking empowers the cat’s family and ensures they are steering the process to meet their cat’s needs and their own needs. The ‘five-step hospice and palliative care plan’ (see later) is designed with this bond-centered care in mind.
Ethical considerations
Hospice and palliative care embrace an inherent set of values to help eliminate and prevent suffering, but end of life is also an area that is both spiritually and morally complex. Veterinary professionals assist families with different views about the appropriateness of ending a life. Language continues to be developed in the feline hospice and palliative care field that is specific to end-of-life care. ‘Hospice-assisted death’ or ‘palliated death’ are terms that veterinary professionals are just beginning to use, to further clarify how they can assist in improving a cat’s quality of death if a family elects not to pursue euthanasia. Previously, many used the term ‘natural death’, which can carry connotations that may impact family decision-making. Continuing to make further refinements to language used in veterinary medicine is crucial to help minimize miscommunication and moral quandaries in end-of-life care.


The ‘four box’ method combines four foundational principles of clinical bioethics to assist clinical decision-making. QOL = quality of life.
Feline hospice and palliative care case management, and dialog with the caregiver and care unit, should be guided by four foundational principles of clinical bioethics. Bioethics is the study of ethical, social and legal issues that arise in medicine and biomedical research. Clinical bioethics grounds ethical decision-making in medical practice. The four principles are:
✜
✜
✜
✜
Figure 1 illustrates how these bioethical principles (described in more detail below) are combined into the ‘four box’ method to assist clinical decision-making. The four principles do not comprise a unified ethical theory, but rather provide a framework within which to consider a specific patient or case. Applying this bioethical framework to hospice and palliative care decision-making requires balancing between the principles to decide what is in the best interests of the patient. When applying bioethical principles to cats receiving end-of-life care, veterinary professionals accept the limitations presented by beings that cannot self-report on their own behalf, while striving to achieve optimal outcomes for them (minimizing pain and providing a peaceful death). The individual cat receiving hospice and palliative care must be considered carefully (see box ‘Cats deserve moral consideration’).

Bioethical principles
Respect for autonomy
Respect for autonomy, as applied to clients, is the obligation of the veterinary professional to articulate, in language understandable by the cat’s caregiver, the information needed for that person to make the best decision on behalf of the cat. When expected outcomes are explained clearly and completely, including the risks and benefits, caregivers can make informed choices among treatment options. Respecting the caregiver’s autonomy is supported in a number of ways. These include: the veterinary team’s truthfulness during discussion of the cat’s condition and prognosis; respect for the caregiver’s values, culture and confidentiality; obtaining consent before proceeding with any treatment; and assisting with decision-making when asked.
Respect for the patient’s autonomy means considering the cat’s disposition or temperament, receptiveness to interactions and willingness to take medications - essentially the cat’s willingness to participate in their own care. Forcing medications or painful wound care on a cat that is expressing a fear-anxiety emotional response and that may exhibit protective behaviors, violates the autonomy the cat can express (albeit ultimately the cat is unable to actively choose specific end-of-life care). In addition, imposing such care can rupture the bond between the cat, caregiver and wider care unit. Finally, even though it is an elusive concept, respecting the cat’s will to live is part of respecting autonomy. A QOL scale and scoring system can provide a strategy for the cat’s caregiver and care unit to apply a level of objectivity to a very subjective aspect of the cat’s circumstances (see later discussion of ‘Other tools’).
Non-maleficence and beneficence
Non-maleficence and beneficence are intertwined in feline hospice and palliative care. For the cat’s caregiver and care unit, these principles translate into avoiding the harms inherent in incomplete or insensitive communication by veterinary professionals, and instead providing the benefit of open and honest discussions about the cat’s prognosis and costs of care. For the feline hospice and palliative care patient, both non-maleficence and beneficence support decisions around procedures or interventions. On balance, the benefits of proceeding must clearly outweigh any potential harms or burdens to the cat. Each step of the palliative care plan must be evaluated for its positive or potentially negative impact on the cat.
Non-maleficence and beneficence are aligned with the cat’s willingness to participate in the care being provided. While cats may not anticipate or fear their own death, they can and do anticipate and fear pain.7,9-12 Pain associated with interactions, administering medications or treatment must be considered, anticipated, identified and prevented whenever possible. In the face of ongoing pain in a dying cat that cannot be palliated by continued imposition of care, both non-maleficence and beneficence must drive a discussion about humane euthanasia in order to relieve suffering.
Justice
The bioethical principle of justice implies fairness towards a cat’s caregiver, the wider care unit, and the cat entered into hospice and palliative care. A reflection of bioethical fairness would be for the veterinary team to provide all parties with their very best efforts, regardless of the caregiver’s background and the cat’s previous care history. Fairness supports consideration of the caregiver’s financial resources, commitment to the treatment plan, willingness to embrace the necessary flexibility inherent in hospice and palliative care, and compliance with care recommendations. Fairness also supports treating individual cats based on their preferences for medical interactions and acceptance of treatment.
Bioethical framework
All four foundational bioethical principles can and should play a role in providing a framework within which to take a systematic approach to feline hospice and palliative care. In addition to influencing direct care decisions, bioethics supports dialog with a caregiver about the expected illness trajectory for their cat’s specific condition, thereby helping to mitigate the risk of an unanticipated outcome. Illness trajectories are generalized patterns that particular diseases tend to follow. 13 Four patterns have been identified: 14
✜
✜
✜
✜
Illness trajectories emphasize how important it is for the veterinary team to understand all of the disease influences on a particular patient.
Communication
The impact of placing a beloved cat into hospice and palliative care is nothing short of profound, and one that is likely to stay with the caregiver forever. As veterinary professionals, it is critical to understand the psychological/emotional consequences of this care. To make the experience as positive as possible, it is important for veterinary teams to communicate in ways that will minimize caregiver distress.
Effective communication between the veterinary team and a cat caregiver fosters trust. It is the foundation for establishing the goals as well as the treatment plans for hospice and palliative care. Veterinarians and their teams need to understand a cat caregiver’s needs, beliefs, goals and budgets (ie, financial, time, physical and emotional), all of which will have been shaped by the caregiver’s life experiences, both positive and negative. This understanding has numerous benefits. It strengthens communication, improves the veterinary-client-patient relationship, enhances trust and respect for the veterinarian’s recommendations, influences the selection of diagnostics and treatments, improves the efficiency of care (especially important with time-sensitive issues), helps put caregivers at ease, reduces the emotional side effects for the members of the care unit, and minimizes the potential conflict that could arise between the veterinarian and the patient’s family.
It is important to be observant and ask the appropriate questions during the initial consultation (see box ‘Important information to gather’). Caregivers need to feel listened to and, likewise, feel safe to share what could be very personal information about their beliefs, family dynamics and finances. It is essential for communication to be compassionate and non-judgmental.
Diverse roles of the veterinarian
When communicating with the cat caregiver and other members of the care unit, the veterinarian (and/or members of the veterinary team) may assume diverse roles - expert, expert guide, partner or facilitator. The expert role is assumed when the veterinarian identifies a diagnosis and educates the care-giver about the patient’s disease trajectory. The expert guide’s role is assumed, for example, when a veterinarian aids the euthanasia decision-making process and then accompanies the caregiver through the procedure. When the veterinarian communicates as a partner, the caregiver should feel supported regardless of the caregiver’s choice of care that their cat will receive. As a facilitator, the veterinarian works to make the caregiver’s agenda a reality. Aligned communication occurs when members of the care unit are in the appropriate role.
Guiding the caregiver through the palliative care consultation
The veterinarian should start the consultation with open-ended questions (‘What…?’, ‘Where…?’, ‘When…?’, ‘Who…?’, ‘Why…?’, ‘How. ?’) or indirect statements, such as, ‘Please describe/explain/tell me about …’.
The caregiver’s body language during the conversation should be observed. For example:
✜ Is the caregiver moving away from the veterinarian? This could mean they are uncomfortable or too stressed to be receptive.
✜ Is the caregiver overtly protective of their cat? This could mean the caregiver may need more time to accept what is being communicated or may need more emotional support.
✜ Is the caregiver avoiding eye contact? This may mean that the caregiver is uncomfortable, although it could be related to a cultural difference or emotional state, for example.
When a veterinarian must share information that can be upsetting for the caregiver, offering a signpost or ‘road map’ of where the conversation is going can be beneficial. Some examples of signposts are:
✜ ‘I am worried about what I am seeing here.’
✜ ‘We are finding ourselves about to experience a big change.’
✜ ‘We are going to have some hard decisions to make.’
✜ ‘We are facing a challenge.’
✜ ‘Your cat is going to need us more than ever before.’
✜ ‘We are approaching a new chapter in his/ her life.’
These statements open up the conversation to go in a specific direction. As the conversation continues, rather than rotely moving onwards, ask for permission to do so (eg, ‘Are you ready for me to continue?’). Asking a question such as, ‘Would it be helpful for you to hear about…?’ helps to create a safe space for the caregiver. Using the ‘chunk and check’ technique, 16 which breaks down big pieces of information into manageable bite-sized ‘chunks’ and combines this with ‘checks’ along the way (eg, ‘Do you follow what I’ve just shared?’), prevents information overload and positively impacts the way a caregiver understands and retains the information. It is important for the veterinarian to establish a mutually understood common ground by using a back-and-forth communication style (including recognizing, endorsing and acknowledging statements) that encourages feedback and collaboration.
Relationship-centered care and goals of care
Two further concepts that are valuable in the context of the palliative care consultation are ‘relationship-centered care’ and ‘goals of care’.17,18 Relationship-centered care emphasizes shared decision-making once the veterinarian has fulfilled their bioethical obligation to educate the caregiver about the patient’s condition in terms the caregiver understands. In their study examining this approach - engagingly framed as ‘Being nice is not enough’ - Kuper and Merle (2019) 17 stressed that it reaches for a balance of power between the veterinarian and the caregiver during the decision-making process. They go on to say that imbalances from either direction - either a paternalistic approach with power on the veterinarian’s side, or a ‘customer-like’ attitude in the caregiver, reducing the veterinarian to the position of a simple provider - increase the risks of dissatisfaction and inefficient patient healthcare.
Conversations on the goals of care are an essential component of palliative care for human and animal patients alike. 18 Widespread implementation of high-quality goals-of-care conversations is a keystone for advancement of palliative care. One of the most important aspects of properly structured goals-of-care conversations is that they provide dependable support for caregivers to navigate their cat’s illness and engage in end-of-life decision-making. Multiple frameworks cover the communication techniques that clarify the caregiver’s understanding of their cat’s health status,19-21 and how, what and when they want information about it. These models have been shown to help both the caregiver and veterinary professional to manage the stress that frequently accompanies hearing or delivering bad news. They also have been shown to improve caregiver satisfaction with outcomes.
Key concepts shared by these various models are that the veterinarian needs to choose an appropriate setting and be prepared for the anticipated conversation. These are vital aspects for successful communication. The conversations should occur in a private place (a safe and comfortable environment) where there will be no interruptions and all stakeholders can be present. They should not be rushed. An effort should be made to find out what the caregiver knows about their cat’s condition (ie, the caregiver’s perspective) and how much information the caregiver wants - a lot, as in every possible detail, or just the ‘big picture’, as in an overview. Once the amount of information that a caregiver prefers is known, aspects of the cat’s medical condition and prognosis can be shared accordingly, noting that the diagnosis should be shared with any others only when permission has been sought from, and granted by, the care-giver.
When sharing, keep the terminology simple (use plain language) and explain any medical jargon if it cannot be avoided. Remember the chunk and check technique works well when there is a lot of information to be given, and also that it can be helpful to offer a warning that difficult news is coming (eg, ‘This might be hard to hear’). It is important always to be empathetic. Empathy - the ability to understand and share the feelings of another person emotionally - is a necessary part of any doctor-patient relationship, assuring the care-giver that you care about them. 22 Offer empathetic statements such as, ‘As a veterinarian, it’s my top priority to provide the best care possible for your cat and ensure their well-being. Please know that I’m here to support you and your cat during this challenging time. Let’s work together to find the best treatment plan and give your cat the care they deserve.’ When imparting difficult news, it is best to be direct and straightforward, with compassionate transparency.
It is important to manage the caregiver’s reaction to the information they are receiving, so it is imperative to listen to their concerns and validate their emotions. Veterinarians need to ‘kindle’ emotions by allowing adequate space for them to flow. The conversation should conclude by summarizing what was discussed, addressing any questions or concerns that still remain, and acknowledging the plan of care with the next steps to be taken.
Caregiver’s communication preferences
The veterinary professional should become familiar with the caregiver’s communication preferences. A study by Englar et al (2016) 23 evaluating communication skills taught at a veterinary school revealed that:
✜ Cat caregivers value chunk and check, and signposting, more so than dog caregivers.
✜ Cat caregivers emphasize the need for empathy more so than dog caregivers.
✜ Cat caregivers appear to appreciate a focus on their cat when conversing with their veterinarian.
✜ Cat caregivers tend to use the pronoun ‘we’ to include their cat; in contrast, dog caregivers tend to use the pronoun ‘I’ when discussing concerns about their dog’s health.
✜ Cat caregivers can be viewed as caretakers vs dog caregivers as masters.
✜ Cat caregivers appear to be along for the ride as passengers, whereas dog caregivers appear to be the drivers that direct the course of the visit.
✜ Cat caregivers appear to accept the veterinarian taking the lead, provided that the veterinarian signposts the direction of the visit.
✜ Cat caregivers appear to prioritize communication skills as a means of lessening distress, distrust and fear, so as to limit transfer of negative emotions to their cat.
✜ Cat caregivers tend to see value in every member of the veterinary team. It matters less who on the veterinary team reaches out to make contact, so long as someone does.
Five-step hospice and palliative care plan
The following five-step process serves as a foundation to help the veterinary team implement a consistently effective hospice and palliative care treatment plan for feline patients.
Step 1: Evaluation of the caregiver’s needs, beliefs and goals for the cat
For every family, the requirements of care-giving are different, and the intensity of caregiving is largely influenced by the severity of disease and by how far along the disease continuum their cat’s condition has progressed. Because of this, it is imperative that the veterinary professional explores the care-giver’s needs, beliefs and goals for their cat since the majority of care will rely on their active involvement, and this information will help determine the best course of treatment.
When evaluating these aspects with the caregiver, it is often helpful to frame conversations through ‘personal budgets’, which refer to the amount of financial, emotional, physical and time resources that a caregiver has available to them. 26 The following are examples of caregiver considerations as they relate to their individual personal budgets:
✜
✜
✜
✜
Understanding a caregiver’s needs, beliefs and goals requires the use of open-ended exploratory questions from the veterinary professional, and a mix of experience/goal sharing from the caregiver. Discussion should focus on personal budgets, how to achieve a balance between quality and duration of life for their cat, goals for their cat’s treatment and care, and whether euthanasia or hospice-assisted death is the preferred option. The caregiver should be invited to ask questions and should not feel rushed or pressured into making treatment decisions. Regardless of the decisions that are made, the caregiver should never feel judged.
Step 2: Education about the disease process and delivery of care
The main goal of caregiver education in hospice and palliative care is for the caregiver to have a clear understanding of all diagnostic and treatment options to ensure the cat’s comfort, as well as the expected trajectory of the cat’s disease and the prognosis. The more a caregiver understands, the better they will be able to execute their role within the unit of care with realistic expectations and make informed decisions based on goals. The veterinary team should communicate information using language that the caregiver can easily follow and understand, and decisions around care should be made only when the caregiver has a clear understanding of all options available.
Caregiver education with regards to the delivery of their cat’s care should involve various forms of instruction, including verbal, written and visual (ie, illustrations, video), whenever possible. When giving instruction on particular care tasks, such as subcutaneous fluid administration, take a ‘see one, do one, teach one’ approach to caregiver education.

Step 3: Development of a personalized plan for the cat and caregiver
Developing an effective, patient-specific hospice and palliative care treatment plan (Figure 2) is a collaborative effort involving the veterinary team, caregiver and entire unit of care, and includes the following components:
✜ An assessment of the caregiver’s capability and willingness to assume specific responsibilities for care.
✜ An assessment of the patient’s willingness and capacity to receive care.
✜ A detailed written plan presented in a way that the caregiver can clearly understand.
✜ An estimate of the time required to provide the level of care needed for their cat.
✜ An estimate of costs, including costs of recheck appointments, additional diagnostics, medication and supplies.
✜ A schedule for follow-up communication and reassessment.
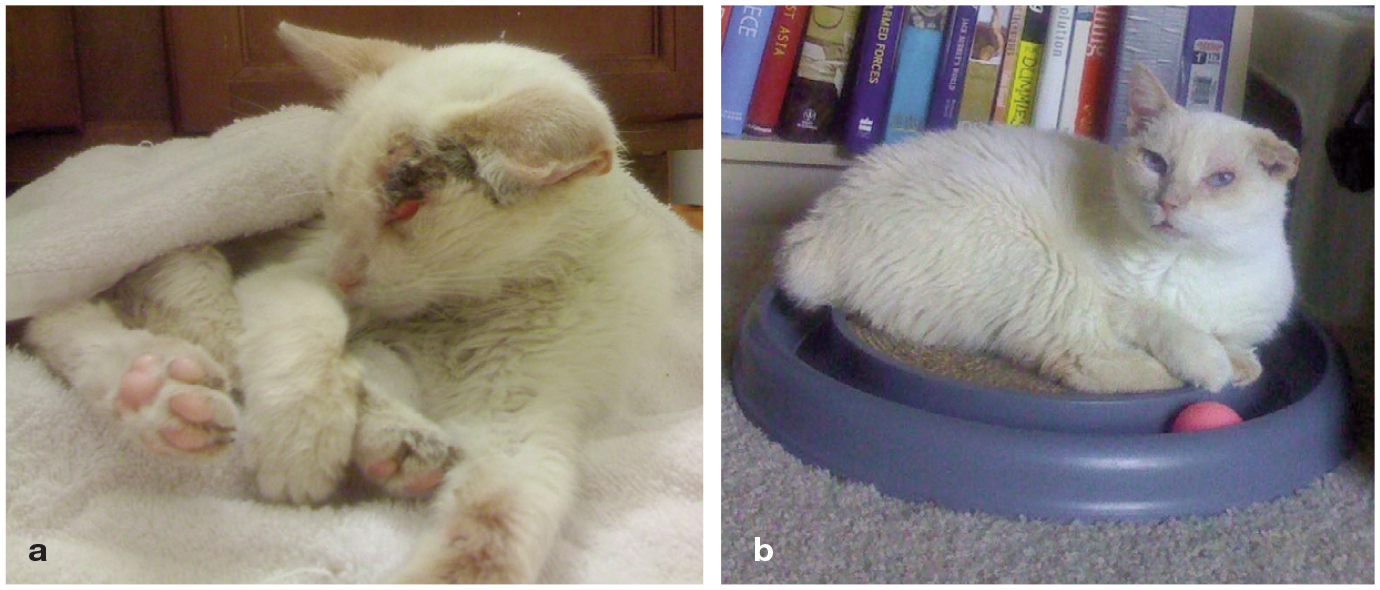
(a) Feline patient before a personalized hospice and palliative care plan was put in place. (b) The same patient after the implementation of a complete care plan, including adequate pain control, nutritional support and comfort care. Images courtesy of Clara Showalter and Katrina Breitreiter
It is helpful to approach creation of the care plan in terms of three critical areas - the physical, emotional and social needs of the individual patient. The box ‘Caregiver discussion points relating to the cat’s needs’ provides a summary for assessing/addressing each of these areas.
Step 4: Application of hospice or palliative care techniques
A hospice and palliative care plan empowers the caregiver to care for their cat in a home setting. To a large extent, execution of the care plan involves instructing the caregiver on various therapeutic techniques, as well as on how to assess their cat’s response to therapies and treatments, and how to recognize signs of clinical decline.
The caregiver should be guided in how to provide safe interactions with and handling of their cat, including how to safely administer treatments such as subcutaneous fluids and medications. Administering medication should be a positive experience (eg, providing oral medication in treats) or followed with a positive experience such as an engaging human-cat interaction. The home environment should be evaluated to ensure the cat’s comfort and safety, with adaptations made where necessary. Environmental modifications might, for example, include improving accessibility of food and water, ensuring that bedding is comfortable, optimizing litter box location and design, selecting an ideal ambient temperature or providing an approved heat source.
Technologies such as asynchronous communication through video recording or synchronous communication utilizing tele-health can be helpful for the caregiver in regularly communicating with the veterinary team regarding the patient’s clinical status.
If at any point in the hospice care relationship a caregiver wishes to decline diagnostics or treatment for their cat, it is critical to avoid making them feel guilty and instead support them in this difficult decision. Moreover, if, say, a caregiver decides against monitoring blood work every 3-4 months to assess their cat’s chronic kidney disease, this does not mean ceasing medical treatment required for supportive care, such as fluids or other medications. Measures should always be taken to ensure the family feels supported and comforted in the decisions they make.
Step 5: Emotional support during the care process and after the death of the cat
Provision of emotional support and empathy begins at the point of the family’s first realization that they are entering their cat’s end-of-life stage, and should be the responsibility of everyone within the veterinary practice. During the course of the hospice care relationship, it is important to continually explore whether care-givers are experiencing anticipatory grief, which is a form of grief that occurs before an impending loss. Anticipatory grief includes all of the same stages (denial, anger, depression, acceptance) as post-mortem grief, and can make decision-making challenging. It may manifest as rehearsing the loss, and meticulous following of instructions or obsessive monitoring. 27 Disenfranchised grief, described by Dr Kenneth Doka in 1989, 28 is something many caregivers experience as well. Often, they are grieving alone or do not get the emotional support they need because their family members, friends, co-workers or acquaintances do not feel the grief that they experience is legitimate.
Encourage grieving caregivers to find the support they need and provide resources such as information about support groups. Often, just naming and normalizing anticipatory, post-mortem or disenfranchised grief goes a long way towards supporting caregivers and their families. For caregivers who are struggling with one or other form of grief, it is strongly recommended that the veterinary team considers a multidisciplinary approach to utilize the expertise of social workers and mental health professionals in providing support and expanding the unit of care. Most importantly, caregivers need to know that it is okay to feel what they are feeling; that is, their feelings need to be validated and supported.

Quality of life
‘How will I know it’s time?’ is one of the most frequently asked questions by caregivers. Partnering with them in making a decision to euthanize their cat is an essential part of the veterinarian’s job. Diseases and treatment-related effects both impact QOL. With more therapeutic interventions and radical surgical procedures now available to prolong life, the onus is on the veterinary team to put the patient’s best interests first, despite any pressure from caregivers. 26 Just because we can does not mean we should, and quality rather than quantity of life is a priority.
Cats live in the moment and, therefore, unlike people, cannot know that ‘tomorrow may be better’ while going through unpleasant treatments. Patients do not make choices for themselves; that falls on the caregiver as well as the veterinary team, who must partner with them to make good, well-informed patient-centric decisions. Integral to this, the veterinary team should ensure that everyone is on the same page by discussing what they actually mean by QOL (see box ‘How is QOL characterized?’).
Assessment of QOL is an essential component of palliative and hospice care, with the aim of determining if the individual patient has a life worth living. Because cats cannot self-report, QOL can only be assessed using direct observations; these may be performed by the caregiver, who knows their cat better than anyone, a veterinarian or a combination of the two, and are termed observer-related outcomes. Assessment can be challenging because QOL is an individual and subjective experience. Pain is an affective state (emotion) and is always unpleasant, but it is not the only unpleasant feeling associated with chronic disease. Other things to consider include nausea, thirst, breathlessness and fear-anxiety (Table 1). QOL assessment is discussed further in the ‘2021 AAFP Feline Senior Care Guidelines’ (available at catvets.com/senior-care). 26
Examples of physical, emotional and social factors that contribute to a poor QOL

DJD = degenerative joint disease; QOL = quality of life
Validated QOL instruments
Feline welfare issues, both on an individual and population level, have been prioritized by a panel of experts. 32 Pertinent to these Guidelines is that out of the top 10 welfare issues identified, diseases of old age were ranked second in priority, and delayed euthanasia was listed second for prevalence. The questions veterinarians should ask care-givers in relation to feline QOL ultimately depend on knowing what matters to them. QOL and HRQOL instruments serve two main purposes: one is to monitor the effectiveness of treatment interventions and the second is to help make decisions about euthanasia.
QOL instruments have been developed for cats with certain specific diseases: cardiac disease, 33 diabetes mellitus 34 and skin disease. 35 However, aging cats rarely have just one disease; therefore, validated generic HRQOL instruments are needed. 36 One such tool, a 20-item instrument that is completed by caregivers online, has been developed and reliably differentiates sick from healthy cats, and shows promise as an aid for tracking chronic feline diseases. 31 During development, cats with degenerative joint disease (DJD), cardiac, dental, renal, lower urinary tract and chronic gastrointestinal disease were included, in addition to cats with painful and non-painful cancer. The 20 items were allocated to three domains encompassing physical and emotional health: vitality, comfort and feline emotional wellbeing. This instrument is available for clinical use through NewMetrica (newmetrica.com) and is fee based.
Other tools
There are many tools available that are not validated by rigorous testing, but this does not mean they should not be used - engaging caregivers to track their cat over time is, after all, the main goal. These other tools include:
✜ Journeys Home Quality of Life Scale Calculator (journeyspet.com/pet-quality-of-life-scale-calculator).
✜ HHHHHMM Quality of Life Scale, created by Dr Alice Villalobos (vetsocialwork.utk.edu/wp-content/uploads/2016/03/Quality-of-Life.pdf).
✜ The Ohio State University QOL assessment (vet.osu.edu/honoringthebond).
Comfort care
Comfort care is a priority for the hospice or palliative care patient, and encompasses the physical, emotional and social needs of cats. This section of the Guidelines focuses on physical needs - in particular, pain recognition and provision of pain control. The cat’s emotional and social needs are the subject of the later section on ‘Feline emotional health’.
Impact of pain
Pain has a negative impact on the QOL of feline patients, and both acute and chronic pain may be experienced in the hospice and palliative care setting. Acute pain occurs during the normal inflammatory and healing stages after injury to tissues (eg, as a result of trauma, surgery, diagnostic procedures, acute medical conditions or diseases). Chronic pain persists beyond the normal healing time or may be caused by a condition where healing will not occur. 37 Chronic pain should be considered maladaptive because it does not serve any beneficial biological purpose and is persistent. 38
Most feline hospice and palliative care patients are likely to be affected by at least one painful condition. Potential sources of pain include, among others, DJD, cancer (including the primary tumor, metastases, diagnostic procedures or side effects of treatment), persistent postoperative pain (associated with onychectomy, other amputations, thoracotomy, etc), gastrointestinal conditions (eg, inflammatory bowel disease, megacolon, constipation), neuropathic disorders (eg, feline hyperesthesia syndrome, feline orofacial pain syndrome), trauma or chronic wounds, skin conditions (eg, chronic dermatitis, otitis), ocular conditions (eg, corneal disease, ulcers, uveitis, glaucoma), feline lower urinary tract disease (eg, feline idiopathic cystitis, urinary tract infections, urolithiasis, bladder neoplasia) and diabetic neuropathy. 38 The severity of pain experienced does not necessarily correlate with the severity of the lesion causing the pain, and in some cases the primary lesion or source of pain may not be identified.
Pain can alter feline behaviors, resulting in the patient being withdrawn or hiding more, and sleeping in abnormal positions, including being hunched. In addition, patients may show a decreased appetite, reduced movement or mobility, hesitation to jump or climb, diminished exercise and activity, difficulty rising, standing or walking, decreased grooming, changes in urination and defecation habits, squinting, increased sensitivity while being touched, and aggression. 37 These behavioral changes can have a negative impact on the human-animal bond. 38
Recognition of pain
Identifying and responding to pain in cats undergoing hospice and palliative care is in alignment with the foundational bioethical principles discussed above, and is a moral imperative for both veterinary professionals and caregivers. Indeed pain is considered one of the five vital signs for assessment as part of the standard physical examination in small animals, in addition to temperature, pulse, respiration and nutrition.37,39
Because cats are so adept at hiding pain, many caregivers may not realize their cat is experiencing discomfort. Providing caregivers with appropriate tools to help identify pain will improve the veterinarian’s ability to address this important issue. A few tools that have been validated for assessing acute and chronic pain in cats are highlighted below, and comprehensive lists can be found in Tables 4 and 7 of the ‘2022 WSAVA Guidelines for the Recognition, Assessment and Treatment of Pain’. 40 In addition, the ‘2022 AAHA Pain Management Guidelines for Dogs and Cats’ 37 and ‘2022 ISFM Consensus Guidelines on the Management of Acute Pain in Cats’ 41 provide in-depth practical recommendations, and the AAFP’s brochure ‘How do I know if my cat is in pain?’, available on its cat caregiver website at catfriendly.com/pain, helps guide caregivers in the recognition of feline pain.
Acute pain
At least three pain-scoring systems have been published and validated for cats. The UNESP-Botucatu multidimensional feline pain assessment scale short form (UFEPS-SF) is a checklist that relies on posture, comfort, activity, attitude and reaction to touching for pain assessment in relation to four specified items. 42 The Glasgow composite measure pain scale-feline (Glasgow CMPS-Feline) is a lengthier checklist that begins with observation of the undisturbed cat and includes assessment of facial features.43,44 The Feline Grimace Scale is a tool that evaluates five separate facial ‘action units’ (ear position, orbital tightening, muzzle tension, whisker position and head position) for evidence of pain; 45 this scale is available in the form of a downloadable phone app that veterinarians and cat caregivers may use to help identify acute pain.
Chronic pain
Several validated tools have been published to aid in the assessment of chronic (primarily DJD) pain in cats. The Feline Musculoskeletal Pain Screening Checklist (Feline MiPSC) is one such tool, 46 and has been adapted into a user-friendly, publicly available feline checklist (available at catredflags.com) that may be easily shared with cat caregivers. The Feline Musculoskeletal Pain Index (FMPI) is a questionnaire-based tool developed by the Comparative Pain Research and Education Centre at North Carolina State University. 47 Available at painfreecats.org, it measures the cat’s mobility, agility and disposition associated with chronic pain. Given that 90% of cats aged 12 years and older may be affected by DJD, 48 this checklist is likely a useful means of assessing hospice and palliative care patients for signs of chronic pain.
Modalities for pain mitigation (control)
Once pain has been identified, a multimodal approach to its alleviation should be implemented to improve patient outcomes (Figure 3). This allows pain to be addressed at multiple points in the pain pathway. Using a combination of different analgesics may allow lower doses of each individual drug to be given, reducing the potential for side effects. Complementary therapies, environmental modification and nutraceuticals all may be considered as part of a multimodal pain control plan. 37

(a) Hospice patient with a painful bleeding tumor. The photograph was taken prior to the implementation of pain control. (b) The same patient after receiving multimodal pain control using a combination of buprenorphine and gabapentin. Images courtesy of Clara Showalter and Katrina Breitreiter
Opioids
Opioids are commonly used for managing acute pain in cats and may play a role in managing chronic pain. 37 Pure mu (μ)-opioid receptor agonists, such as morphine, hydro-morphone, methadone and fentanyl, are potent drugs and are typically used during surgical procedures to control moderate to severe pain. The partial μ-opioid receptor agonist, buprenorphine, provides mild to moderate pain control and is now available in several longer acting formulations, including a transdermal formulation approved in 2022 in the United States by the Food and Drug Administration (FDA). The mixed μ-opioid receptor antagonist/kappa agonist, butor-phanol, has been shown to provide ineffective levels of pain control, particularly when used as a single-agent analgesic. Butorphanol can, however, be used for minor procedures associated with mild pain, such as venipuncture or cystocentesis, and has the advantage of being a good sedative. 38
Opioid medications are generally very well tolerated by feline patients. Side effects are rare, but include sedation, dysphoria, mydriasis, nausea, vomiting, gastroesophageal reflux, hyperthermia, bradycardia and respiratory depression. 41 Although most opioid drugs are likely to be too short acting to provide adequate pain control for feline hospice and palliative care patients in the home setting, oral transmucosal and longer acting formulations of buprenorphine or longer acting formulations of fentanyl (eg, patches) may be valuable in some hospice situations (Table 2).
Dosing recommendations for opioid medications in cats

IM = intramuscularly; IV = intravenously; NSAID = non-steroidal anti-inflammatory drug; SC = subcutaneously
NSAIDs
Non-steroidal anti-inflammatory drugs (NSAIDs) work by inhibiting cyclooxygenase enzymes in cell membranes, thereby decreasing the release of inflammatory mediators. 38 NSAIDs may be safely and effectively used for both acute and chronic pain management in cats. Adverse effects include anorexia, vomiting, diarrhea and gastrointestinal irritation. The potential for an adverse drug reaction may be minimized by utilizing the lowest effective dose and avoiding concurrent administration with steroid medications. Studies have been published demonstrating safety of long-term administration of NSAIDs to cats with stable chronic kidney disease in order to manage their DJD.50,51 Two NSAIDs, meloxicam and robenacoxib, have been approved for use in cats and may be considered for feline hospice and palliative care patients (Table 3). Although both drugs are labeled for long-term use in Europe and some other countries, there is currently no NSAID labeled for long-term use in cats in the United States, and any off-label usage must be thoroughly discussed with caregivers.
Dosing recommendations for NSAIDs in cats

NSAID = non-steroidal anti-inflammatory drug; PO = orally; SC = subcutaneously
Monoclonal antibody therapy
Monoclonal antibodies are a novel therapeutic agent for pain management in cats. Frunevetmab, a feline-specific anti-nerve growth factor antibody (Table 4), received FDA approval for use in cats in 2022. Nerve growth factor contributes to peripheral and central sensitization and its concentrations are increased in some painful conditions, including DJD and neoplasia. A double-blind placebo-controlled randomized study demonstrated both safety and efficacy of frunevetmab in the treatment of pain associated with DJD in cats. 52 The most common side effects included vomiting and soreness at the injection site.
Dosing recommendations for monoclonal antibody therapy in cats

SC = subcutaneously
Adjunct pain control agents
Additional pain medications, such as gabapentin, pregabalin and antidepressant medications, may be utilized to improve pain management in feline hospice and palliative care patients (Table 5). Gabapentin and pregabalin are calcium channel blockers that reduce neuronal excitability. Gabapentin and pregabalin have been demonstrated to reduce distress during transportation and examination, as well as reduce fear-anxiety during the visit.54-57 The recommended dose for gabapentin is 20 mg/kg55,56 or 100-200 mg/cat 54 given 2-3 h prior to transportation54-56 (use 50% lower dose in cats with reduced renal function 53 ). Pregabalin is labeled in Europe to reduce the fear-anxiety associated with veterinary visits and travel (5 mg/kg PO 90 mins prior to transportation). 57 More research should be conducted on the use of gabapentin and pregabalin for maladaptive/ neuropathic pain, as much more is known about the effects of these medications on reducing fear-anxiety. Amantadine is an N-methyl-D-aspartate (NMDA) receptor antagonist and is used to treat central sensitization.
Dosing recommendations for adjunct pain medications in cats

These agents are not intended as stand-alone pain medications, and should be used in conjunction with other analgesics. See text for details on pre-visit pharmaceutical use for gabapentin and pregabalin to reduce fear-anxiety CKD = chronic kidney disease; NMDA = N-methyl-D-aspartate; PO = orally
Integrative medicine in hospice and palliative care
Integrative medicine is the combination of Western medicine, and complementary and alternative medicine modalities (referred to as complementary alternative medicine [CAM] in veterinary and human medicine). A 2006 veterinary oncology study from Colorado State University involving 254 (dog and cat) caregivers showed that three-quarters (76%) used CAM therapies, with nutritional supplements being the most commonly used. Even at that time, more than half the caregivers expressed a strong interest in CAM (with 40% indicating average interest, and only 3% no interest). 58
The Academic Consortium for Integrative Medicine & Health, a human health organization, states that ‘Integrative medicine and health reaffirms the importance of the relationship between practitioner and patient, focuses on the whole person, is informed by evidence, and makes use of all appropriate therapeutic and lifestyle approaches, healthcare professionals and disciplines to achieve optimal health and healing.’ Distinct parallels can be drawn with end-of-life care for feline patients and their families: utilizing an inte-grative approach provides additional resources and tools to allow the hospice and palliative care team to refocus on those relationships and improve QOL for the feline patient. The box ‘Integrative medicine modalities to consider’ lists a range of possible therapies. It should be noted that dietary supplements do not require proof of safety, efficacy or quality control to be marketed; more generally, there are varying levels of scientific research supporting the use and efficacy of integrative medicine modalities in both humans and animals.


The three components of the feline physical environment.
Feline emotional health
Emotional health is as equally important as physical health, 59 and the two components of overall health are fundamentally linked. Compromised physical health, with pain and/or illness, impairs emotional health, increasing protective emotions, such as fear-anxiety, pain and frustration. 60 Pain, which is recognized to be both a sensory and emotional response (‘pain is not just how it feels, but also how it makes you feel’) 61 is considered part of the fear-anxiety system.59,62,63 Fear-anxiety can exacerbate pain, and pain increases fear-anxiety. 64 Minimizing perceived threats in the cat’s physical and social environment is therefore an essential component of pain management and of maintaining feline emotional health. 37
Emotional compromise is the cause of undesirable behaviors. 65 An environment that does not meet an individual’s essential needs based on their current health status compounds this situation. 66 Incorporating feline essential needs modified for hospice and palliative care patients enhances feline welfare.
Components of the cat’s physical environment
All cats, regardless of their health status, are territorial animals with strong protective mechanisms. Because of the compromised condition of hospice and palliative care patients, their need for a safe physical environment is critical.
The feline physical environment consists of three components: the home range, territory and core territory (Figure 4). The core territory, the smallest component, is the area that is safe for eating, sleeping, resting and playing. The territory is the area that cats will actively defend against invasion, while the home range is the entire area over which a cat roams. The size of the environment depends on access to the outdoors, the density and social groupings of the cats indoors and outdoors, and the individual cat’s temperament. 67 With impaired physical, emotional and/or cognitive health, all of which are common in hospice and palliative care patients, it is not uncommon for the environment to shrink. Impaired mobility may confine the cat to one floor of a home and prevent use of vertical space. Poor social relationships or changes in feline social groups will further reduce the environment. The environment may shrink to just one or two rooms, or even a portion of a room, such as a closet. Cats that previously had outdoor access may choose to remain exclusively indoors or limit their time outdoors.
Environmental modifications are often needed to provide safe outdoor access, if desired, and a safe indoor space where the patient can choose to be with (or separated from) certain people and other pets. Safe options for cats that enjoy and choose outdoor access include sitting in the sun with a person to monitor them, or resting in a secure outdoor enclosure (eg, catio), screened-in porch or sunroom. This continued provision of outdoor space can increase QOL even though the individual’s home range may be significantly smaller than it once was.
Within the home, resources for resting, sleeping, feeding, scratching and toileting need to be provided within the patient’s preferred areas. Often these areas are where caregivers spend most of their time (eg, living room and bedroom).
The five pillars of feline essential needs
The ‘five pillars’ framework, introduced in the 2013 ‘AAFP and ISFM Feline Environmental Needs Guidelines’, 68 and discussed below, identifies a cat’s environmental needs within their living situation. Each of the five pillars is essential to increase feline comfort and safety (Figure 5). Collectively, their purpose is to allow cats to maintain normal feline behaviors and minimize emotional distress and behavior problems. The goal for hospice and palliative care patients is to use the framework to educate caregivers about feline essential needs, and required modifications based on the patient’s impaired function and mobility.

The ‘five pillars’ framework, developed to describe a cat’s essential needs in the veterinary practice setting, applies equally to the cat’s home environment, and can help to guide caregivers in adaptations that might be needed to accommodate the particular needs of hospice and palliative care patients.
Cats in general prefer consistent and predictable environments, with resources positioned without changing their locations. If the patient, however, can no longer access these resources (eg, go down stairs), changes are required. Caregivers should be helped to recognize the need for safe and easy access to the patient’s favored areas and resources, with more than one entry/exit option to prevent tension with other cats or other undesired interactions. Meeting the environmental needs of cats leads to more engaging (positive) emotions and ensures that they can respond appropriately to protective (negative) emotions. One example might be a cat moving to a safe hiding area away from other cats with which they are not socially bonded. 60 Even cats that were previously bonded may have a breakdown of that relationship due to pain or frailty (a syndrome characterized by decreased functional reserve that leads to a decline in physiological and cognitive performance; 26 Figure 6).

(a) These two cats enjoyed a strong social bond for more than 5 years. (b) During the last stages of life, the orange tabby cat withdrew and no longer wanted to be near the other cat.
The veterinary team can successfully support caregivers to adopt the five pillars of essential needs and make modifications, as required, based on the individual patient and the home environment. Use of a home environment questionnaire identifies limitations that a cat might be experiencing (see ‘Hospice and palliative care patient questionnaire’ in the supplementary material). Home visits, where practical, facilitate the ability to identify specific environmental needs or modifications that might be necessary, and to educate caregivers accordingly. If not possible, photographs and videos of the cat’s environment can be helpful in developing a plan for modifications, bearing in mind that further adjustments might be needed over time.
Pillar 1: Safe place
A primary requirement for a territorial species is safe space. Safe resting and sleeping areas impart a sense of control, familiarity and predictability. Feline choice is also important, and a minimum of two resting options in different locations is desired. Hiding options, especially when a cat feels physically and/or emotionally compromised (eg, as a result of illness and fear-anxiety), as is common in these patients, increase the cat’s coping ability.69-72 Good options are those with sides that are high enough for cats to feel hidden, such as high-sided or igloo cat beds, a carrier, or a box that is only big enough for one cat (Figure 7). Cats often readily use carriers with soft bedding that are left open and placed in favored areas. The cat’s thermoneutral zone is higher than that of humans, with cats preferring an ambient temperature of 86-100.4°F (30-38°C). 73 Providing (safely) heated beds is especially important as a means of increasing comfort for less active and frail hospice and palliative care patients.

(a,b) A safe resting and sleeping area imparts a sense of control, familiarity and predictability, which is especially important for cats that are physically and/or emotionally compromised. Images courtesy of (a) Ilona Rodan and (b) Katrina Breitreiter
Critically, safe spaces and comfortable resting areas need to be provided in the location the cat prefers to spend most of their time, within their current core territory. Ask care-givers about changes in the cat’s use of space within the home and ensure that all resources are easily accessible (Figure 8). If negative changes in feline social relationships have occurred (Figure 6b), additional safe spaces are often necessary. Ideally, provide a minimum of one safe space per cat, plus one to allow choice.

All of the cat’s resources in the home should be easily accessible. (a) This cat has been provided with pet steps to help reach their bed. (b) A bench allows this cat to get to their favorite resting spot in the sun. Images courtesy of (a) Ilona Rodan and (b) Sheilah Robertson
In addition to frailty, the hospice and palliative care patient is likely to have other comorbidities that impair mobility, such as DJD and weakness. Cats often prefer elevated safe spaces from which to monitor the environment and, when compromised, to stay safe from young children and other cats. Provide recommendations on how best to support safe access to elevated areas, with the use of sturdy pet steps (Figure 8a) or ramps.
Educate caregivers also about the importance of rest and sleep. Disturbed sleep is detrimental to QOL and impacts an individual’s coping ability.74-76 It is the cat’s choice as to when and where to rest and sleep, and they should never be disturbed while doing so.
Pillar 2: Multiple and separated key environmental resources
Feline resources are food, water, litter boxes, resting and sleeping areas, scratching and toileting areas. Multiple resources should be dispersed throughout the home, and spaced apart (ie, with at least a few feet between them). In multiple cat households, there should be approximately one of each resource per cat - or at least per social group - to prevent competition for resources, with visual barriers (ie, a wall) and safe, easy access ensured. The ability to access each resource from two different locations is important, to prevent blocking by another cat or other individual. Caregivers should be educated in recognizing subtle signs of tension - staring, stalking and blocking. 77 Hallways, stairs and other narrow paths are common places where tensions arise, and all resources should be placed away from these areas.
Special accommodations for hospice and palliative care patients may be needed. All resources should be placed in their preferred environment; even though this may be small (eg, a single room), the requirement to separate resources still applies. If competition from another cat exists and that cat is allowed in the room, multiples of each resource should be placed in this location.
As pillar 1 addressed safe space, and feeding and hydration management are discussed later, the particular focus for the remainder of this section is litter boxes and scratching areas.
Litter boxes
Litter boxes should be placed in multiple locations, separated (both by distance and visually) from one another, and always away from food, water and resting areas. It is not uncommon for caregivers to prefer to place two or more litter boxes in the basement of their home, often side by side. Yet hospice and palliative care patients are likely to be frail, with impaired mobility, and may be experiencing pain. Even if keeping litter boxes downstairs worked before, it is critically important to ensure easy accessibility for these patients, which means keeping litter boxes on all levels of the home where the patient spends time, and away from noisy locations and other pets.
Cats prefer large litter boxes (preferably 26.8 in [68 cm] in length) that allow them to turn around, dig and eliminate. 78 As discussed, safe entry and exit is necessary, and litter boxes should be separated from other resources. There is study evidence to show that cats prefer to use clean boxes without solid materials. 79 As larger volumes of urine are often voided by these patients, scooping multiple times daily may be indicated, with thorough cleaning more often than previously (ie, as often as once weekly).
Many hospice and palliative care patients have difficulty entering and exiting litter boxes. At least one lip of the box should be lower (Figure 9) - a cement mixing box with its low sides makes a good option. Cats with DJD often have a few challenges, including getting to a litter box, entering and keeping urine within the box. Difficulty squatting often results in urine being deposited just outside the litter box. A dog litter box or large storage box with an opening cut out in the front to create a low lip and a high back (Figure 9a) prevents this problem. For the occasional patient that cannot walk into any litter box, placing puppy pads on the floor may aid in keeping the cat’s area clean.

Many hospice and palliative care patients have difficulty entering and exiting litter boxes. (a) At least one lip of the box should be lower. (b,c) A cement mixing box or storage box with its low sides makes a good option. Images courtesy of (a) Ilona Rodan and (b,c) Heather O’Steen
Additional resources can be found in the ‘AAFP and ISFM Guidelines for Diagnosing and Solving House-soiling Behavior in Cats’ 80 (available at catvets.com/house-soiling) and the ‘2021 AAFP Feline Senior Care Guidelines’ 26 (available at catvets.com/senior-care).
Scratching posts
Scratching is a normal feline behavior to help remove old claw sheaths, stretch muscles and mark territory. Dependent on the individual’s health, scratching behavior may range from none to increased scratching. With distress, for example, as may arise with intercat tension or inadequate environmental resources, scratching behavior increases, often associated with marking territory.81,82 Undesirable scratching on furniture or carpet may also occur due to a cat’s inability to use the scratching posts that were used prior to illness.
Scratching, where still possible, is an important behavior for hospice and palliative care patients, though cats should never be forced to scratch or punished physically or verbally for scratching in undesirable locations. Advise caregivers to promote scratching and claw care in desirable locations by providing options that cater to the patient’s abilities. A cat that can still scratch vertically should have a post that is long enough for a good stretch, with a sturdy base. Survey data have indicated that preferred textures are sisal rope and carpet.81,82 Moreover, cats 14 years and older were found to change their preference from vertical to horizontal posts on the floor due to discomfort associated with age-related DJD, and also preferred carpet over sisal rope and cardboard. 82 If scratching is occurring in undesirable areas, place specific and easily accessible scratchers in these areas. Additional information can be found in the AAFP’s Claw Friendly Educational Toolkit (available at catvets.com/claw-friendly-toolkit).
For those patients unable to scratch, more frequent nail care, including trimming, is often needed. Recognize that nails may be thicker and grow more quickly due to the cat’s inability to maintain claw care. Analgesia and anxiolytic medication may be needed to perform nail trimming to prevent fear-anxiety and pain. Although gabapentin and pregabalin function as both an anxiolytic and analgesic, they may not provide sufficient analgesia; where required, transmucosal buprenorphine can be used in conjunction with gabapentin (Tables 2 and 5). If the caregiver cannot perform claw care, consider veterinary or technician house calls.
Pillar 3: Play and predatory behavior
Play
If the cat is still interested in play, interactive play should be offered a minimum of twice daily to increase patient satisfaction and strengthen muscles. Most hospice and palliative care patients will no longer actively pursue wand toys, but may like the interactions and watching a toy move. If play is still enjoyable, it should be one-on-one and based on the cat’s energy level (Figure 10). A rare patient may enjoy watching young, healthy cats play, rather than engaging in play themselves.

If play is still enjoyable, it should be one-on-one and based on the cat’s energy level. Image courtesy of Ilona Rodan
Predatory behavior
Cats have evolved as solitary survivors, hunters and foragers - and are both predators and prey. The domestic cat maintains a strong instinct for predatory-type behav iors. Additional information and discussion on this can be found in the section on ‘Nutrition and hydration management in the hospice and palliative care patient’.
Pillar 4: Positive, consistent and predictable human-cat social interaction
The way in which veterinary teams and care-givers approach their interactions with cats, both non-physical and physical, is critical to the human-cat relationship and prevention of fear-anxiety, pain and frustration. Best practices for veterinary professionals during feline interactions are described in the ‘2022 AAFP/ISFM Cat Friendly Veterinary Interaction Guidelines: Approach and Handling Techniques’. 65 These, together with supplemental resources (including a helpful video for caregivers, ‘How to interact with your cat - the Battersea way’), are available at catvets.com/interactions.
Hospice and palliative care patients often desire increased human interactions, with massage and grooming being actively enjoyed by many. Regular human-cat interactions may also be necessary for the purposes of providing medication. Allowing the cat to remain in their preferred location for the interactions, and ensuring easily accessible hiding options are available in the room, are important. People have a tendency to want to pick up and snuggle cats, but it must be recognized that this is usually not preferred by cats, which favor having all four feet on a safe surface. Hospice and palliative care patients may need assistance to reach desired areas, and ramps and stable pet steps are preferable for cats that are sufficiently mobile. If a patient still needs to be moved, ideally move them within their cat bed or hiding area. Otherwise, if it is necessary to partially or fully pick up a cat to move them, loosely wrap a blanket or towel around their entire body, including their limbs, to do so safely.
Pain or declining health can alter a cat’s response to interactions, and caregivers should be instructed to note any differences and contact their veterinary team with any concerns.
Massage
Feline massage therapy may reduce musculo-skeletal and myofascial pain. 83 Most cats enjoy being massaged, but make sure that the interaction is well accepted, and avoid massaging over areas that cats do not like (ie, the belly or base of the tail).
Grooming
If cats are unkempt or matted and unable to groom themselves anymore, instruct care-givers to groom them to increase comfort and hygiene. Many cats are amenable to being groomed and enjoy the attention given during the process, particularly where combing or brushing has started at an earlier age. For cats not used to being groomed, encourage the caregiver to start with gentle and positive stroking with hands or a soft brush.
Mats in the coat should not be manually pulled out, as this is painful for the cat. Teach caregivers to trim small and tight mats by placing a comb between the skin and the matted fur to prevent accidental cutting of the skin. If heavily matted, professional clipping is ideal, with analgesia, anxiolysis and sedation provided prior to grooming. If there is fecal and/or urine soiling, a sanitary clip is helpful to keep the area clean. If washing is needed, unscented baby wipes should be used.
Medication administration
Hospice and palliative care patients often need analgesia, anti-nausea medication and other medical support to maintain QOL. While the ideal would be to introduce treats to hide medications before cats need them, this does not happen with many patients, with a recent study indicating that compliance with medication administration is only 76% because of the associated stress. 84 Client education is desired and necessary to help ease medication administration and hence minimize associated patient distress (essential not only for QOL, but also for the cat-caregiver bond). Medication administration should be positive and occur during calm times, utilizing minimally invasive techniques where possible. The box ‘Steps to minimize distress associated with medicating cats’ presents a number of practical recommendations aimed at addressing QOL of both the cat and the caregiver or veterinary team member administering the medication. One recent study suggests cats do not have a flavor preference; however, when comparing compounded medications in an oil base vs a water base, cats preferred the oil base. 85


Where possible, combining tablets in a gelatin capsule is a useful way of minimizing the frequency of administrations - so helping to preserve the cat-caregiver bond and patient quality of life when frequent medications are necessary. Image courtesy of Ilona Rodan
If patient distress and fear-anxiety associated with administration of medications is impacting the cat’s or caregiver’s QOL, this needs to be addressed. When appropriate, a feeding tube is an excellent and easy method for oral medication administration in addition to nutritional support (see section on ‘Nutrition and hydration management in the hospice and palliative care patient’).
Pillar 5: Environment respecting the cat’s senses
Pillar 5 in the original five pillars framework referred solely to the cat’s sense of smell. The ‘2022 ISFM/AAFP Cat Friendly Veterinary Environment Guidelines’ (available at catvets.com/environment) incorporated an adaptation of the fifth pillar to broaden the scope to include the cat’s other senses. 66 Cats use their keen senses to gather information about the environment to assess whether it is safe and familiar, or whether it presents a perceived threat.
✜
✜
✜
Nutrition and hydration management in the hospice and palliative care patient
Gastrointestinal signs, such as inappetence, weight loss, vomiting and diarrhea, are often taken into consideration when assessing QOL. Feline caregivers may feel that their cat’s QOL has declined if the cat is losing weight, not eating well, or is experiencing frequent vomiting or diarrhea. Control of nausea and appropriate appetite support are crucial for maintaining a good QOL, as is maintenance of adequate hydration and water intake.
Ensuring that feline hospice and palliative care patients take in adequate nutrition to maintain themselves can be challenging. Resting energy requirements and protein requirements actually increase in cats over the age of 11-12 years.26,88 Illness and injury likewise increase resting energy requirements. Inadequate nutritional intake can lead to frailty, which may exacerbate QOL concerns in cats of any age. 26
Feeding should never be forced - including, for example, by syringe feeding or putting food on the face or paws for the cat to lick off. These patients are often inappetent due to illness, pain and/or nausea, and forced feeding may serve only to worsen food aversion, nausea, pain and patient distress. Medications to address illness, pain or nausea are important components of care. If nutritional intake is insufficient despite medications, or if clients are unable to medicate their cats, feeding tubes are an excellent option.
Use of feeding tubes
Feeding tubes may increase QOL and benefit some cats, as well as create longer quality relationships with caregivers. As such, placement of a feeding tube can be considered comfort care. Once in place, the feeding tube may reduce stress by being used to administer medications, provide adequate nutrition and supplement fluids (Figure 12). The distress of forcefully medicating cats may otherwise outweigh the benefits of the medication being given when overall QOL and the cat-caregiver bond are taken into consideration.
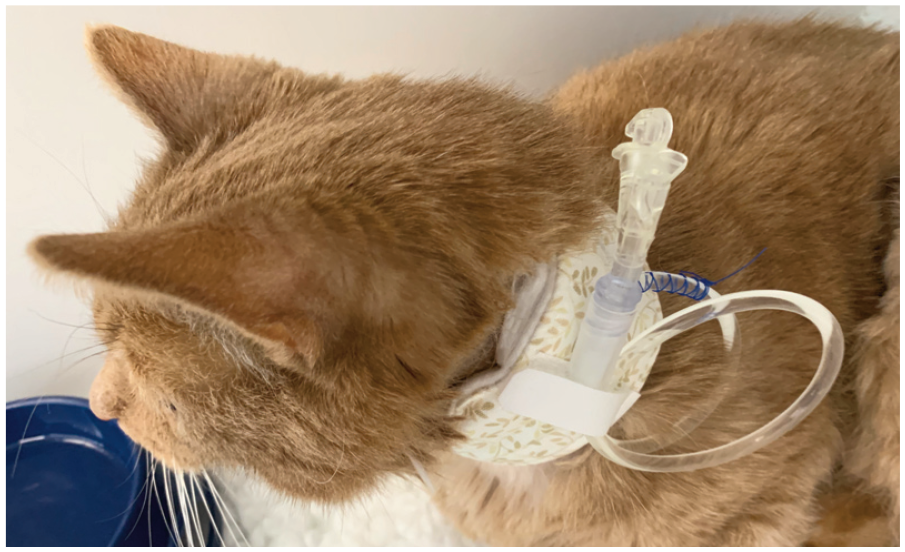
An esophagostomy tube may reduce stress by being used to administer nutrition, fluids and medication. The tube pictured here is covered with a soft padded collar. Image courtesy of Sam Taylor
Esophagostomy (esophageal) feeding tubes are generally well tolerated by cats, and may be left in place for weeks to months if cared for properly. If well enough, cats may still continue to voluntarily eat and drink, even with the tube in place. Soft padded collars are available to protect the tube and facilitate easy tube maintenance.
The advantages and disadvantages of tube feeding should be discussed with the caregiver as early as possible. While the surgical procedure for placement is brief, it necessitates general anesthesia, so the risks should be considered for each patient. When a tube is to be placed, it preferably should be used initially for provision of medication and hydration before nutritional support becomes a requirement. More broadly, a discussion covering caregiver personal budgets, how to achieve a balance between QOL and duration of life for their cat, and their goals for their cat’s treatment and care is likely to be valuable.
Further information on types of feeding tubes and factors influencing their selection, how to place a tube and check that it is positioned correctly, as well as managing complications, such as feeding tube obstruction and stoma site infections, can be found in the ‘2022 ISFM Consensus Guidelines on Management of the Inappetent Hospitalised Cat’, which are endorsed by the AAFP. 89 An accompanying guide for caregivers from ISFM’s parent charity, International Cat Care, available at bit.ly/aafp-feeding-tubes, can be used by the veterinary team to ensure that caregivers are well educated about how best to care for a cat with a feeding tube.
Feeding strategies
Where possible, cats should be willing participants in both feeding and medication administration, and there are various strategies that may be employed to encourage cats to voluntarily take in adequate nutrition, hydration and medications.
✜ Cats should always be fed separately, with visual separations, to prevent threat. Normal feline feeding behavior is eating small meals multiple times daily. 90 This is even more important in hospice and palliative care patients, as often stomach capacity is reduced.
✜ Dishes should be placed on the floor to prevent falls (eg, from countertops). Raised (shoulder height) food and water dishes are best if comorbidities such as DJD or other medical conditions make it uncomfortable for the cat to feed in a normal position (Figure 13).
✜ Although, in healthy patients, use of puzzle feeders is recommended to satisfy behavioral needs by simulating hunting, this must be weighed against the nutritional and caloric intake needed in hospice and palliative care patients.
✜ Caregivers should be educated to provide enticing food that is preferred by the patient. Cats over 7 years of age were shown to prefer warmed wet food, heated to 98.6°F (37°C) vs temperatures of 42.8°F (6°C) and 69.8°F (21°C). 91 Stronger smelling foods may appeal more to cats that have lost their sense of smell, either due to age or a medical condition. However, each cat has their own preferences, and options should be provided to confirm their choice.
✜ Flavor enhancers such as lickable treats, tuna juice or broth (without onions or onion powder) may promote appetite, but the goal is to enhance flavor and not feed so much that calories are diluted.
✜ A caregiver guide on inappetence from International Cat Care can be accessed at bit.ly/aafp-inappetence.

(a,b) Raising food and water dishes off the floor helps to provide a better feeding and drinking position for cats with degenerative joint disease and other comorbidities affecting mobility and comfort. Images courtesy of (a) Ilona Rodan and (b) Heather O’Steen
Hydration management
Many feline hospice and palliative care patients may be at risk of dehydration if good hydration management is not maintained. Strategies such as adding warm water to the cat’s food, offering multiple water sources in different locations (including water fountains or dripping faucets to provide running water) and separated from food and other resources, or using flavor enhancers (such as tuna juice or low-sodium chicken broth) may be utilized. Electrolyte-supplemented gravy packets have been shown to improve hydration status. In cases where their administration does not damage QOL or the cat-caregiver bond, at-home subcutaneous fluids may be considered.
Antiemetics
Because cats cannot self-report when they feel nauseous or are experiencing gastrointestinal upset, any cat that is vomiting or not eating well should receive a trial of antiemetic medication. Signs of nausea in cats are often subtle and may include licking of the lips, hypersali-vation, turning away from food, or trying to bury the food.
Maropitant is a central antiemetic that works through the blockade of substance P binding to the neurokinin-1 receptor. While very effective as an antiemetic, maropitant may not control nausea. Ondansetron is an antiemetic with 5-HT3 receptor antagonist activity in the central nervous system and gastrointestinal tract, which may be more effective for nausea. These medications are generally well tolerated in cats, with minimal side effects reported (Table 6).
Dosing recommendations for antiemetic medications in cats
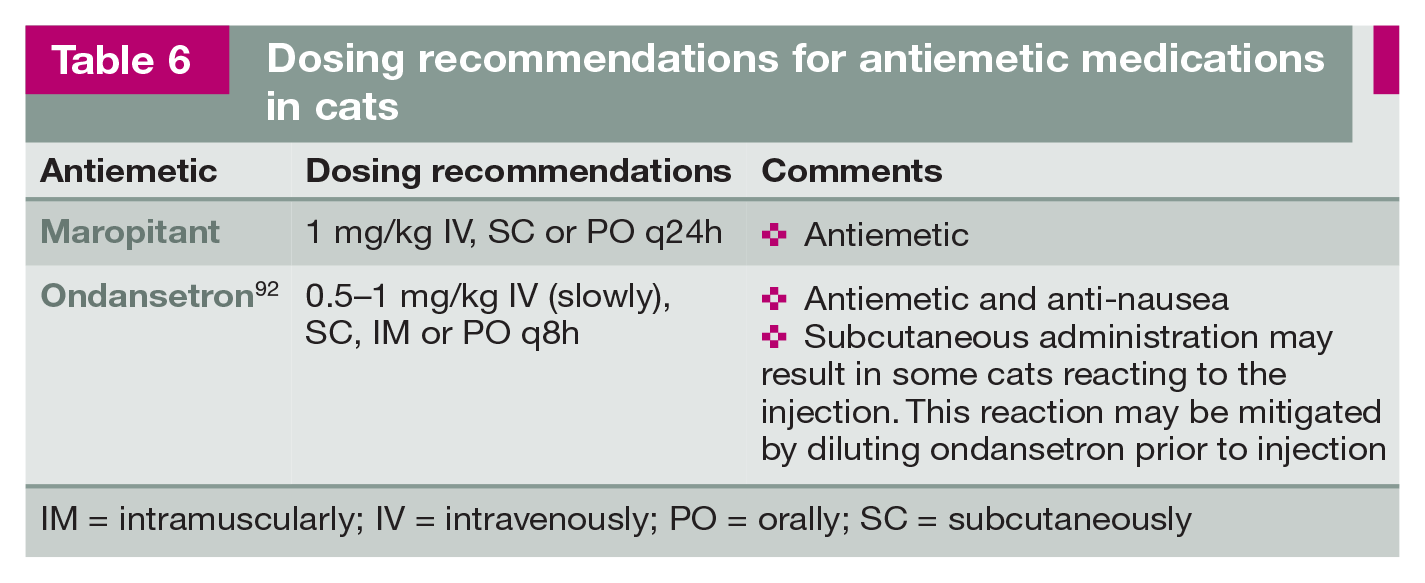
IM = intramuscularly; IV = intravenously; PO = orally; SC = subcutaneously
Appetite support
At the time of publication, there are two FDA-approved medications for appetite support in feline patients. Mirtazapine is a 5-HT3 receptor antagonist that has both an anti-nausea and appetite-stimulating effect. Mirataz (Dechra) is a transdermal formulation of mirtazapine approved for use in cats to manage unintended weight loss. Capromorelin is a ghrelin receptor agonist approved to increase appetite in cats with weight loss secondary to chronic kidney disease (Table 7). For additional information, see the ‘2022 ISFM Consensus Guidelines on Management of the Inappetent Hospitalised Cat’. 89
Dosing recommendations for appetite stimulants in cats

PO = orally
End of life
Following the practices outlined in these Guidelines can help ease the end-of-life journey of feline patients. Sadly, that journey will come to an end at some point. When the cat’s passing is planned with care and consideration, the outcome should be minimal pain and a peaceful transition. Being present with the caregiver and the patient is one of the last opportunities for a veterinarian and the veterinary team to serve the cat and the caregiver directly. The caregivers that are present for the procedure should be fully informed and aware of the steps that will be followed. The desire for death to come quickly and gently should not override the importance of allowing the caregiver(s) the time they need, and the team the opportunity to have everything in place.
Additional information and resources can be found in the AAFP’s End of Life Educational Toolkit (available at catvets.com/end-of-life-toolkit). The Toolkit aims to help the veterinary team to ensure a smooth, calm and compassionate experience for cats and care-givers alike. Advice and insights are offered on each step of the process, beginning with evaluating QOL, through to supporting the caregiver’s emotional wellbeing after the procedure. Details of bereavement and grief counseling services can be found in the client resources section of the Toolkit.
Conclusions
When the focus moves from curative care to providing comfort care, veterinarians and their teams should commit to the cat’s QOL leading up to death, which demands consideration of foundational bioethical principles. QOL assessments should center on whether the individual feline patient has a life worth living. The cat’s acceptance of treatments and medical interactions must weigh into care decisions. Cats can and do express preferences, and respecting their autonomy means respecting their expressed preferences as much as possible. Honoring and preserving the human-animal bond involves attention to non-maleficence (avoiding harm; ie, not harming the caregiver’s relationship with the cat) and beneficence (acting in the patient’s best interests; ie, allowing the human-animal bond to be a higher priority than intervening with aggressive procedures).
Veterinary professionals have the privilege and responsibility to improve patient welfare, which encompasses both physical and emotional health. The two are equally important and are intertwined - compromised physical health, with pain and/or illness, impairs emotional health and increases the likelihood of emotional compromise (eg, fear-anxiety, pain) and behavior problems. An environment that does not meet the individual’s physical and social essential needs based on their current health status compounds this situation. The five pillars of feline essential needs are key for a cat, to increase comfort and safety. The purpose of this framework is to allow cats to maintain normal behaviors, and minimize emotional distress and behavior problems.

The human-animal bond has strengthened over time, leading many cat caregivers to embrace human hospice end-of-life philosophies for their cats. Using the evidence-guided approach to feline hospice and palliative care covered in these Guidelines - a central component of which is the five-step hospice and palliative care plan - veterinary professionals can successfully meet the needs of patients that qualify for hospice and palliative care, along with meeting the needs and goals of their caregivers.
Summary Points
✜ The veterinary team’s bioethical obligations to the cat, the cat’s caregiver and wider care unit provide both a lens through which to consider all the diverse aspects of hospice and palliative care, and a formal framework within which to facilitate the shared decision-making that cats, their caregivers and their care units need and deserve.
✜ Hospice and palliative care, in all their dimensions, go beyond simple physiological considerations and include moral/ethical considerations as well. This is advocacy on behalf of beings who cannot advocate for themselves.
✜ Providing hospice and palliative care relies on excellent communication skills, which have been shown not only to lead to a more satisfying experience for the caregiver, but also a more satisfying experience for the veterinary care provider.
✜ The recognition and alleviation of pain and discomfort in feline hospice and palliative care patients is of paramount importance to improve and maintain a good QOL. A number of valuable resources may be used by veterinary professionals to aid caregiver understanding and recognition of feline pain.
✜ Incorporating feline essential needs modified for hospice and palliative care patients further enhances feline welfare. The goal is to educate caregivers about the five pillars of feline essential needs, and the adaptations needed to the home environment based on the patient’s impaired function and mobility.
✜ The ‘2023 AAFP/IAAHPC Feline Hospice and Palliative Care Guidelines’ present an evidence-guided approach by which veterinary professionals can successfully meet the needs of patients that qualify for hospice and palliative care, along with meeting the needs and goals of their caregivers.
Supplemental Material
Supplemental Material
Hospice and palliative care patient questionnaire
Supplemental Material
Caregiver brochure
‘Hospice and palliative care for your cat’.
Footnotes
Acknowledgements
These Guidelines were supported by an educational grant to the AAFP from Royal Canin. Contributions were provided by Daniel Dominguez and Heather O’Steen in the preparation of the Guidelines. The video in the supplementary material is provided courtesy of Mikel Delgado.
Supplementary material
The following files are available as supplementary material alongside the Guidelines:
✜ Hospice and palliative care patient questionnaire;
✜ Video - ‘Teaching your cat to get used to medication’;
✜ Caregiver brochure - ‘Hospice and palliative care for your cat’.
Conflict of interest
Ilona Rodan serves on an advisory board for Royal Canin. Members of the Task Force have also received financial remuneration for providing educational material, speaking at conferences and/or consultancy work; however, none of these activities cause any direct conflict of interest in relation to these Guidelines.
Funding
The members of the Task Force received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.