
Abstract
Objectives
The aim of this blinded, nested case-control study was to compare cats with and without early owner-reported mobility changes using subjective and objective outcome measures (owner-completed questionnaires, orthopaedic examination).
Methods
A total of 57 cats with and without early owner-reported signs of impaired mobility were allocated to the case (n = 30) and control (n = 27) groups, respectively. Participating owners completed one inclusion and two pre-visit questionnaires (Feline Musculoskeletal Pain Index, VetMetrica). Cats were then visited in their own homes, where they underwent an orthopaedic examination, an assessment of their body condition score and temperament, and the placement of an accelerometer on their collar for 2 weeks.
Results
There was no significant difference between groups for age category, breed, sex, temperament and body condition score. Case cats scored significantly lower for the Feline Musculoskeletal Pain Index (P = 0.003) and the VetMetrica domain of Comfort (P = 0.002), but not Vitality (P = 0.009) or Emotional Wellbeing (P = 0.018). Total pain (P <0.0001), crepitus (P = 0.002) and thickening (P = 0.003) scores were higher in case cats, as was the presence of bilateral disease (P = 0.005, odds ratio 14) and the number of bilaterally affected joints (P = 0.001).
Conclusions and relevance
Both the Feline Musculoskeletal Pain Index and orthopaedic examination were able to differentiate cats with early owner-reported signs of impaired mobility from healthy cats. VetMetrica Comfort domain scores indicated a compromised quality of life for cats with early owner-reported signs of impaired mobility compared with healthy cats. Being able to recognise signs of mobility impairment earlier would allow interventions aimed at slowing disease progression, thereby improving feline health and welfare.
Keywords
Introduction
Feline degenerative joint disease (DJD) has been established as one of the most common causes of chronic pain in cats. 1 The prevalence of DJD is strongly associated with age and is estimated to occur in 61–99% of cats of all ages according to radiographical studies.2,3 Clinical signs associated with DJD are difficult to identify, as domestic cats tend to hide signs of pain and disease, 4 and owners may consider DJD-related behavioural changes 5 a part of the natural ageing process. 6 The diagnosis of feline DJD is further hindered by the difficulty of assessing pain in cats and the lack of agreement between orthopaedic examinations and radiographical findings.7–10 Consequently, feline DJD may not be recognised in a significant number of cats, and untreated chronic pain is a welfare concern.
The Feline Musculoskeletal Pain Index (FMPI) is an owner-completed questionnaire used for the clinical assessment of DJD-associated chronic pain in cats which has proven validity and reliability.11–15 VetMetrica is an owner-completed questionnaire used for the assessment of the quality of life (QoL) in cats which has been shown to have good discriminatory validity and reliability in cats with or without comorbidities. 16 Actical is an activity monitor (accelerometer) that has been used in a plethora of studies investigating activity levels and different therapeutic interventions in cats with DJD.13,15,17–20 This device has been used to successfully differentiate healthy cats from cats with DJD and may also have the potential to objectively detect early signs of DJD in cats where the diagnosis has not yet been established.
Being able to recognise DJD-related signs earlier would allow interventions aimed at slowing DJD progression, thereby improving the QoL of cats with DJD. The aim of the present study was to determine whether owner-reported mobility changes were indicative of early DJD-related changes as evaluated by the FMPI and orthopaedic examination. A further aim was to investigate the effect of early DJD on the QoL of affected cats. We hypothesised that early DJD-related changes in owner-reported mobility would reflect joint health as evaluated by the FMPI and orthopaedic examination, and that early DJD-related pain would have a significant impact on the QoL of affected cats.
Materials and methods
This blinded, nested case-control study was approved by the University of Bristol’s Health Sciences Faculty Research Ethics Committee (69041; 4 July 2018) and the Animal Welfare and Ethical Review Body (VIN/18/026; 9 August 2018). Owners were recruited from the Bristol Cats (BC) study and the general public between August 2018 and October 2019. Briefly, the BC study is an ongoing longitudinal study of the health, behaviour and environment of client-owned cats, where data are being collected prospectively from owners and veterinary surgeons via the use of questionnaires and the sharing of clinical records, respectively. 21 Owners of eligible BC study cats were contacted directly via phone, post or email. Owners of non-BC study cats were recruited via study advertisements (University of Bristol campus, local veterinary practices) and social media. The inclusion criteria are shown in Table 1.
Inclusion and exclusion criteria

Cats with unrestricted outdoor access were excluded to avoid losing the accelerometers. Restricted outdoor access included being walked on a lead or being allowed in an enclosed area for limited periods. A breakaway collar and habituation instructions were provided at least 2 weeks before the visit for cats not wearing a collar. Cats were allocated to the case or control group according to their mobility score (MS). A total of 12 mobility-related questions were selected from the BC questionnaire (see section E2 of file 1 in the supplementary material) based on changes that were most likely to occur as a result of DJD rather than other disease processes. These questions were used to classify cats as cases or controls, and owners additionally needed to have completed at least 10/12 questions (~80%), answering ‘not applicable’ in less than 50% of those. The answer ‘not applicable’ was not given a score; the remaining answers were 0 = ‘no’, 1 = ‘maybe’ and 2 = ‘yes’. Control cats were required to have no owner-assessed mobility impairment (MS = 0), whereas cats with owner-assessed mobility impairment (MS >1) were assigned to the case group. An MS of 1 corresponded to a ‘maybe’ answer to a single question and was excluded to eliminate uncertain answers to a single aspect of mobility that could also have reflected a different disease process to DJD. Conversely, a score of 2 and above corresponded to one ‘yes’ answer or two ‘maybe’ answers and it was felt that it could reflect early mobility impairment. Eligibility evaluation and MS calculation were performed using the most recently completed BC questionnaire for BC study cats and an online questionnaire containing the same questions about mobility for non-BC study cats.
Participating owners signed a consent form after being fully informed about the study. Owners of eligible cats additionally completed the FMPI and VetMetrica questionnaires online (pre-visit measures). The FMPI questionnaire asked owners to rate their cat’s ability to perform 17 activities compared to a normal cat on an integer scale, with 0 = ‘not at all’ and 4 = ‘normal’. To maintain the scale when questions were unanswered or non-applicable, a calculation of percent was used for analysis, where FMPI% = (sum of answered questions) / (number of questions answered × 4). The VetMetrica questionnaire asked owners to rate how 20 different words described their cat on an integer scale, with 0 = ‘not at all’ and 6 = ‘couldn’t be more’. Using the responses to these questions, a proprietary algorithm generated scores for the Vitality, Comfort and Emotional Wellbeing (EWB) QoL domains. One final question asked owners to rate the cat’s QoL on an integer scale, with 0 = ‘very poor’ and 3 = ‘very good’. The assessor (EM) was blinded to each cat’s MS and other questionnaire results. Participating cats were visited in their own homes, where the assessor recorded the body condition score (BCS) 22 and performed an orthopaedic examination (see file 2 in the supplementary material). Pain responses for each joint were graded, and appendicular joints were evaluated for the presence of crepitus, thickening and effusion using a previously published integer scale. 2 A score was assigned to each cat based on their temperament during the orthopaedic examination. 23 After this, an activity monitor was placed upright on the ventral aspect of each cat’s collar for 2 weeks (Figure 1).

Study participant wearing the collar-mounted activity monitor
The activity monitor used was an Actical Z (Philips Respironics), an omnidirectional activity monitor that has dimensions of 29 mm × 37 mm × 11 mm, weighs 16 g and has a piezoelectric sensor mounted to an internal circuit board. 24 The sensor can measure analogue voltage changes that are generated proportionally to the intensity and duration of change in acceleration. 25 The measurement range of this sensor is 0.05–2 G, and the measurement bandwidth is in the range of 0.035–3.5 Hz. The readings are converted into counts of 100 for the chosen measurement period (epoch) when the accelerometer reading goes above 0.02 G (at a peak of 1 G). Actical Z has a 32 Hz sampling rate and can collect data in epoch lengths in the range of 1 s to 1 min, or in raw collection mode. There were four devices available, all newly purchased and calibrated by the manufacturer at the same time. The epoch length in this study was set to 1 s, with each daily activity profile composed of 86,400 second-by-second measurements. The recording was set to start the following morning (8:00 AM local time) to avoid the confounding effects of the visit and acclimation to wearing the activity monitor. The activity monitor was worn throughout the 2-week study period, after which the researcher would visit the cat again to remove the device. Activity data were downloaded using a designated serial port reader (Actireader) and software (Actical 3.10); this created a graph containing activity counts per day (Figure 2) and imported raw data into an Excel spreadsheet to be used for subsequent analysis. Finally, the owners were asked to keep a diary, recording the times when the device and/or the collar fell off and were replaced (see file 3 in the supplementary material). Accelerometry findings are described separately. 26

Representative graph illustrating activity counts as generated by the activity monitor. The graph shows total activity counts per day (‘Total’) as well as the average hourly activity count (‘Average’) for one of the study’s participants
Data and statistical analysis
Participating cats were assigned a unique identification number. Age was regrouped into biologically relevant life stages that have clinical relevance in terms of the physical and behavioural changes that occur at different time points in cats’ lives, thereby informing veterinary care. 27 These were <7 years (Prime); ⩾7–11 years (Mature); ⩾12–15 years (Senior); ⩾16 years (Geriatric). Categorical variables were collapsed if data were sparse. Temperament assessment scores were collapsed to 0–2 = ‘friendly’ or 3–4 = ‘unfriendly’. 23 Data were collapsed to ‘overweight/obese’ for BCS 6–9 and ‘not overweight’ for BCS 1–5, which included underweight cats (BCS 1–3) and cats of ideal weight (BCS 4–5). A total pain score was created for each cat by summing the total appendicular and axial scores. Total crepitus, thickening and effusion (manipulation scores) were generated for each cat by summing the score for each appendicular joint. Individual pain and manipulation scores were additionally grouped for descriptive statistics into ‘no pain’ and ‘no abnormal signs’ if 0, or ‘pain present’ and ‘abnormal signs present’ if ⩾1, respectively.
Analyses of the questionnaire and visit data were performed using SPSS (version 24.0.0.2; IBM). Data consisted of non-normally distributed variables, and non-parametric statistical tests were used. An alpha value of ⩽0.05 was set for statistical significance in all analyses, and an exact significance (two-tailed) is reported. Group comparisons were performed using a Mann–Whitney or χ2 test if the variables were continuous or categorical, respectively. Fisher’s exact test was used instead of the χ2 test when >20% of cells had expected frequencies of <5. Odds ratio (OR) and Cramér’s V were used as measures of effect size on the results of the χ2 and Fisher’s exact tests, respectively. A post hoc comparison using the Holm–Bonferroni correction was performed to correct for the familywise error rate associated with multiple hypotheses testing. 28 A corrected significance cut-off was calculated for each hypothesis as α/n – rank number of pairs (by the degree of significance) + 1, where n is the number of tests. The null hypothesis (there is no difference between the two groups of cats for the selected variable) was rejected when the P value associated with each hypothesis was lower than the corrected P value calculated using the Holm–Bonferroni correction.
Machine learning of the accelerometer data was undertaken, and the methodology and results are presented separately. 26
Results
A total of 57 cats were included in the study, as shown in the recruitment flow chart (Figure 3).
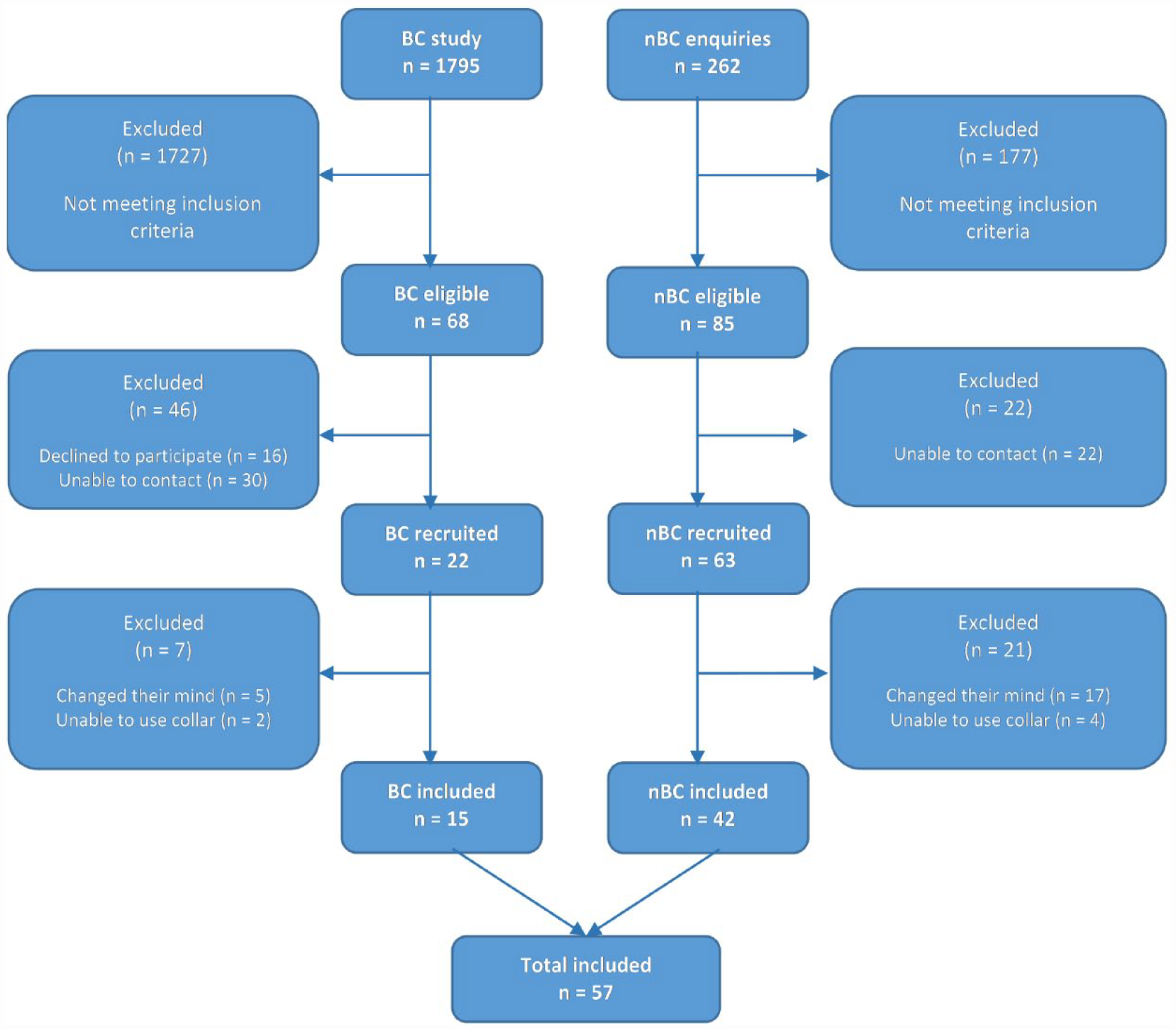
Recruitment and enrolment flow chart. BC = Bristol Cats; nBC = non-Bristol Cats
All cats were neutered, 29/57 (50.9%) were male and 30/57 (52.6%) belonged to the Mature life stage age group. Only 14/57 (24.6%) cats were purebred, with the remaining being domestic shorthair, domestic longhair and crossbreeds. Most cats were considered friendly (49/57, 86.0%) and not overweight (32/57, 56.1%) by the assessor. There were no missing data for the FMPI or VetMetrica questionnaires, and owners perceived their cat’s QoL as ‘very good’ (40/57, 70.2%) or ‘good’ (17/57, 29.8%). The orthopaedic examination was not possible in one cat due to its temperament; therefore, only data from 56 cats were included in the analysis of the orthopaedic examination data. It was also not possible to examine the hip joints of five cats for the same reason. The median and interquartile range (IQR) for pre-visit and visit measures are shown in Table 2.
Pre-visit and visit measures
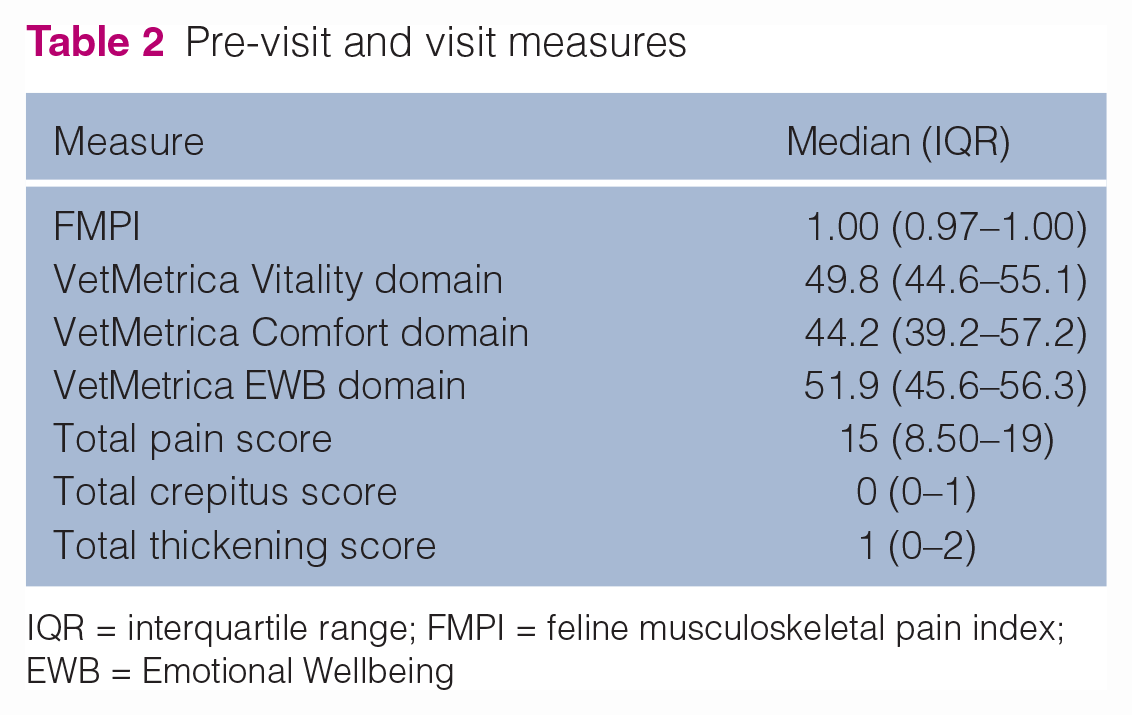
IQR = interquartile range; FMPI = feline musculoskeletal pain index; EWB = Emotional Wellbeing
The prevalence of abnormalities detected during the orthopaedic examination is shown in Table 3. Pain was detected bilaterally in 46/56 (82.1%) cats with a median of 2 (IQR = 1–3) affected joints (Table 4).
Prevalence of abnormalities detected during orthopaedic examination of the appendicular and axial skeleton (n = 56 cats)

Data are presented as n (%)
Prevalence of bilateral pain in each joint type (n = 56 cats)

Data are presented as n (%)
The mobility score range was 0–13 with a median of 3 (IQR = 0–4). All 27 control cats had an MS of 0, and the 30 case cats had a median MS of 4 (IQR = 3.75–6). No significant difference was found between the two groups in terms of their demographics, temperament or BCS (Table 5).
Group comparisons for demographic data, temperament and BCS (n = 57 cats)

Data are presented as n (%)
Corrected significance cut-off values associated with each hypothesis testing are as follows: age in life stages = 0.01; sex = 0.0125; breed category = 0.05; vet-assessed temperament = 0.0167; vet-assessed BCS = 0.025
BCS = body condition score; FET = Fisher’s exact test; OR = odds ratio
There was a significant difference and a moderate effect size when comparing FMPI scores (P = 0.003) and VetMetrica scores for the Comfort domain (P = 0.002). Case cats scored lower than control cats in both the FMPI and VetMetrica Comfort domain, which signified a higher degree of impaired mobility and QoL related to comfort, respectively. No statistical difference was detected for the Vitality and EWB domain scores. Owner perception of QoL was not statistically analysed as 2/4 of categories (‘very poor’ and ‘poor’) had no data. Case cats scored significantly higher than control cats for total pain (P <0.0001), crepitus (P = 0.002) and thickening (P = 0.003). The observed effect size was large for total pain scores and moderate for total crepitus and thickening scores. Group comparisons for pre-visit and visit measures are shown in Table 6.
Group comparisons for pre-visit (n = 57 cats) and visit (n = 56 cats) measures

Data are presented as median (IQR)
Corrected significance cut-off values associated with each hypothesis testing are as follows: FMPI = 0.005; Vitality = 0.0071; Comfort = 0.0042; EWB = 0.0083; total pain = 0.0036; total crepitus = 0.0045; total thickening = 0.0056
Statistically significant
EWB = Emotional Wellbeing; FMPI = Feline Musculoskeletal Pain Index; IQR = interquartile range
Case cats were 14 times more likely (P = 0.005) to have bilateral pain detected on orthopaedic examination than control cats. There was also a significant difference (P = 0.001) and a moderate effect size when comparing the number of joints affected with bilateral pain between the two groups, with case cats having more affected joints than control cats (Table 7). Analysis of the accelerometry data identified differences between the activity of the case and control cats.26
Group comparisons for the prevalence of bilateral pain and the number of affected joints (n = 56 cats)

Data are presented as n (%)
Corrected significance cut-off values associated with each hypothesis testing are as follows: bilateral pain = 0.0063; number of affected joints = 0.0038. Analysis of the accelerometry data identified differences between the activity of the case and control cats 26
Statistically significant
FET = Fisher’s exact test; OR = odds ratio; IQR = interquartile range
Discussion
This study demonstrated that early DJD-related changes in owner-reported mobility reflect changes in joint health as evaluated by the FMPI and orthopaedic examination. The study also confirmed the initial hypothesis that early DJD-related pain has a significant impact on the QoL of affected cats. The activity profiles of cats with DJD have previously been assessed using both subjective and objective tools; however, these cats had well-established DJD that had been confirmed using different imaging modalities.10,14,29 This is the first study where the activity profiles of cats with early DJD-related changes in owner-reported mobility were compared to healthy cats using prospectively collected data from subjective owner assessment questionnaires (FMPI, VetMetrica), orthopaedic examination and accelerometry.
The ability of the FMPI to confidently differentiate between healthy cats and cats with both clinically and radiographically confirmed DJD has previously been established. 11 Nevertheless, this is the first time that it has been shown to successfully discriminate between cats with and without early owner-reported mobility changes, as evidenced by the significantly lower FMPI scores of case cats compared to control cats. This further validates the FMPI as a clinical tool that can be used for the timely diagnosis of DJD.
The significantly lower scores of case cats compared to control cats in the Comfort VetMetrica domain suggested that even the lower levels of DJD-related pain experienced by cats with early DJD significantly impact all the physical aspects of their QoL. One possible explanation for the lack of a statistically detected difference between groups for the Vitality and EWB domain scores could be that owners have difficulty distinguishing early DJD-related changes affecting the mental and emotional aspects of their cats’ QoL. This is the first time that this instrument has been used in a population with early signs of DJD-related pain and no comorbidities; however, this study’s findings suggest that further refinement of the scoring algorithm may be indicated, especially concerning items loading to more than one domain.
Although cats with higher pain scores were shown to have an unfriendly temperament in previous studies,30,31 no significant difference was detected between the temperament of the case and control cats in this study. A likely explanation could be that the cats in those studies had well-established DJD rather than early signs of DJD-related pain, as was the case with the cats of the present study.
The significant differences detected between the groups for all orthopaedic examination findings demonstrate that orthopaedic examination can clinically differentiate between cats with and without early DJD-related changes in owner-reported mobility and altered activity patterns. Case cats had significantly higher pain and manipulation scores than control cats, were more likely to suffer from bilateral pain and had more joints affected with bilaterally detected pain. The latter findings confirm the previous belief that bilateral disease is a core component of feline DJD. It should, however, be noted that, whereas previous studies estimated the prevalence of bilateral DJD based on radiographic and/or orthopaedic examination findings,2,3,7,32–34 the higher prevalence detected in this study was a direct reflection of bilateral pain detected exclusively during the orthopaedic examination.
One of the limitations of this study’s design was that its subjective outcome measures depended on questionnaires and thus owner-reported data, which could have introduced response, measurement and reporting bias. Reporting bias could have been partially mitigated if veterinary records had been checked for exclusion criteria that had not been reported by owners; however, this was not possible within the study’s time frame. Every effort was made to minimise interviewer bias by blinding the assessor to each cat’s case or control status and demographic data until data analysis began. This bias could be addressed in future studies by having two veterinary surgeons perform the orthopaedic examination, providing they follow a standardised protocol to minimise inter-observer variability.
The study’s population was similar to the UK population attending primary-care veterinary practices except for the proportion of purebred cats (~25% in this study vs 11%). 35 Owners of pedigree cats are considered more motivated than the general UK population 36 and, as they completed several questionnaires and allowed the assessor to examine their cats within their own homes, this study’s owners were possibly more motivated than owners attending primary-care veterinary practices. There was no significant difference between the case and control groups concerning their demographic characteristics. Most owners were able to provide an estimate rather than an accurate age; therefore, the decision to use life stages was made to allow for age estimates while having a holistic clinical basis. 27
Conclusions
Being able to recognise signs of mobility impairment earlier would allow interventions aimed at slowing the progression of DJD, thereby improving the QoL of affected cats. Both the FMPI and orthopaedic examination agreed with owner-reported information, illustrating that they can be used in the consulting room to confidently differentiate cats with early signs of DJD-related pain from healthy cats.
Supplemental Material
File 1
Bristol cat questionnaire for 6-year-old cats
Supplemental Material
File 2
Orthopaedic examination sheet
Supplemental Material
File 3
Accelerometer diary
Footnotes
Acknowledgements
The authors would like to thank all owners and their cats for participating in this study as well as the BC study team for assisting with recruitment. Many thanks go to Axel Montout, Dr Tilo Burghardt, Dr Ranjeet Bhamber and Professor Andrew Dowsey for their invaluable help with the analysis of the accelerometer data. The authors would also like to acknowledge NewMetrica for allowing the use of their tool VetMetrica, free of charge.
Author note
This paper was presented in part at the 2020 ISFM European Feline Congress.
Supplementary material
The following files are available online:
File 1: Bristol cat questionnaire for 6-year-old cats.
File 2: Orthopaedic examination sheet.
File 3: Accelerometer diary.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by Zoetis as part of EM’s Feline Scholar role. The BC study is funded by Cats Protection and Waltham Petcare Science Institute.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (`best practice’) of veterinary clinical care for the individual patient were always followed. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals) for all procedure(s) undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.