
Abstract
Objectives
The aims of the study were to investigate if feline middle ear anatomy can be visualized using endoscopy via a lateral bulla approach and to determine if scope-assistance increases rates of successful entry into the hypotympanum during feline total ear canal ablation and lateral bulla osteotomy (TECA-LBO).
Methods
A total of 13 feline cadaver heads underwent CT to confirm the absence of pre-existing middle ear disease. For each head, an electronic coin toss was used to determine which ear would undergo endoscope-assisted TECA-LBO; a traditional TECA-LBO without the use of the scope was performed on the contralateral side. In endoscope-assisted procedures, a 1.9 mm scope was intermittently inserted into the tympanic bulla via a lateral bulla approach and used to identify middle ear structures, visualize the bony septum and confirm entry into the hypotympanum. After the bilateral TECA-LBO, the cadaver heads were imaged again and assessed for evidence of entry through the septum.
Results
Soft tissue and osseus structures of the middle ear were readily visualized with a 1.9 mm scope. Success rates for entry into the hypotympanum were high between both endoscope-assisted and traditional procedures, with entry confirmed for 12/13 ears in each group.
Conclusions and relevance
Endoscope assistance can facilitate the identification and examination of middle ear structures but does not appear to increase the success rate of entry into the hypotympanum during feline TECA-LBO, as entry through the bony septum was consistently accomplished even without scope-assisted visualization. Alternative benefits to scope assistance may exist, and future studies to elucidate its impact on rates of intraoperative trauma to middle ear structures are indicated.
Introduction
Total ear canal ablation and lateral bulla osteotomy (TECA-LBO) is commonly performed in both dogs and cats and involves complete resection of the external ear canal and ablation of the epithelial lining of the tympanic bulla. While it is typically performed to treat septic otitis media in dogs, in cats, both neoplasia and inflammatory disease are the leading causes for TECA-LBO.1 –3 Significant differences exist in the structural anatomy of the middle ear between these species; namely, the presence of an incomplete bony septum within the feline tympanic bulla that divides it into a smaller dorsolateral component, composed of the epitympanum and mesotympanum, and a larger ventromedial hypotympanum.4,5 In combination with the relatively deep tympanic chamber of the cat, this septum can impede complete penetration into the deeper portion of the tympanic bulla, limiting the surgeon’s ability to fully ablate the epithelium of the bulla. In fact, previous research has shown that even experienced surgeons may fail to completely enter the hypotympanum through the septum up to 25% of the time during feline TECA-LBO procedures. 6
One strategy for increasing success in entering the hypotympanum may involve more direct visualization of the structures of the middle ear than is achievable with current surgical approaches. In human otolaryngology, endoscopy has gained popularity in the diagnostic assessment of the middle ear, as well as visualization during surgery, and is acknowledged as an effective means of identifying ear anatomy and adequately illuminating the middle ear during surgical procedures.7,8 A recent veterinary study has illustrated that an endoscope can be used to effectively identify the structures of the canine middle ear after lateral and ventral bulla osteotomy, 9 but so far, no attempts have been documented to assess endoscopic evaluation of middle ear structures in cats. In addition, there is no existing literature evaluating the use of scope assistance for increasing effective hypotympanum entry during feline TECA-LBO.
The aims of the present study were to investigate whether the unique anatomy of the feline middle ear can be adequately visualized using endoscopy via a lateral bulla approach and to determine if endoscopy is helpful in ensuring appropriate entry into the hypotympanum during feline TECA-LBO. We hypothesized that the ease of successful visualization of middle ear structures would be comparable to that in dogs, and that direct endoscopic visualization of the septum during surgery would facilitate higher rates of successful bony septum penetration than previously reported.
Materials and methods
A total of 13 feline heads from cadavers of unowned animals (Skulls Unlimited International) were acquired for use in this study. For Skulls Unlimited’s ethical sourcing policy, please see file 1 in the supplementaty material. Before use, each head was imaged via a GE 64-slice LightSpeed VCT scanner run in helical fashion, with images acquired at 1.0 mm and reconstructed into axial sequences at 1.25 mm. The scans were evaluated by a board-certified veterinary radiologist and assessed for any evidence of osseous changes consistent with pre-existing middle ear disease.
The TECA-LBO procedure 10 was performed bilaterally on all cadavers, with the external canal amputation performed by either a surgical intern or a board-certified small animal veterinary surgeon; the bulla osteotomies and ear canal ablations were performed exclusively by the boarded surgeon. For each cadaver, the laterality of the traditional TECA-LBO was assigned randomly via an electronic coin flip. The contralateral TECA-LBO was performed with the assistance of a 1.9 mm 30° arthroscope attached to a 4k camera system (Synergy UHD4 Imaging Platform; Arthrex) inserted intermittently into the middle ear via the lateral bulla osteotomy site to facilitate visualization of the middle ear structures and assessment of the integrity of the incomplete bony septum until entry into the hypotympanum was observed. Images of the tympanic bulla and the bony septum were captured before and after entry into the hypotympanum for all ears where endoscope assistance was utilized.
After the TECA-LBO procedures, postoperative CT images were acquired as previously described. The tympanic bullae were assessed by the board-certified radiologist and radiographic evidence of entry through the bony septum (yes/no) was recorded for each ear. Using the results of this assessment, a frequency table was created to compare the percentage of successful procedures (defined as those with CT evidence of entry into the hypotympanum) between the endoscope-assisted and traditional-approach TECA-LBO treatment groups. A second frequency table assessing the effect of laterality (left vs right ear) on success of the procedure by treatment group was also generated.
The magnitude of the effect of endoscope assistance was determined via computation of odds ratios for both treatment groups across both ears, for the left ear only, and for the right ear only. Statistical significance was assessed using Fisher’s exact test for the resulting data, and a P value <0.05 was considered significant. A Mantel–Haenszel procedure was performed to control for procedure laterality, along with an exact logistic regression that incorporated fixed effects for both the laterality and treatment groups.
Results
Based on their dentition, all cadavers appeared to be from adult felines; the remainder of each cadaver was not available so exact age, full body weight and sex of the cats could not be determined. None of the cadaver heads exhibited any evidence of osseous pathology related to middle ear disease on initial CT imaging.
Use of the endoscope during surgery did not require an additional approach or enlargement of the lateral bulla osteotomy relative to the traditional approach. The middle ear was readily observed and both osseous landmarks and neurovascular structures were able to be recognized and imaged with acceptable clarity. These structures included the malleus, incus and stapes, the chorda tympani, the external acoustic meatus, the pars flaccida and pars tensa of the tympanic membrane, the promontory, and the cochlear and vestibular windows. The bony septum was identified consistently and without difficulty in each cadaver, and entry into the hypotympanum was easily observed and documented. Representative images from the middle ear are shown in Figure 1.

Images captured during endoscopic evaluation of the middle ear of feline cadavers. (a) View of the tympanic membrane before entry into the middle ear. (b) View from inside of the middle ear after penetration through the tympanic membrane. (c) View of the intact bony septum. (d) View of the bony septum after entry through the septum into the hypotympanum. (e) View of the middle ear bones. D = dorsal; V = ventral; R = rostral; Ca = caudal; CT = chorda tympani; CW = cochlear window; EAM = external acoustic meatus; I = incus; MM = manubrium of the malleus; P = promontory; S = stapes; TM = tympanic membrane
A total of 13 endoscope-assisted TECA-LBO procedures and 13 traditional-approach TECA-LBO procedures were performed. In each treatment group, 12/13 procedures resulted in entry in the hypotympanum (Figure 2). Both unsuccessful procedures were performed in the right ear. Without laterality considered, the odds of successful entry into the hypotympanum during an endoscope-assisted procedure were 1.0 (95% confidence interval [CI] 0.1–17.9) times the odds of successful entry during a traditional-approach procedure (P = 1.0) (Table 1). An odds ratio could not be calculated for left-sided procedures owing to all procedures being successful on that side, regardless of treatment group. For right-sided TECA-LBO procedures, the odds of successful hypotympanum entry were 1.2 (95% CI 0.1–24.5) times greater with endoscope assistance (P = 1.0) (Table 2). When adjusting for laterality, the Mantel–Haenzel odds ratio for association between hypotympanum entry and treatment group was 1.2 (95% CI 0.1–24.5), indicating no confounding effect of laterality (P = 0.455). The odds ratio for successful entry into the hypotympanum with left-sided procedures (regardless of treatment group) compared with right-sided procedures was 2.4; univariable analysis revealed a lack of significance of laterality with regard to the success of the procedure (P = 0.48).
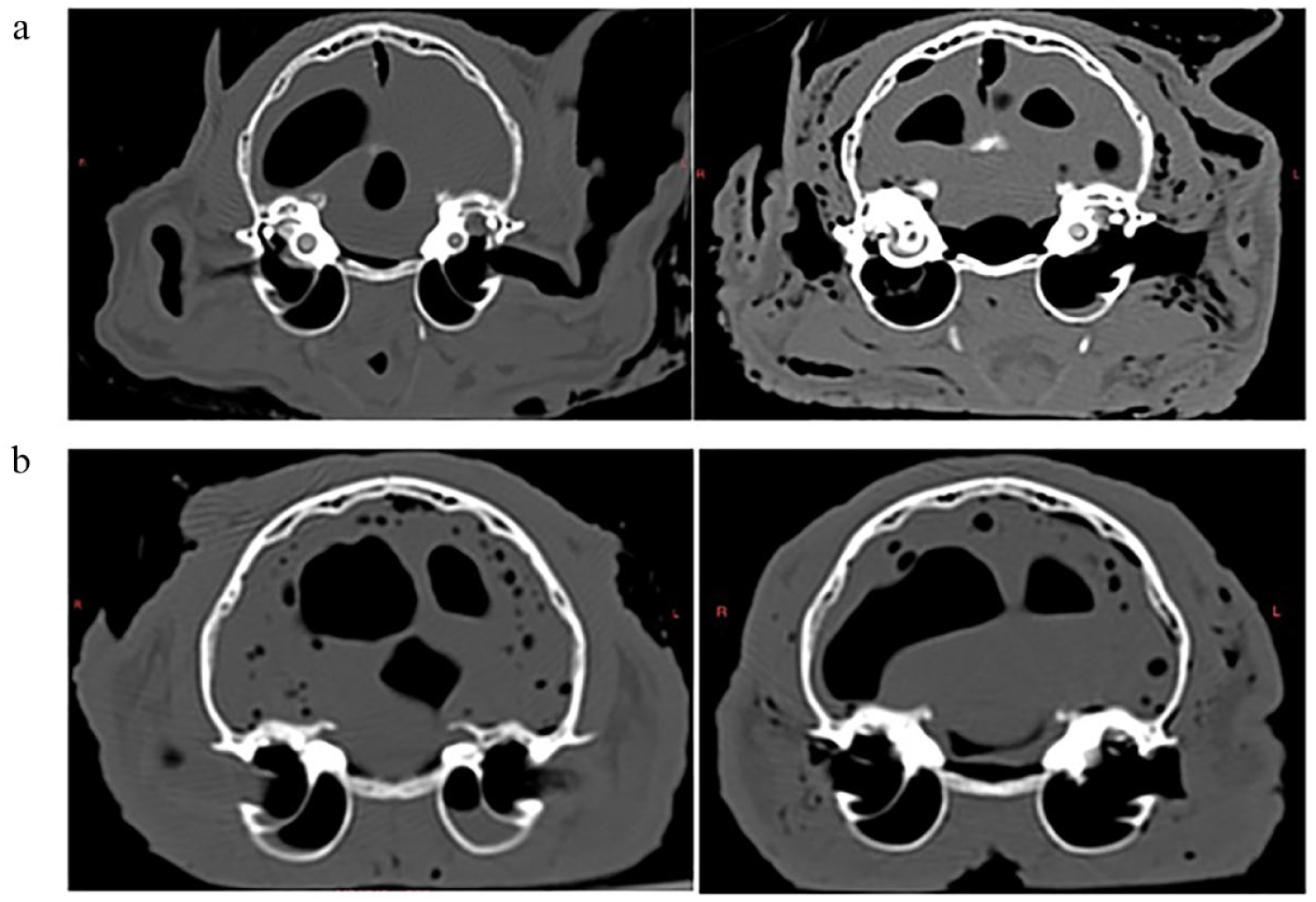
CT images from cadaver heads before and after the total ear canal ablation and lateral bulla osteotomy (TECA-LBO) procedure. (a) Cadaver 1 with intact septa before TECA-LBO (left) and bilaterally perforated septa postoperatively (right). (b) Cadaver 11 with intact septa before TECA-LBO (left) and perforated left septum after bilateral procedure (right)
Frequency table of procedural outcomes for both traditional-approach and endoscope-assisted total ear canal ablation and lateral bulla osteotomy in feline cadavers

Fisher’s exact test
Frequency table of procedural outcomes for both traditional-approach and endoscope-assisted total ear canal ablation and lateral bulla osteotomy with regard to procedure laterality

Odds ratio (OR) could not be calculated
Fisher’s exact test
Discussion
In the feline cadavers studied, the addition of an endoscope to the traditional TECA-LBO approach was observed to be technically simple and was able to be facilitated through the lateral bulla osteotomy site without the need for an additional or expanded approach. A previous study in canine cadavers resulted in the successful visualization of 14 notable structures of the middle ear via lateral endoscopic visualization using a 2.7 mm 30° scope; 9 in the current study, only 12 structures were able to be directly observed via this approach. Structures unable to be identified in the cat compared with the dog included tympanic bone spicules and the tympanic plexus. Tympanic bone spicules are an inconsistent anatomic feature in cats, 11 so may not have been present in any of the ears evaluated endoscopically. Another potential cause for the decreased number of visible structures compared with those seen in dogs is the relatively smaller volume of the feline middle ear, as well as the decreased diameter of the bulla osteotomy site in smaller patients. As a result of these size limitations, endoscopic evaluation of the middle ear of the feline cadavers was restricted to a 1.9 mm scope; the smaller scope has an inherently narrower image width than the 2.7 mm scope, resulting in a more constrained field of vision. In addition, the cadavers included in this study were utilized in several unrelated studies and had undergone multiple freeze–thaw cycles before the TECA-LBO procedure, resulting in a compromise of the soft tissue structures and a subsequent diminished ability to accurately identify these structures, including the tympanic plexus, during endoscopic evaluation.
Despite these limitations, multiple important structures of the tympanic chamber were still able to be consistently identified with scope assistance. These included neurovascular structures, such as the chorda tympani, osseous landmarks, such as the bony promontory, and the incomplete bony septum separating the mesotympanum from the hypotympanum. Rates of neurologic complications during the feline TECA-LBO procedure are particularly high compared with those in dogs,12,13 with 42% of patients experiencing postoperative Horner’s syndrome and 58% of patients experiencing postoperative facial nerve paralysis in one study. 3 It has been hypothesized that the prevalence of Horner’s syndrome in particular may be largely due to the greater exposure of the tympanic plexus and post-ganglionic parasympathetic fibers in the feline middle ear that makes these structures more susceptible to iatrogenic damage during aural surgery. The bony promontory is the primary location of the tympanic plexus; 14 therefore, visualization of this structure can allow for greater protection of the plexus during surgery, even if the plexus itself is not directly observed and may result in less neurologic trauma.
A primary hypothesis of this study was that direct visualization of the bony septum would result in improved success in fully penetrating the septum to gain access to the hypotympanum. In the feline cadaver surgeries, the use of the endoscope to directly visualize the bony septum at the time of surgery did not result in any significant increase in rates of successful entry into the hypotympanum. However, it is important to note that success rates for penetration through the bony septum were very high in general and notably higher than previously reported success rates. 6 There was also no significant effect of laterality on the success of the procedure, indicating that no additional benefit was derived from the scope, even in procedures performed on the surgeon’s non-dominant side. Access to the hypotympanum is essential for full debridement of the epithelial lining of the tympanic bulla, and in dogs undergoing TECA-LBO for chronic otitis, incomplete ablation of this epithelium poses a risk of continued or recurrent infection of the middle ear, abscessation at the surgery site and formation of acquired cholesteatomas.15,16 In cats, the procedure is less likely to be performed for otitis and more likely to be performed for neoplastic or inflammatory disease, and as a result, the utility of full epithelial debridement is less clear. 6 However, previous studies in feline patients have shown that cats with neoplastic or polypoid disease can have secondary low-grade bacterial otitis associated with their disease and can have persistent aural secretions after removal of these growths.13,17,18 Previous reports of feline cholesteatoma 19 also suggest that development of the acquired form of this disease may be possible in cats undergoing TECA-LBO without complete epithelial debridement. Most ear canal tumors in cats are malignant and recurrence is possible with incomplete excision, 20 and aural polyps are also prone to regrowth, especially in the presence of continued inflammation or infection; 21 in both of these situations, full epithelial ablation may be important for removing all traces of disease intraoperatively. In addition, in those feline patients that do present for primary otitis media, up to 94% may have both middle ear chambers affected, 22 making full epithelial ablation as essential in these cats as in their canine counterparts.
While the frequency in which entry into the hypotympanum was achieved in this study is encouraging and implies that access to this chamber can be reasonably accomplished even without scope-assistance, penetration into the hypotympanic chamber does not guarantee effective epithelial ablation. The condition of the soft tissues in the cadavers studied was not conducive to evaluating the epithelial lining of the bulla, and an examination of whether ablation was more effective with or without endoscope-assistance is beyond the scope of this study. However, this may be a worthwhile avenue for future investigation. In addition, other effects on the soft tissue structures were likewise unable to be determined. Human studies have shown that introduction of an endoscope into the relatively small, confined and avascular middle ear results in a rapid increase in the temperature within the bulla by up to 10°C. 7 This raises concerns for possible thermal damage to the structures within the middle ear in living patients, particularly the cochlear and neurovascular structures. The impact of this thermal damage could potentially negate any possible benefits derived from being able to visualize the neurologic structures of the ear, and further studies to better elucidate the potential benefits and complications of endoscopic evaluation of the middle ear in veterinary patients are indicated.
This study was limited by an overall small sample size, which may cause a type II error and obscure significant differences in outcomes with and without the use of an endoscope during the TECA-LBO procedure. In addition, the subjects of this study were decapitated cadaver heads; owing to the lack of the remainder of the cadaver body, surgical positioning was not fully analogous to that which would be exhibited in a live patient. Positioning for the postoperative CT scan was similarly challenging, and recreation of the positioning used for the preoperative imaging could not be perfectly achieved. The difficulties experienced during imaging may have slightly skewed the results of this study, as the cadaver ear that underwent an endoscope-assisted procedure and did not have evidence of entry through the septum on postoperative CT had intraoperative images that clearly showed that a hole had been created in the septum into the hypotympanum. This calls into question the acuity with which CT can determine whether a defect has been created in the thin bone of the septum. The conflict between intraoperative and postoperative findings in this cadaver suggests that there is a possibility of missing septum penetration even with advanced imaging, which may explain why the previous study resulted in lower rates of hypotympanum entry than would be expected. 6
Conclusions
Endoscopic evaluation of the feline middle ear is easily accomplished during the TECA-LBO procedure and allows for visualization of key osseous and neurologic structures. While endoscope assistance did not have any effect on the success rate of entry into the hypotympanum during the procedure, alternative benefits with regards to epithelial ablation and reduced iatrogenic trauma to middle ear structures may exist. Further work to better assess these proposed advantages will be helpful in identifying indications for the use of endoscopy during middle ear surgery in live patients.
Supplemental Material
Supplemental Material
Skulls Unlimited ethical sourcing policy
Footnotes
Acknowledgements
The authors thank Dr Natalia Cernicchiaro for the statistics performed in this study.
Author note
This research was presented as an abstract at the 2022 Society of Veterinary Soft Tissue Surgery (SVSTS) conference in New Orleans, Louisiana, USA.
Supplementary material The following file is available as supplementary material: Skulls Unlimited ethical sourcing policy.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non- experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.