
Abstract
Objectives
The study hypotheses were as follows: (1) owing to the unique anatomy of the feline middle ear, the hypotympanum would be entered in less than 100% of cats during total ear canal ablation and lateral bulla osteotomies (TECA-LBOs); and (2) incomplete penetration of the septum and subsequent failure to enter the hypotympanum is more likely to occur in surgeries performed by a novice surgeon when compared with an experienced surgeon and may be under-recognized.
Methods
Head CT was performed in 12 feline cadavers to confirm absence of gross ear disease. A novice surgeon and an experienced surgeon were randomly assigned to perform TECA-LBO on the left or right ear. Surgeons were blinded to each other’s surgical technique. CT of cadavers was performed after the procedure. Successful penetration of the septum, entry into the hypotympanic cavity and amount of bone removed in bulla osteotomy, quantified via CT, were compared between the novice surgeon and experienced surgeon.
Results
The novice surgeon entered the hypotympanum in 3/12 (25%) procedures, compared with 9/12 (75%) procedures performed by the experienced surgeon. The experienced surgeon performed a larger osteotomy than the novice surgeon (3301 mm vs 1376 mm, P <0.0023). Regardless of surgeon experience, more bone was removed in surgeries in which the hypotympanum was entered.
Conclusions and relevance
Our results underscore the need for familiarity with feline middle ear anatomy when performing TECA-LBOs. Postoperative CT is recommended for novice surgeons to confirm entry into the hypotympanum.
Introduction
Total ear canal ablation and lateral bulla osteotomy (TECA-LBO) is a procedure involving the complete excision of the horizontal and vertical ear canal, external acoustic meatus and partial osteotomy of the tympanic bulla to gain access to remove the epithelial lining of the tympanic cavity. 1 While ventral bulla osteotomies are commonly performed in cats as treatment for disease isolated to the middle ear (primarily inflammatory polyps), TECA-LBO is the surgical treatment of choice for external ear canal neoplasia, severe inflammatory conditions and end-stage otitis externa as well as aural trauma and para-aural abscessation.2,3 Complete removal of all debris and the epithelial lining from the external auditory meatus and tympanic cavity is necessary to reduce the risk of persistent infection and recurrent neoplasia postoperatively.4,5 In dogs, deep infection and cellulitis has been reported in 2–54% of cases postoperatively.2,6–9 In the light of these complications, larger osteotomies have been advocated by some surgeons to improve visualization and ensure complete curettage. 1
The unique anatomy of the middle ear of the cat makes the TECA-LBO surgery challenging. The feline tympanic bulla is divided into an epitympanum and hypotympanum by a complete bony septum, which is not present in the dog. 10 This osseous septum must be disrupted for thorough curettage of the epithelial lining of the hypotympanum during TECA-LBO in cats. 10 Information regarding procedural methodology of feline TECA-LBOs is sparse, with few studies reported in the literature or referenced in veterinary textbooks.10,11
The aim of this study was to assess the frequency of hypotympanum entry during feline TECA-LBOs as well as identifying any effect of surgeon experience level on hypotympanum entry and quantity of bone removal. The hypotheses for this study were as follows: (1) the hypotympanum would be entered in less than 100% of TECA-LBOs due to the presence of a bony septum in cats; and (2) novice surgeons would be less likely to penetrate the septum and thus less likely to access the hypotympanum compared with experienced surgeons.
Materials and methods
Twelve feline cadavers, with no known history of ear disease and which were unowned animals euthanized for reasons unrelated to the study, were used for the present study. Institutional Animal Care and Use Committee approval is not necessary at our institution when working with cadavers. Cadavers were assigned a nine-digit code using a random number generator. 12 Each cadaver’s weight, sex and estimated age based on dentition (juvenile/adult) were recorded.
CT images of the skull were obtained using a 64 detector helical CT scanner (Toshiba Aquilion 64; Toshiba America Medical Systems). Images were collected as a volume with 0.5 mm voxels, 0.5–0.6 s rotation speed, 0.5–0.6 helical pitch, 120 kVp and 200–350 mA. The 0.5 mm volume data were reconstructed in bone and soft tissue algorithms and in transverse, sagittal and dorsal planes at 1 mm slice thickness. CT scans were evaluated and an absence of osseous trauma and signs of ear disease were required for enrollment in the study.
A novice surgeon with no prior experience performing the TECA-LBO procedure and a board-certified small animal veterinary surgeon were randomly assigned to perform TECA-LBO on either the left or right ear of each of the 12 feline cadavers using an electronic coin toss. 12 The novice surgeon studied the procedure using a veterinary surgical textbook, 13 performed one cadaveric surgery under the supervision of the experienced surgeon and assisted in one clinical procedure prior to commencement of cadaveric procedures. Surgeons did not evaluate each other’s surgeries and were not blinded to the aims of the study. TECA-LBO was performed as previously described. 13 Specifically, a Love–Kerrison rongeur (Sontech Instruments) with a 3 mm foot plate was used to perform the LBO. Surgical time was recorded in minutes. During dissection, care was taken to preserve the facial nerve and retroauricular vein to mimic clinical conditions. If the facial nerve was identified during dissection, its condition (intact vs severed) was recorded. All postoperative imaging data were pooled and evaluated at the same time, after the conclusion of all procedures.
Postoperative CT images were obtained as described for the preoperative image acquisition. After the completion of all surgical procedures, CT images were evaluated in transverse, sagittal and dorsal planes by both the novice surgeon and experienced surgeon and a board-certified radiologist. All three observers were blinded to surgeon ear assignment. The tympanic bulla was measured on anatomically matched CT images before and after surgery to measure the length of bone removed using a web-based image viewer (NovaRad, version 8.7.11 NovaRad Corporation) (Figure 1). Entry into the hypotympanum (yes/no) was recorded for each ear. The distance between the ventral extent of the external acoustic meatus and the hypotympanic cavity at the point where the septum attaches to the bulla was measured in each skull. Additionally, the height of the external acoustic meatus was measured on the transverse slice at the point where the external acoustic meatus was longest in the dorsoventral direction (Figure 2). This measurement was used to provide an intraoperative scale for surgical planning and to serve as a baseline to better assess the amount of bone removed relative to the location of the hypotympanum. To gain a more global impression of osteotomy size, the sum of all projections’ differences in pre- and postoperative measurements were compared between the experienced surgeon and novice surgeon.

Representative postoperative CT findings of a feline cadaver after bilateral total ear canal ablation and lateral bulla osteotomy, with the right (R) ear performed by an experienced surgeon and the left (L) ear performed by a novice surgeon. Anatomically paired (a) dorsal, (b) transverse and (c) sagittal slices demonstrate penetrance of the osseous septum on the right ear. Images of the left ear demonstrate incomplete penetrance of the osseous septum with a minimal osteotomy. The white bar is a 1 cm marker

Representative transverse CT image of the left tympanic bulla in a presurgical feline cadaver. An image analysis program (NovaRad) was used to draw a non-linear measurement from the external acoustic meatus to the hypotympanum along the lateral side of the bulla wall (blue line). The mean distance from the most ventral aspect of the external acoustic meatus to the hypotympanum is 10 mm. Mean height of the external acoustic meatus of all cadaver skulls was found to be 5 mm (red line). The white line is a 10 mm marker
Data were analyzed for normality using the Shapiro–Wilk test. Continuous variables that were normally distributed were described using mean ± SD and means were compared using a paired t-test. Non-normally distributed variables were described using median and range and Wilcoxon matched pairs signed rank or Mann–Whitney tests were performed to compare matched samples. To determine if the length removed depended on the surgeon or the image evaluator, a randomized complete block split plot ANOVA with cats as random blocks, surgeon as whole plot fixed effect and image evaluators as split plot fixed effect was carried out using SAS Proc Mixed (SAS/Stat version 14.4). To test the difference in lengths of bone removed, a logarithmic transformation was used to satisfy the assumptions of the ANOVA. A natural log (for transverse data) or natural log (response + 1) (for sagittal and dorsal data) transform of the response variable length was used. The natural log (response + 1) was used for the sagittal and dorsal positions due to some lengths being equal to zero. On back transforming to the original scale, a ratio was created of experienced to novice surgeon length of bone removed. Significance was set at P <0.05.
Results
All 12 cats were characterized as adults based on the absence of deciduous teeth. Five were female (sexual status unknown) and seven were castrated males. Mean body weight was 3.1 ± 1.1 kg. No cadavers were found to have signs of middle ear disease based on CT scan. During dissection, the facial nerve was identified in every procedure by both surgeons and none were transected during dissection in any procedure. The mean distance from the ventral-most aspect of the external acoustic meatus to the hypotympanum was 10 ± 0.9 mm. The mean diameter of the external acoustic meatus was 5 ± 0.7 mm (Figure 2).
The novice surgeon penetrated the osseous septum in 3/12 procedures (25%), with a mean surgical time of 43 ± 9.6 mins (Table 1). The experienced surgeon entered the hypotympanum in significantly more procedures (P <0.03) (75%) and had a significantly decreased mean surgical time of 25 ± 5.2 mins (P <0.001) (Figure 3; Table 1).
Summarized tympanic bulla bone removed by a novice surgeon and an experienced surgeon, surgical time and septum penetration for each cat


Surgical time over successive procedures for experienced surgeon vs novice surgeon. Mean surgical time for the experienced surgeon was significantly lower 25 ± 5.2 mins compared with the novice surgeon who had a mean surgical time of 43 ± 9.6 mins (P <0.03). For the surgeon, the surgical time begins to plateau at the eighth procedure, while it plateaus earlier for the experienced surgeon, around the fourth procedure
When evaluating the bone removal data, the person evaluating the images (novice surgeon, experienced surgeon or radiologist) had no statistically significant effect on the amount of bone removed in any plane (transverse, sagittal and dorsal F statistic [df = 2, 44] 1.29, 1.16 and 2.03, respectively; P value = 0.28, 0.32 and 0.14, respectively) nor which surgeon performed the surgeries (transverse, sagittal and dorsal F statistic [df = 2, 44] 0.21, 2.25 and 0.64, respectively; P value = 0.81, 0.11 and 0.53, respectively). This indicates that image evaluators (novice surgeon, experienced surgeon or radiologist) had no effect on the measurement of how much bone was removed and was consistent between evaluators.
The experienced surgeon removed significantly more bone based on sagittal and dorsal CT projections (F statistic [df 1, 22] 8.57 and 4.42, respectively; P value = 0.008 and 0.047, respectively). This difference was not significant in the transverse plane (F statistic [df 1, 22] = 2.56; P value = 0.124) (Table 2). When combining the mean sum of bone removed on each sagittal, dorsal and transverse CT, significantly larger osteotomies were performed by the experienced surgeon (3301 mm) than the novice surgeon (1376 mm) (P <0.0023). Regardless of surgeon experience, significantly more bone was removed in surgeries in which the septum was penetrated and the hypotympanum was entered (P <0.03).
Ratio of length of bone removed by experienced to novice surgeon
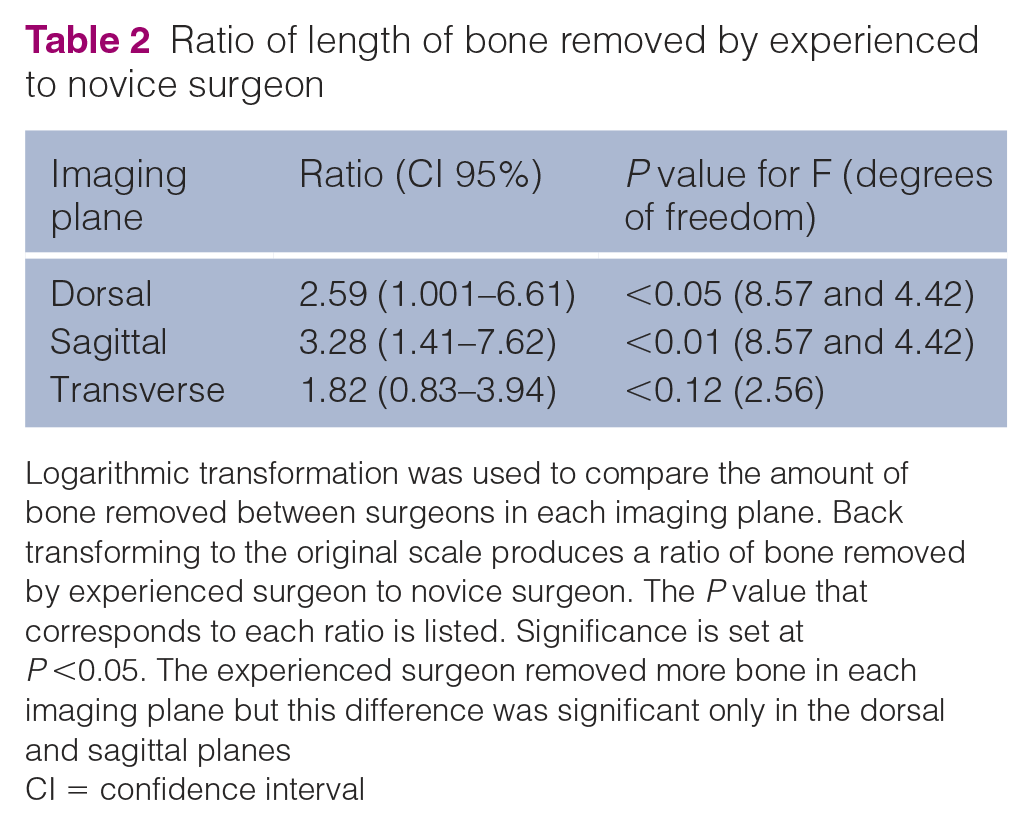
Logarithmic transformation was used to compare the amount of bone removed between surgeons in each imaging plane. Back transforming to the original scale produces a ratio of bone removed by experienced surgeon to novice surgeon. The P value that corresponds to each ratio is listed. Significance is set at P <0.05. The experienced surgeon removed more bone in each imaging plane but this difference was significant only in the dorsal and sagittal planes
CI = confidence interval
Discussion
Our results indicate that the septum was penetrated, and thus the hypotympanum accessed, in less than 100% of procedures and therefore we accept our first hypothesis. The novice surgeon was more likely to make smaller osteotomies and failed to enter the hypotympanic cavity in 75% of procedures. Based on these results, we also accept the second hypothesis that increased surgeon experience leads to more consistent septum penetration and more bone removal.
Ventral bulla osteotomies are performed more frequently in cats for middle ear disease and TECA-LBOs are reserved for disease of the external ear canal, which is typically either inflammatory or neoplastic.4,14,15 The anatomy of the feline ear makes observation of surgically relevant structures during this procedure challenging. Owing to the presence of the bony septum in the cat, a ventrally extended LBO is necessary to enter the hypotympanum for access to perform curettage. For perspective and surgical planning, the diameter of the external acoustic meatus was measured and found to be 5 mm, making the depth of the LBO required to enter the hypotympanum approximately twice the diameter of the external acoustic meatus in the cat. This finding may serve as a useful intraoperative guideline for surgical planning and training.
In dogs, incomplete curettage of the tympanic bulla results in recurrent ear abscessation and deep tissue infection.1,6 Reported rates of postoperative deep surgical site infection, abscessation and fistulation range from 2% to 54%.2,4,6–9,16 The lack of a septum in dogs allows for access into the tympanic bulla directly after the tympanum is penetrated and a lateral osteotomy facilitates thorough curettage. The clinical consequence of not entering the hypotympanic cavity and subsequent incomplete curettage is less well described in cats and the incidence of incomplete penetration into the hypotympanum in the clinical setting is unknown. An experimental study examining morphologic aspects of the tympanic bulla after TECA-LBO in 20 cats revealed incomplete curettage and aural secretions in 9/20 cats postoperatively. 11 These cats were purpose-bred, had no preoperative middle ear disease and were euthanized at 8 and 16 weeks postoperatively so development of long-term, postoperative complications could not be assessed. In the largest study of 44 cats receiving a TECA-LBO, no postoperative periaural abscessation was reported. 4 In this study, 41% of feline TECA-LBOs were performed as treatment of aural neoplasia and so it is unlikely that these patients exhibited the same degree of inflammatory debris that is seen in canine end-stage otitis media externa. As this study did not document postoperative imaging in these cats, whether the hypotympanic cavity was entered in these patients remains unknown. In another study, cats were more likely to have a TECA-LBO as treatment for a periaural mass, as opposed to chronic inflammatory conditions, and exhibited a shorter timeframe of clinical signs prior to undergoing surgery. 14 More studies are needed to assess the clinical consequence of incomplete curettage in cats.
The surgeons were not blinded to the purpose of this study; therefore, the finding that the experienced surgeon failed to enter the hypotympanic cavity in 25% of the procedures was unexpected. We suspect that this finding is likely explained by a lack of surgical references with specific guidelines and the relative depth needed to enter the hypotympanum in a cat. The mean distance from the external acoustic meatus ventromedially to enter the hypotympanum was found to be 10 mm, which is subjectively deep compared with the overall size of a cat’s skull. Clinically, larger or more aggressive osteotomies and curettage could increase the risk of known complications such as facial nerve paralysis or neuropraxia, Horner’s syndrome, hypoglossal nerve injury, inner ear injury and vestibular signs or hemorrhage from the retroarticular vein or carotid artery.4,5,14 Horner’s syndrome and facial nerve paralysis are postoperative complications that are signifcantly more likely in cats compared with dogs. 14 Alternately, larger osteotomies may decrease the risk of reported complications by improving visualization of structures surrounding the bullae and allowing thorough curettage. 1 In both cats and dogs, the sympathetic nervous plexus is located at the dorsolateral aspect of the osseous septum and in cats courses through the communication in the osseous septum. While there are few described anatomic differences between the course of the tympanic plexus in cats and dogs, the tympanic plexus may be more fragile in cats, putting this species at higher risk of iatrogenic surgical trauma from aggressive osteotomies. 4
This study assessed the amount of bulla removed using CT, a cross sectional imaging modality. The differences in osteotomy size between the novice surgeon and experienced surgeon were found to be significant, independent of observer. The significantly larger osteotomies performed by the experienced surgeon may reflect a superior familiarity with the surgical anatomy of the feline bulla or a confidence that comes with greater clinical experience with this procedure. The finding that regardless of surgeon experience, significantly more bone was removed in surgeries in which the septum was penetrated, may be useful as a guideline for this procedure. Based on these results, postoperative assessment of osteotomy size can be performed equally well by a novice surgeon, an experienced surgeon or a radiologist. The experienced surgeon performed larger osteotomies, best demonstrated by the statistically significant difference in overall measured values. When the hypotympanum was entered, this study showed a correlation with larger osteotomies (P <0.03).
In this study, operative time was significantly less for the experienced surgeon compared with the novice surgeon, which is an expected finding. In a study assessing veterinary surgery residents performing hemilaminectomies, residents experienced a rapid decrease in surgical time over the initial 10 cases, followed by a more gradual decline. 17 This somewhat mimics the curve seen in this study; however, no feedback was given to the novice surgeon during this study. No improvement in septum penetrance was seen over successive surgeries, which reflects the fact that none of the CT images were assessed until completion of all procedures. If CT images were assessed sequentially after each TECA-LBO procedure, we would expect rapid and successive improvement in entry to the hypotympanic cavity by the novice surgeon.
The major limitation of this cadaveric study was the inability to correlate surgical data and imaging findings to clinical sequelae and potential development of postoperative complications. Additionally, no cadavers had ear disease detectable on images, gross examination or during surgery, which may have affected the ease of our osteotomies and dissection, compared with clinically affected cats. Furthermore, introduction of surgical bias is possible given that the experienced surgeon trained the novice surgeon during the pilot phase of the study on a cadaver not included in the analysis. However, the cadaver that was used for training was imaged postoperatively (data not shown), confirming that the experienced surgeon successfully entered the hypotympanum during instruction. Finally, no histopathology was performed in this study, so thoroughness of bulla curettage was not evaluated.
Conclusions
Although TECA-LBOs are performed less routinely in cats than dogs, this study describes the important differences between the species with respect to surgical approach. We recommend a ventromedial osteotomy of approximately 10 mm in depth to ensure penetration of the septum and allow for complete curettage of the hypotympanum. In addition, this study suggests that postoperative CT may be beneficial for both novice and experienced surgeons to confirm entry into the hypotympanum and provide immediate feedback to improve surgical technique over time.
Footnotes
Acknowledgements
The authors thank Dr Judith Jayawickrama for the statistics performed in this study.
Author note
This study was presented at the ACVS Surgery Summit in Las Vegas in October 2019.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Funding was provided through a Department of Clinical Sciences Grant at Oregon State University.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognized high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee was therefore not necessarily required.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.