
Abstract
To investigate the efficacy and safety of the treatment of percutaneous endoscopic debridement (PED) and continuous lavage drainage (CLD) on lumbar tuberculosis. Total 31 patients diagnosed with lumbar tuberculosis, who underwent the PED and CLD from January 2012 to January 2018 in our hospital were included. The operation time, intraoperative blood loss, complications were analyzed. The recovery of local tuberculosis was evaluated by erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and visual analogue scale (VAS) before and after operation. The patients were followed up for 18 to 84 months. At the last follow-up, lumbar lordosis (LL), the Japanese Orthopaedic Association (JOA) score and imaging data were used to evaluate the recovery of spinal structure and function. There were no complications for all patients. During the follow-up of 3 to 12 months after operation, ESR and CRP returned to normal. The VAS score of local pain was significantly lower than that before operation (p < 0.05). The LL and JOA scores of the patients at the last follow-up were significantly better than those before operation (p < 0.05), and the lumbar CT and MR suggested the healing of vertebral lesions.
PED and CLD might be an effective surgical treatment for spinal tuberculosis.
Introduction
Spinal tuberculosis is the most common extrapulmonary tuberculosis, while lumbar tuberculosis accounts for the majority of spinal tuberculosis. The incidence of spinal tuberculosis has increased due to the large increase of floating population and the emergence of resistant bacteria. However, with the improvement of living standards and medical conditions, spinal tuberculosis can be diagnosed and treated earlier. 1 For early spinal tuberculosis, if the traditional surgery with complete debridement, internal fixation, bone graft fusion is performed, it will not only increase the patient’s pain, but also bring a considerable economic burden to the patient. 2 With the development of medical technology, from January 2012 to January 2018, 31 patients with early lumbar tuberculosis were treated with percutaneous spinal endoscopy and vertebral lesions. The authors retrospectively analyzed and summarized its clinical efficacy and safety.
Methods
Patients
A total of 31 patients were enrolled. Patients diagnosed with lumbar spinal tuberculosis by diseased vertebra biopsy were all treated with oral antituberculosis drugs for 3 months. Subsequent to the hospital for spinal endoscopy, follow-up (18–84) months with an average of 46 months was performed. General information of patients was shown in Table 1.
Patients’ demographic characteristics.

The clinical manifestations of 31 patients were tuberculosis, low back pain with limited movement and other local symptoms, CT and MRI images confirmed single vertebral body lesions, can be complicated with intervertebral space and paraspinal psoas major muscle abscess.
Inclusion criteria
Inclusion criteria were typical clinical symptoms of tuberculosis infection, the pathological biopsy of vertebral body lesions and positive culture of Mycobacterium tuberculosis was confirmed as tuberculosis infection. Through CT and MRI imaging examination, the infected vertebral body was controlled in a vertebral body segment, and there was a large piece of dead bone formation, which might be accompanied by peripheral psoas abscess and intervertebral space involvement. Preoperative X-ray examination showed lumbar lordosis LL < 50°. Neurological function Frankel grade showed D and above. The patient was informed and voluntarily signed informed consent and approved by the ethics committee. 3
Exclusion criteria
CT showed severe bone destruction (> 1/2 volume of the vertebral body) or a cold abscess away from the lesion. The kyphosis was obvious (LL > 50°). Neurological function Frankel grades patients showed below grade D. Patients with cognitive dysfunction or mental illness were also excluded.
Surgical instruments and material preparation
Spinal endoscopy system, microscopic nucleus clamp, microscopic high-speed grinding (or ultrasonic bone knife), RF electrode, 3000 mL irrigation saline 1–3 bags, negative pressure drainage tube 1 set, epidural anesthesia catheter 1 root were used. All patients underwent intravenous + local anesthesia. Intravenous bolus of sufentanil 0.1 μg/Kg body weight 10 mins before surgery, followed by dexmedetomidine hydrochloride 0.2–0.7 μg/Kg.h speed pump maintenance was administrated to maintain the patient can wake up state. Local anesthesia was performed with 10 ml of 2% lidocaine and 0.75% ropivacaine hydrochloride.
All patients underwent surgery through the posterolateral approach. The patient’s prone position was located at the oscillating operating table arch frame, the conventional disinfection drapes, the intraoperative X-ray C-arm positioning the diseased segment, and the vertebral body destruction serious side and the upper edge as the target. A puncture point was opened (10–12) cm apart from the intervertebral space on the corresponding segment.
After the puncture point was localized, the target puncture was performed with a special puncture needle that could be placed into the guide wire. The subcutaneous, deep fascia and the surrounding tissue of the target site and the periosteum were fully localized in the puncture path. After successful puncture, a small incision of about 8 mm was made at the puncture site and the subcutaneous deep fascia was bluntly separated, then the puncture needle was pulled out. Under the guidance of the guide wire, a pencil-like dilatation guide with a diameter of 5 mM was used to bluntly puncture the target to the target. The rod was placed in the working channel (Figure 1(a) and (b)).

Patients underwent surgery through the posterolateral approach. (a) and (b) intraoperative fluoroscopy puncture in positive and lateral position; (c) intraoperative mashing of large dead bone in the focus; (d) and (e) removal of hardened bone around the focus and drilling on the outer bone of the hardened bone; The focus of vertebral tuberculosis was cleared and drainage tube could be seen by CT after (f) operation.
The entire process was carried out under C-arm fluoroscopy. Place the endoscope system in the working channel and continue to rinse with saline. Radiofrequency electrodes were used to clean the ligaments and soft tissues around the target segment of the lesion and to stop bleeding. Then using high-speed grinding or ultrasonic bone knife (the early use of high-speed grinding in our hospital, ultrasonic bone knife introduced into the country after the use of ultrasonic bone knife) at the target site according to the size of the lesion to open the vertebral cortex until the lesion, with a nucleus pulposus clear Dead bone in the lesion (large bones are broken with an ultrasonic bone knife), tuberculous granulation tissue and necrotic tissue (Figure 1(c)). After cleaning the lesion, using a high-speed grinding or ultrasonic bone knife to remove the surrounding hard bone from the edge of the lesion to the periphery, and drilling holes in the outer bone of the hardened bone (Figure 1(d) and (e)).
A large amount of saline was used to wash the lesion, and a self-made lavage drainage tube was placed (the epidural anesthesia catheter was inserted from the drainage hole at the front end of the negative pressure drainage balloon to the front end of the drainage tube about 1 cm, and was fixed with a silk thread) (Figure 1(f)). Local iodophor disinfection, suture 1 needle, covered with sterile dressing, complete surgery.
Immediately after the operation, the saline was used to lavage and vacuum-absorbed for 24 h until the drainage fluid was clear (usually about 7 days). After extubation, the patient could properly move under the protection of the waist and gradually increase the amount of activity. After 12 months of regular anti-tuberculosis drug treatment, the total course of treatment can be extended 18 to 24 months. The liver and kidney function were measured every 2–4 weeks during the medication to see if there was drug-induced liver and kidney damage. ESR and CRP was measured to reflex the inflammation. Lumbar X-ray, CT and MRI were examined at 1 month, 3 months, 6 months, and 12 months after surgery. Followed up was performed once a year until the image confirmed the healing of the vertebral lesions.
Observation index
The time to remove the lesions in the vertebral body during surgery, the amount of intraoperative blood loss, and surgical complications (including large blood vessels, spinal cord or nerve damage) were recorded. The operation was evaluated, and the postoperative ESR, CRP, and visual analoge scale VAS scores 4 were used to assess the local tuberculosis recovery. Lumbar lordosis (LL), Japanese orthopaedic association JOA 5 and other indicators to assess the structural and functional recovery of the spine. Parallel image review was used to evaluate the healing of vertebral lesions.
Recovery assessment
The scoring system for the recovery were (1) good overall condition, normal body temperature, good appetite. (2) local symptoms disappeared, no pain, sinus closed. 33 times of erythrocyte sedimentation rate were normal. (3) imaging findings abscess disappeared or even disappeared, or calcified; no dead bones, the contour of the lesion edge is clear. (4) After getting out of bed for 1 year, the above four indicators can still be maintained. 6
Statistical analysis
Statistical analysis was performed using SPSS.24.0 statistical software. The measurement data were expressed
Results
In this study, all 31 patients were followed for at least 18 months, with an average follow-up of 18 to 84 months (mean 46 months).
Surgery completion
All patients successfully completed the operation. Intraoperative vertebral lesion clearance time was (19–46) minutes, with an average of (33.52 ± 7.07) minutes. The intraoperative blood loss was (20–65) mL, with an average of (37.13 ± 10.91) ml. There were no complications such as vertebral segmental arteries, spinal cord and nerve root injury.
Followed up 3 to 12 months after surgery
The local pain was relieved and the VAS score was significantly lower after surgery (p < 0.05) (Figure 2). ESR and CRP were measured three times in (3–12) months in all patients, and all returned to normal and continued to decrease (p < 0.05) (Table 2).
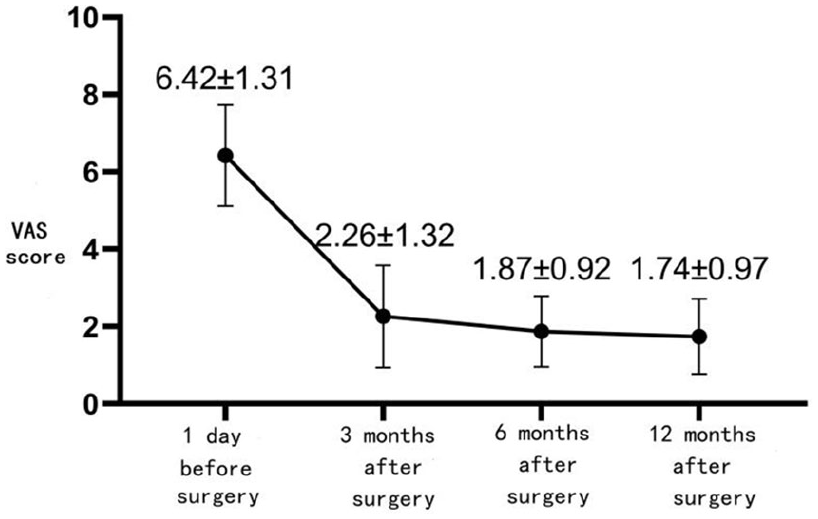
At 3 to 12 months after operation, the VAS score of low back pain was significantly lower than that before operation (p < 0.05).
Comparison of ESR and CRP before and after operation (

Erythrocyte sedimentation rate and C-reactive protein measured three times after operation (3–12 months) returned to normal, and the difference was statistically significant compared with that before operation (p < 0.05).
Last follow-up
The lumbar spine structure and function were improved significantly in all patients. LL value decreased significantly after surgery, while JOA score increased significantly after surgery (p < 0.05) (Table 3). At last follow-up, the vertebral abscess was calcified, with no dead bones, and the contour of the lesion was clear (Figures 3 and 4).

Represent of a male patients, 21 years old. Low back pain with left lower limb radiation pain for 2 months. MR and CT of lumbar vertebrae before (a)–(d) showed bone destruction of L4 vertebral body with dead bone formation, swelling of left psoas major muscle and formation of cold abscess. 12 months after (e)–(h) operation, lumbar MR and CT showed that psoas major muscle swelling subsided, cold abscess absorbed and L4 vertebral bone reconstruction.

Represent of a female patient, 19 years old. Low back pain with right lower limb radiation pain for 3 months. MR and CT of lumbar vertebrae before (a)–(d) showed bone destruction of L2 vertebrae with dead bone formation, swelling of right psoas major muscle and formation of cold abscess. 12 months after (e)–(h) operation, lumbar MR and CT showed that psoas major muscle swelling subsided, cold abscess absorbed and L2 vertebra bone reconstruction.
Comparison of LL value and JOA score before and after last follow-up (

Discussion
Indications of the use of percutaneous spinal endoscopy in lumbar tuberculosis
Effective anti-tuberculosis treatment is the basis for the treatment of spinal tuberculosis. Many studies have reported that spine tuberculosis is formed for the stability of the spine, the absence of spinal nerve compression symptoms, and the absence of large dead bones and cold abscesses. It can be cured by early, combined, moderate, regular, and full-course drug treatment. Once a dead bone or a cold abscess is formed, conservative treatment is often difficult to achieve, and surgical intervention is necessary. For a long time, open surgery for lesion clearance and reconstruction of spinal function is the golden standard procedure for the treatment of lumbar tuberculosis. However, open surgery often causes large trauma, long operation time, great damage to the spine structure, and there is a risk of accelerated degeneration of adjacent segments after internal fixation and increased postoperative infection. At the same time, when general condition of tuberculosis patients is poor, the open surgery under general anesthesia is also dangerous.7,8
For the early lumbar tuberculosis with slight structural damage of the lumbar spine, percutaneous spinal endoscopy through the continuous lavage drainage of the lesions in the vertebral body combined with anti-tuberculosis drugs is effective. At the same time, the overall structure of the lumbar spine is also restored. The data of this group showed that the LL value of the lumbar spine before treatment decreased from preoperative (42.61 ± 2.81)° to (33.58 ± 1.79)° at the last follow-up. Since the operation was minimally invasive surgery, it did not require built-in materials and it was performed under local anesthesia. The postoperative recovery was faster, and the economic burden of the patient was also reduced. At the same time, the internal fixation was eliminated to increase postoperative infection and accelerate the rapid degeneration of adjacent segments.
Minimally invasive paraspinal abscess clearing lavage drainage or vertebral lesion clearance lavage drainage
Early vertebral tuberculosis with ineffective anti-tuberculosis drugs was often combined with paraspinal abscess and dead bone in the vertebral body. In the past, CT-guided paraspinal abscess tube placement with anti-tuberculosis drugs continued to lavage or drainage and achieved certain effects.9 –12 However, previous minimally invasive treatment of lumbar tuberculosis often underwent CT-guided anesthesia epidural catheter in the peri-vertebral abscess, and post-administered anti-tuberculosis drugs for up to 1 month or longer for lavage drainage. On one hand, the patient was exposed to excessive radiation during the operation, and the CT room disinfection measures were limited, which might cause cross infection. On the other hand, the anesthesia catheter was too thin, which was easy to be blocked and easy to fall off during the postoperative washing process. Long-term anti-tuberculosis drug flushing not only increased the bedtime and hospital stay, but also increased the risk of tuberculosis drug resistance. At the same time, the drug entered the blood through the surrounding tissue, and the systemic side effects of the drug were increased at the basis of oral drugs, especially the effects on liver and kidney function. 13
With the rise of spinal endoscopy and the emergence of high-efficiency bone-cutting tools such as high-speed grinding and ultrasonic bone knives,14,15 vertebral lesions and surrounding abscesses can be treated under endoscopy. 16 Due to the dense distribution of the lumbar plexus around the lumbar spine, there are important structures such as the inferior vena cava, abdominal aorta and kidney in front to avoid damage. At the same time, considering that anti-tuberculosis drugs are easy to enter into the soft tissue around the vertebral body. We prefer to enter the vertebral body through the “safety triangle” enclosed by the upper vertebral body, superior articular process and upper nerve root. The tuberculosis lesions in the vertebral body and the inner layer of the surrounding hardened bone was removed. The outer layer of hardened bone was kept in parallel to facilitate the entry of tuberculosis drugs into the lesion.
This study showed that there were no nerves, large blood vessels and important structural damage during the operation. Postoperative anti-tuberculosis drugs could reach the vertebral body lesions through the drilling hole and spread to the surrounding cold abscess through soft tissue, without local chemotherapy of tuberculosis drugs. The local tissue could reach the effective drug concentration, thereby exerting the basic role of anti-tuberculosis drugs and accelerating the rapid recovery of lumbar tuberculosis.
Postoperative lumbar deformity
It was reported that spinal deformity did not improve significantly in mild spinal tuberculosis through drug conservative treatment. 17 It might be caused by that only through drug treatment, spinal tuberculosis recovery is slow. In the course of drug treatment, tuberculosis further destroys the structure of the vertebral body, bone absorption and loosening, excessive activity of the patient, resulting in further compression of the vertebral body. This study showed that at the last follow-up, the LL value of the lumbar spine became smaller, which was significantly improved compared with that preoperatively. The reason might be related to the following reasons. Firstly, the removal of lesions by surgery is beneficial to the rapid control of tuberculosis and reduces the further damage of tuberculosis to the vertebral body. Secondly, during the operation, the outer layer of hardened bone is preserved, which can provide strong support for the vertebral body and avoid collapse of the vertebral body. Thirdly, the patient’s preoperative vertebral destruction of the vertebral body and the stimulation of the surrounding structure by the abscess are compensated by increasing the LL value. After the operation, the control of the tuberculosis, the absorption of the abscess, and the disappearance of the protective reflex was performed. The function is restored to the maximum extent. 18 Of course, as the average age of the patients in this study is not large, the vertebral bone structure is still good, and the number of cases is too small, further research are needed.
Conclusion
In summary, spinal endoscopic vertebral lesion removal and lavage drainage for lumbar tuberculosis has a short operation time, less intraoperative blood loss, safe and effective. It can provide a new surgical treatment for spinal tuberculosis. However, it is necessary to strictly control the indications for surgery. It is feasible for patients with severe vertebral body damage to cause obvious deformity of the spine, therefore, it is necessary to continuously improve the treatment on spinal tuberculosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from The Second Affiliated Hospital Of Chongqing Medical University.
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.