
Abstract
Case series summary
A retrospective multicenter case series of renal fusion anomalies in cats was investigated. The aim of this study was to describe the imaging characteristics (radiography, ultrasonography and CT) of renal ectopia and fusion in cats. A total of 13 feline patients (median age 9 years) were included in this multicentric retrospective study. Ultrasound was available in 12/13 cases, radiographs in 4/13 cases and CT in 3/13 cases. Of the 13 cases, seven were left to right fusions, four were right to left fusions, one was on the midline and one was in the pelvic inlet. Adopting a human classification system, there were five lump kidneys, four disc kidneys, one horseshoe kidney, one caudal ectopia, one L-shaped kidney and one pelvic kidney. In 2/13 cases, additional congenital malformations were noted, including an azygous continuation of the caudal vena cava and a peritoneal-pericardial diaphragmatic hernia.
Relevance and novel information
This study provides further description of the imaging findings in feline patients with fused renal ectopia. The morphologic characteristics of the fused kidneys in cats appear similar to what is published in the human literature. Renal fusion might be an incidental finding in cats, but further investigations are necessary to determine their clinical relevance.
Introduction
Renal fusion is a rare condition in veterinary medicine but is a relatively common congenital malformation of the urinary tract in humans.1–3 The three main types described in the literature are horseshoe kidneys, crossed fused renal ectopia (CFRE) and fused pelvic kidney (pancake kidney). 1 Renal fusion is often asymptomatic but has been reported in association with other congenital malformations and may predispose to several complications, such as recurrent urinary tract infections or calculi. 2 Horseshoe kidney is the most common renal fusion anomaly in humans, accounting for 90% of cases. 3 It refers to partially fused kidneys on either side of the vertebral column. CFRE is characterized by an ectopic kidney that has crossed the midline and partially fused with the contralateral orthotopic kidney. It is the second most common type of renal fusion in human medicine, with male predominance and the left kidney being most commonly ectopic. 3 A fused pelvic kidney is the least common type of renal fusion described in human medicine, consisting of a complete renal fusion at the level of the pelvic cavity and two short orthotopic ureters.1,4,5
There are several published classifications of CFRE in humans: 6 lump kidney is classified as extensive renal fusion that forms an irregular mass/lump; disc kidney displays fusion along the medial concave surface of both kidneys; inferior ectopia is when the ectopic kidney is fused to the inferior pole of the orthotopic kidney; superior ectopia is when the ectopic kidney is fused to the superior pole of the orthotopic kidney; sigmoid or S-shaped kidney is when the ectopic kidney is axially rotated and inferior to the orthotopic kidney; and L-shape kidney is characterized by the ectopic kidney being transversely oriented and the upper pole of the ectopic kidney being fused to the lower pole of the orthotopic kidney.6,7 Inferior crossed fusion is reported to be the most common type in humans.7,8
There are a few case reports describing CFRE in cats, but no specific classification system pertaining to CFRE exists for cats.9–12 The published data show that this condition has occurred in both male and female cats of varying ages and breeds. The left and right kidneys have been documented to cross the midline and fuse to the contralateral kidney. Of four published cases, three were considered incidental findings, with only one case reporting concurrent polydipsia, polyuria, renal failure and systemic hypertension. 10 One case also details two additional congenital malformations, including an atypical portal vein and coccygeal deformation. 12 To the authors’ knowledge, there is only a single case report describing fused pelvic kidney and a single case report of horseshoe kidney in cats in the veterinary literature.9,13
Prior case reports of CFRE have classified the fusion types according to the classifications described in the human literature. The authors in this case series have elected to adopt the McDonald classification system, 6 with slight adjustment to the anatomical directional terms used in animals compared with people, when describing the different morphologic features of CFRE. Figure 1 presents a schematic representation of the six different renal fusion types.
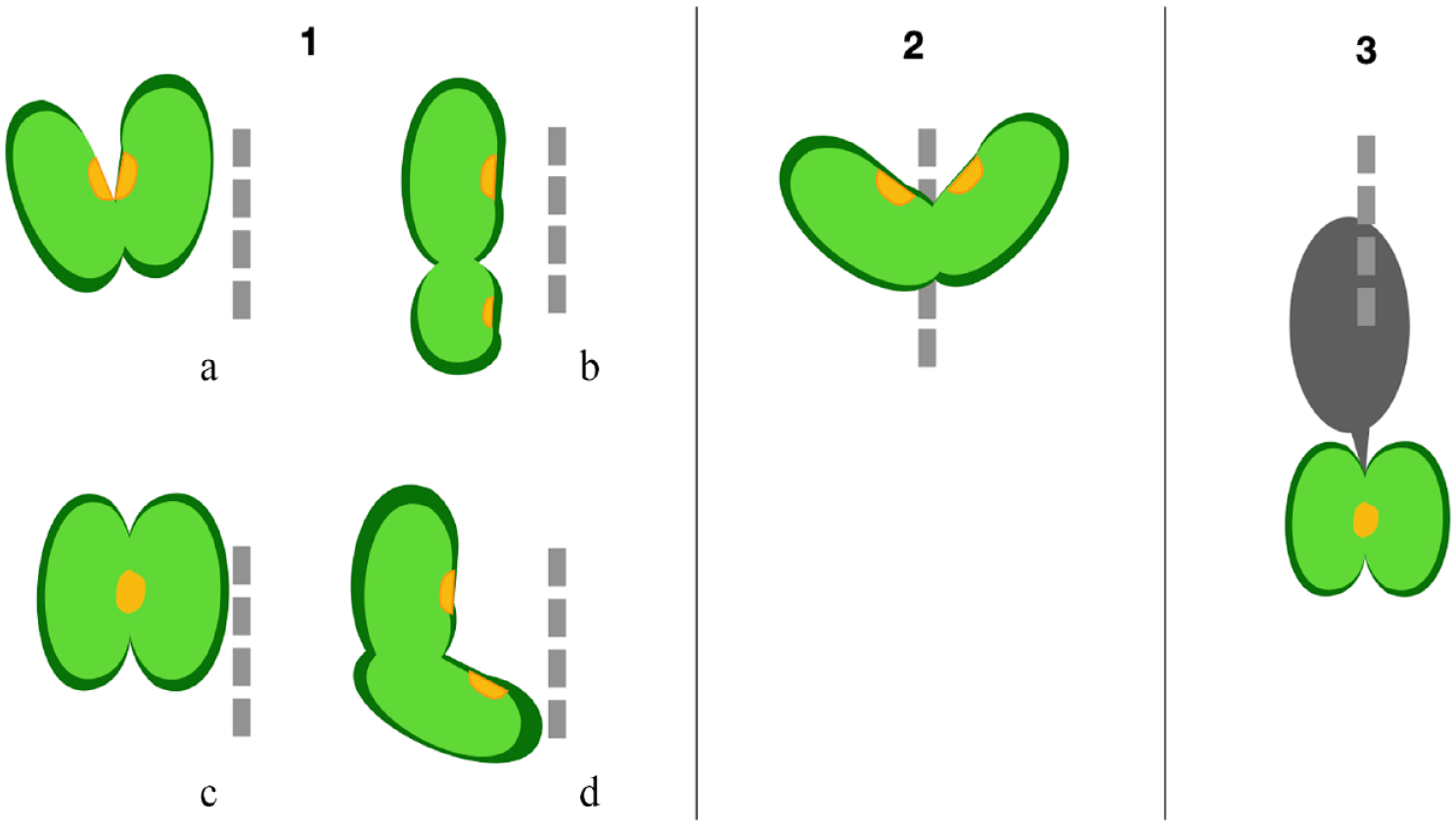
Schematic representation of the different renal fusion types: (1a) disc kidney; (1b) caudal ectopia; (1c) lump kidney; (1d) L-shaped kidney; (2) horseshoe kidney; (3) pelvic kidney (pancake kidney)
Case series description
Cases with suspected renal fusion anomalies were retrospectively selected by searching the keywords ‘kidney fusion’, ‘ectopic kidney’ and ‘horseshoe kidney’ from the databases of multiple institutions (Cummings School of Veterinary Medicine at Tufts University [North Grafton, MA, USA], Veterinary Hospital I Portoni Rossi Anicura Italy [Bologna, Italy], University of Barcelona [Barcelona, Spain], Dick White Referrals [Cambridgeshire, UK], Justus-Liebig-University [Giessen, Germany] and Vetmeduni Vienna [Vienna, Austria]) between 2005 and 2021. Data from medical records were collected, including signalment, history and any abdominal imaging studies performed. The case images, including ultrasound (US) still images and videoclips for each case, radiographs and complete CT studies where available, were reviewed by a rotating intern (PS) and a board-certified radiologist (AA).
In total, 13 feline patients were included in this series (Table 1). There were nine castrated male cats and four spayed female cats. The median age was 9 years (range 1–13 years). The breeds included domestic shorthair (n = 6), domestic mediumhair (n = 2), domestic longhair (n = 1), Persian (n = 1), Persian mix breed (n = 1), Exotic Shorthair (n = 1) and one British Shorthair (n = 1). Clinical signs at the time of presentation included anorexia (n = 4), lethargy (n = 4), hyperthermia (n = 2), abdominal pain (n = 2), weight loss (n = 2), vomiting (n = 2) and dysuria (n = 2).
Signalment, presenting complaint, imaging modalities and ectopia classification
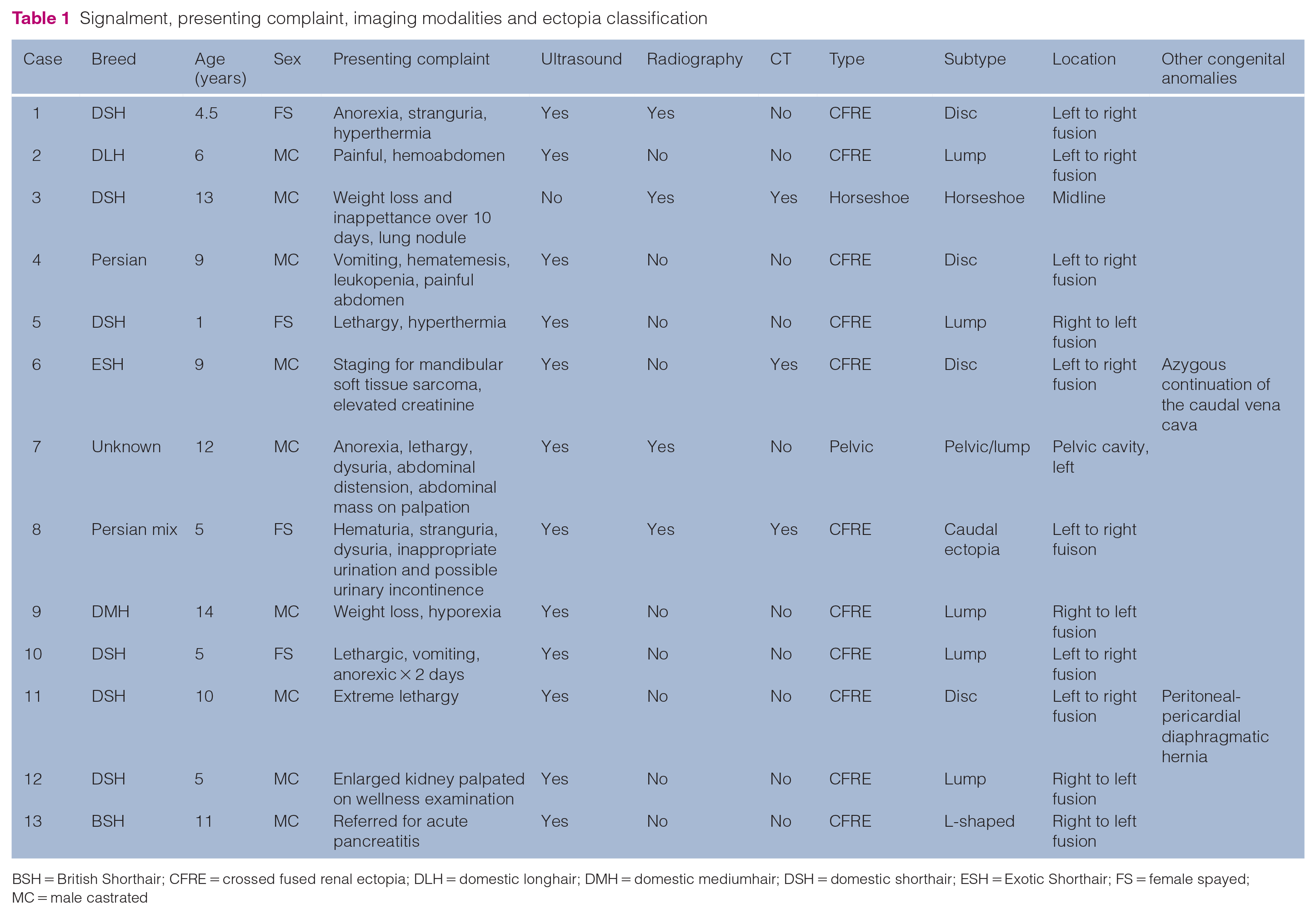
BSH = British Shorthair; CFRE = crossed fused renal ectopia; DLH = domestic longhair; DMH = domestic mediumhair; DSH = domestic shorthair; ESH = Exotic Shorthair; FS = female spayed; MC = male castrated
Of the 13 cases, there were 11 cases of CFRE, including the following: five lump kidneys characterized by an extensive renal fusion of both kidneys forming a single renal mass with two independent pelves opposite each other (Figure 2); four disc kidneys exhibiting partial cortical fusion on the medial aspect of both kidneys with two independent renal pelves opposite each other (Figure 3); one caudal ectopia where the ectopic kidney was small and located caudal to the orthotopic kidney and fused by their cranial and caudal poles, respectively (Figure 4); and one L-shaped kidney, where the renal pelves were not opposite each other but oriented in different directions (Figure 5). Seven cases were classified as left to right fusions, and four were right to left fusions.

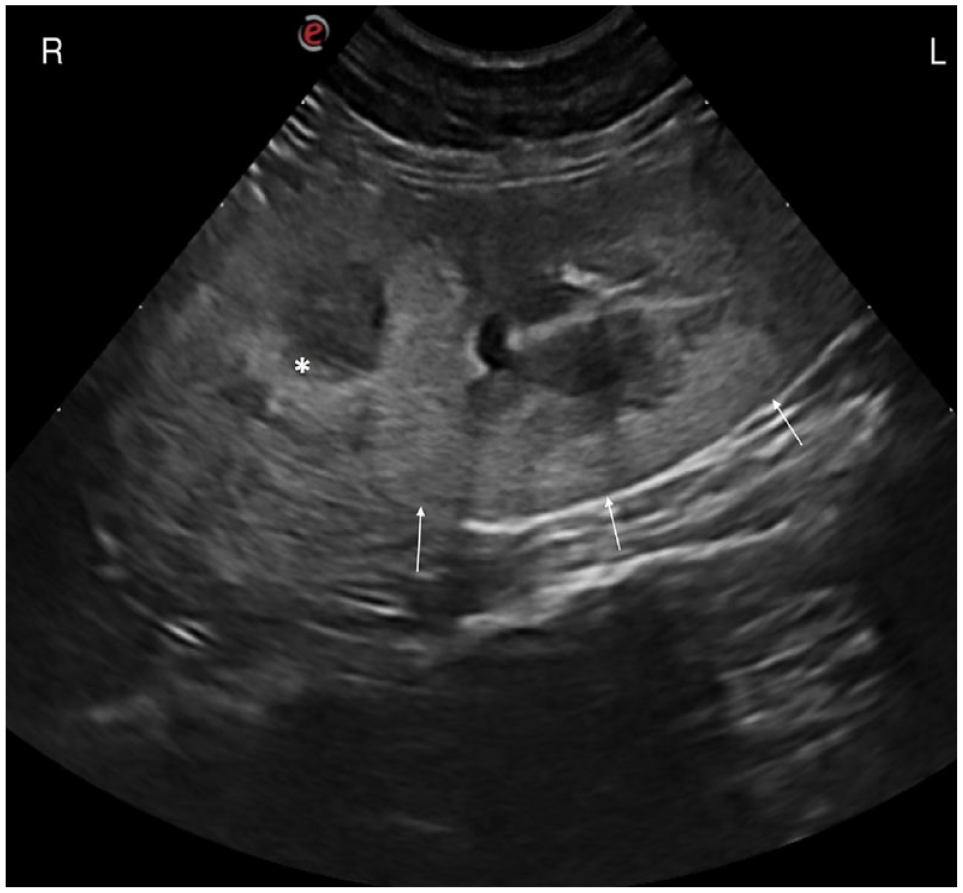
Ultrasonographic transverse image of a lump kidney showing extensive renal fusion of both kidneys forming a single renal mass. L = left; R = right

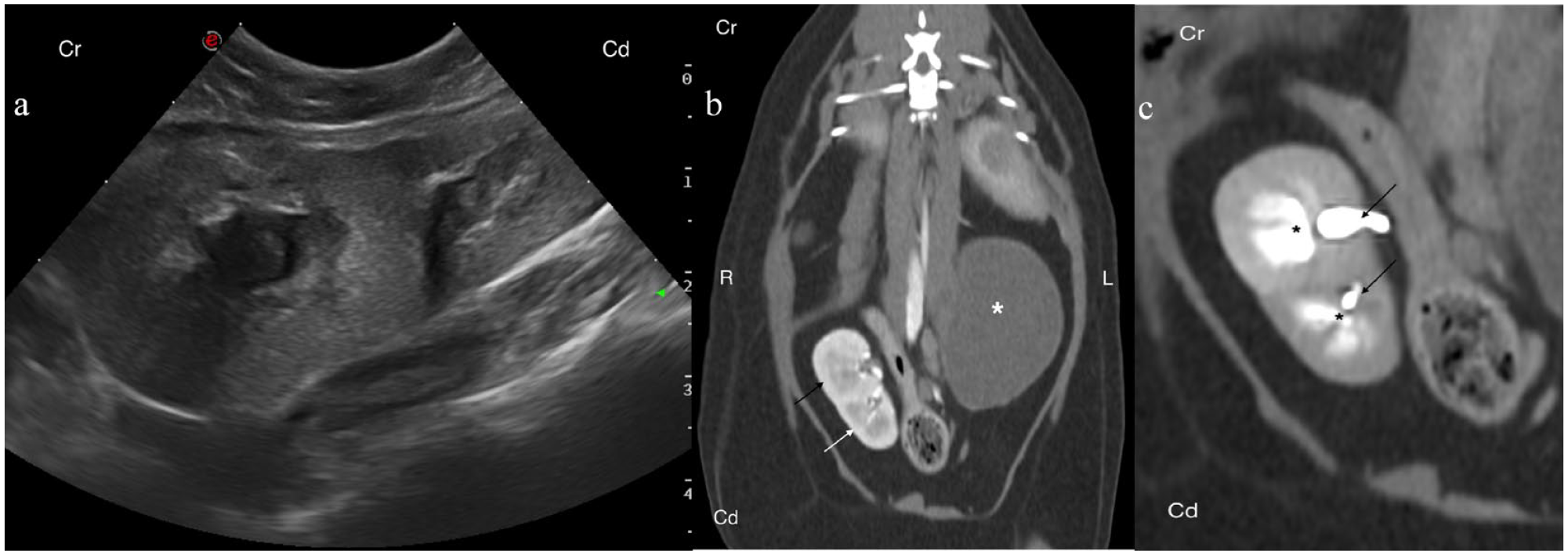
(a) Ultrasonographic transverse image of a disc kidney displaying partial cortical fusion on the medial aspect of both kidneys. (b) Post-contrast dorsal reformat CT image of the same case. The renal structure is right of the midline; the kidneys are partially fused along their caudal cortical margins and the pelves are opposing each other. (c) Zoomed image of the same kidneys in panel (b). The white arrows highlight two separate ureters. The black asterisk indicates the renal pelves. Window width = 400, window level = 40. Cd = caudal; Cr = cranial; L = left; R = right
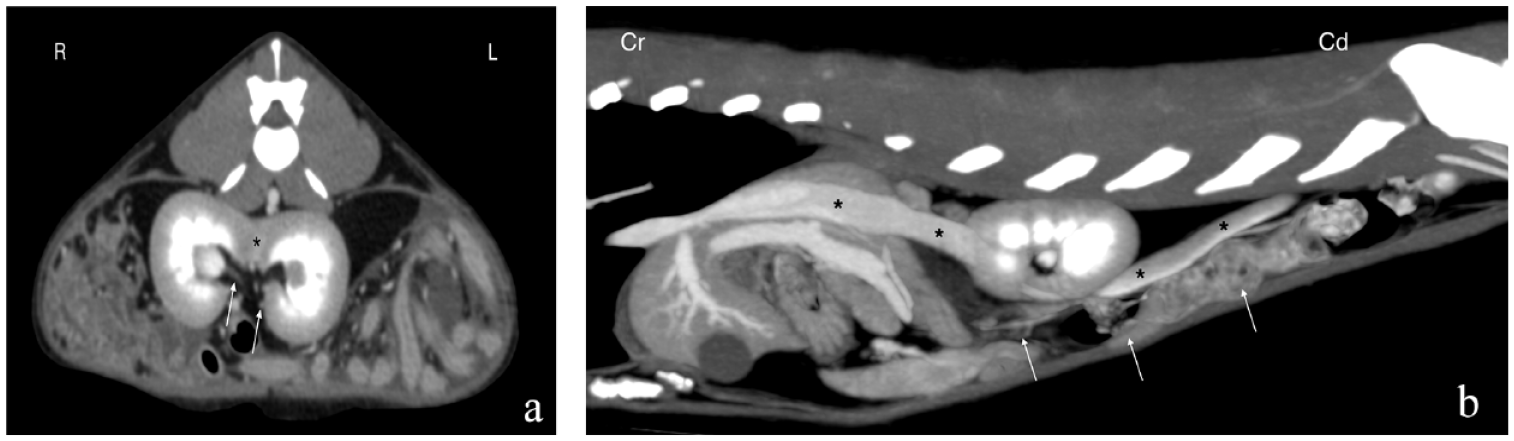
(a) Ultrasonographic sagittal image displaying caudal ectopia. The orthotopic kidney and ectopic kidney are fused by their caudal and cranial poles, respectively. (b) Post-contrast dorsal reformatted CT image of the same case. The ectopic kidney (white arrow) is small and located caudal to the orthotopic kidney (black arrow) and fused by their cranial and caudal poles, respectively. The bladder is located to the left (asterisk). (c) Zoomed image of the same kidneys in panel (b). The black arrows highlight two separate ureters. The black asterisk indicates the renal pelves. Window width = 400, window level = 40. Cd = caudal; Cr = cranial; L = left; R = right
Ultrasonographic transverse image of an L-shaped kidney where the renal pelves are oriented in different directions. The caudal kidney is seen on a sagittal plane (arrows), while only a transverse image of the caudal pole of the right kidney is seen (asterisk). L = left; R = right
One case was classified as a horseshoe kidney (1/13), which was characterized by two distinct kidneys present on both sides of the vertebral column and fused together by their caudal poles, forming an isthmus of normal renal parenchyma on midline (U-shaped) (Figure 6). The kidneys were located between the caudal vena cava and descending colon (ventral), and the aorta (dorsal).
(a) Transverse post-contrast CT image of a horseshoe kidney characterized by two distinct kidneys on both sides of the vertebral column and fused together by their caudal poles, forming an isthmus of normal renal parenchyma on midline (asterisk). The arrows point to two separate ureters. (b) Sagittal post-contrast reformatted CT image with MIP of the same case. The kidneys displaced the caudal vena cava (asterisks) and descending colon (arrows) ventrally. WW = 400, WL = 40. Cd = caudal; Cr = cranial; L = left; MIP = maximal intensity projection; R = right; WL = window level; WW = window width
One case presented with a fused ectopic kidney at the level of the pelvic cavity (pancake kidney) (1/13), caudal to the urinary bladder. This renal mass also displayed morphologic characteristics of a lump kidney as it had extensive renal fusion of both kidneys and fused renal pelves.
US was available in 12/13 cases. US allowed the identification and classification of the type of fusion in all cases. Information regarding renal vasculature and insertion of the ureters was not available in any case. Other US changes included reduced corticomedullary distinction (8/12), increased cortical echogenicity (6/12) and pyelectasia (6/12).
Four cases had radiographic studies available for review. In one case, the fused kidneys were located on the midline (1/4), corresponding with the horseshoe kidney. Two of the four cases had a right-sided soft-tissue opaque mass and in 1/4 cases, the fused kidney was located caudally in the pelvic inlet and was more left-sided.
Three cases had CT pre- and post-contrast series available for review. The ureters could be evaluated in these studies and were noted to implant into the urinary bladder at the appropriate locations. Two renal arteries and two renal veins were identified for each pair of kidneys.
In 2/13 cases, additional congenital malformations were noted. In one case, the patient was noted to have a peritoneal-pericardial diaphragmatic hernia (PPDH) identified on echocardiogram. In the other case, the abdominal vena cava displayed segmental aplasia, enlarged vertebral veins and azygous continuation of the caudal vena cava.
Discussion
For the four published feline cases of CFRE, one case was classified as S-shaped 12 ; however, in this case, both kidneys were ectopic in the pelvic cavity, one L-shaped 9 and one inferior fusion. 10 In the fourth report, the author did not describe the fusion type. 11 In addition, left to right fusion was the most common type (in 3/4 cats).9–12 Evaluation of the ectopia type for the 13 cases in this series showed that left to right fusion was the most prevalent, similar to the previous published cases. In this series, 5/13 cases were classified as lump kidney and 4/13 were classified as disc kidney. These two fusion types are the most similar in appearance. Only one case in this population displayed inferior crossed fusion (classified here as caudal ectopia given the differences in anatomical position between humans and cats), which is the most common type in humans.
CFRE is reported to be more common in males vs females in the human literature. 7 For the four published cases, two cases were in male cats and two cases were in female cats.9–12 In this series, 9/13 cases were in male cats and 4/13 were female cats. These results are consistent with this anomaly being reported to occur more commonly in males vs females.
Only one case in this series had significant azotemia (blood urea nitrogen >130, creatinine 8.6) and two additional cases had reported mild azotemia. Owing to a lack of complete case history and clinicopathological data, and the retrospective nature of the study, the authors cannot say whether these were a prerenal, renal or postrenal cause of azotemia, nor whether these patients had true renal dysfunction or elevated renal values from a separate cause. CFRE is commonly an incidental finding in humans; it is rarely reported to be the cause of renal insufficiency but rather more commonly associated with complications such as pyelonephritis, recurrent urinary tract infection, nephrolithiasis, vesicoureteral reflux, hydronephrosis and cancer.1,2,14
Ultrasonography is a useful imaging modality to evaluate the renal morphology in cats.14,15 Common US findings of patients with chronic kidney disease include increased cortical echogenicity, abnormal corticomedullary distinction, poorly discernable internal architecture, abnormal shape and decreased renal size.14,16 The majority of patients in this series had either reduced corticomedullary distinction, increased cortical echogenicity or evidence of pyelectasia. Whether this renal anomaly results in altered kidney function or predisposes a patient to chronic kidney disease was not determined in this case series. Sarhan et al 17 determined that, on follow-up, 14% of their human patients with CFRE developed chronic kidney disease. In this series, US was proven valuable in determining the location of the renal structure within the abdominal cavity and most of the morphologic features; however, the authors acknowledge the limitations of US evaluation in the absence of a definitive diagnosis.
For the available radiographic studies, the authors were able to identify a soft-tissue opaque mass in the region of the kidney, as well as lack of a soft-tissue opaque mass where an orthotopic kidney should be located. Renal ectopia and fusion can be a differential for a soft-tissue opaque mass in the abdomen when the kidneys are unable to be located at the normal radiographic position.
In the available CT studies, the ureters and renal vasculature appear unaffected by this anatomic anomaly. Two renal arteries and two renal veins were identified for each pair of kidneys, and the ureter draining the ectopic kidney eventually crossed the midline and implanted at its normal position on the urinary bladder. In humans with this condition, it is uncommon for the ureters to be affected.6,18 Few human cases have been documented detailing CFRE with either a single renal ureter or vessel and only a single case detailing both a single ureter and renal vein. 19
One case in this series was classified as a horseshoe kidney on CT. Unfortunately, there were no US images available for review for this case. To the authors’ knowledge, there is only one other published case report of horseshoe kidneys in cats. 13 Horseshoe kidney is reported to be the most common renal congenital anomaly in humans. The true incidence in cats is unknown; however, it appears to be a rare fusion anomaly.
A separate case in this series showed similar morphologic abnormalities to a published case in that the kidneys displayed ectopia and fusion but were located ectopically in the pelvic canal. Hebel et al 12 detail a left to right fusion of the renal mass, with an S-shaped classification, as well as being located in the pelvic canal. The case in this series located the renal mass ectopically in the pelvic canal and displayed morphologic characteristics similar to that of a lump kidney. Both cases display both crossed ectopia and fusion, as well as ectopia in the pelvic canal. Kubihal et al 1 state that in cases of fused pelvic kidney (also known as pancake kidney), the renal mass shows extensive medial fusion of the kidneys, but the ureters are short, do not cross the midline and implant at their normal location on the urinary bladder. This is different from the published feline case, in which the ureters are noted to be short, but the ureter connected to the ectopic kidney does cross the midline before implanting into the urinary bladder. Unfortunately, there are no CT data available for the case in this series, so the authors were unable to trace the ureters and determine whether they crossed the midline.
One case in this series had a concurrent PPDH, which is reported to be one of the most common midline congenital abnormalities in cats aged above 2 years. 20 Reimer et al 21 evaluated 66 cats with PPDH and documented additional congenital abnormalities, but CFRE was not one of them. A separate case in this series presented a continuous azygous vein with segmental aplasia of the caudal vena cava and enlarged vertebral veins. To the authors’ knowledge, this is the first case reporting this finding in cats. This congenital abnormality is both rare and usually an incidental finding and has been documented in both humans and dogs.22–24 Owing to the retrospective and multicentric nature of this study, as well as the lack of detailed history and case follow-up information, determination of the clinical significance of this condition is difficult.
Conclusions
In this case series of cats, crossed renal ectopia and fusion was the most prevalent type of renal fusion. Left to right fusion was the most common presentation. Males were over-represented. Renal fusion might be an incidental finding in cats, but further investigations are necessary to determine their clinical relevance.
Footnotes
Acknowledgements
The authors would like to thank Drs Borbala Lőrincz, Sergio Monteagudo and Harald Hechinger for their contribution of cases to this series.
Accepted: 3 August 2023
Author note
The abstract for this submission was presented at the 2022 American College of Veterinary Radiology Annual Scientific Meeting, Silver Legacy Hotel, Reno, Nevada on 18 October 2022.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.