
Abstract
Objectives
Thrombocytosis is an uncommon hematologic abnormality that is associated with various physiologic, metabolic, inflammatory and neoplastic conditions in people and dogs. Thrombocytosis is not a well-described abnormality in cats. The objective of this study was to classify thrombocytosis in cats based on underlying disease processes and severity, and to compare this with a control population of cats.
Methods
A retrospective study was conducted by reviewing the medical records of cats with increased (
Results
In total, 158 cats were identified with thrombocytosis, with 315 cats in the control group. Non-neoplastic inflammatory disease was the most common diagnosis in both groups (54.4% in cats with thrombocytosis and 56.2% in controls; P = 0.77); however, gastrointestinal diseases were more common in cats with thrombocytosis (75.6%) when compared with controls (34.5%; P <0.0001). Neoplasia was diagnosed more frequently in cats with thrombocytosis (44.3%) compared with the control group (25.4%; P <0.0001). Round cell tumor was the most common neoplasia diagnosis in both groups, but gastrointestinal and multicentric lymphoma were diagnosed more frequently in cats with thrombocytosis compared with control cats. No association between the severity of thrombocytosis and etiology was identified.
Conclusions and relevance
Thrombocytosis in cats is more commonly associated with gastrointestinal, hepatobiliary or immune-mediated diseases when compared with a control population. Neoplasia, especially multicentric and gastrointestinal lymphoma, was more commonly diagnosed in cats with thrombocytosis when compared with control cats.
Introduction
Thrombocytosis refers to an increased number of platelets in peripheral blood with respect to the species-specific reference interval. Thrombocytosis is categorized as either a primary or secondary process. 1 Primary thrombocytosis is a term used to describe a rare myeloproliferative neoplasm, also called essential thrombocythemia.1,2 In secondary, or reactive, thrombocytosis, the number of circulating peripheral platelets is increased either by redistribution or through increased production of platelets secondary to an underlying disease process.1,3 Primary and secondary thrombocytosis have been described in people and in dogs, but there is minimal information about thrombocytosis in cats. In people and dogs, reactive thrombocytosis is described more commonly than primary thrombocytosis.4 –8 This reactive increase in circulating platelets can be transient, most often seen as a rebound effect upon recovery from events such as acute blood loss or splenectomy.5,9 Other causes for transient thrombocytosis include physiologic mobilization of platelets from the spleen or other stores. These causes include exercise, excitement or a response to drugs such as epinephrine (adrenaline) and glucocorticoids.5,9 When reactive thrombocytosis is more sustained, underlying diseases such as neoplasia, chronic inflammatory diseases, trauma, endocrinopathies and iron deficiency can contribute to an increase in circulating platelet number.1,3,10 –12 It is theorized that these disease processes are associated with an increase in inflammatory cytokines such as interleukins 1, 6 and 11 (IL-1, IL-6, IL-11) and chemokine ligand 5 (CCL-5), which can then increase production of thrombopoietin (TPO) and subsequently increase production of platelets.3,12
In dogs, several studies have identified neoplasia as the most common condition associated with thrombocytosis, though severity of thrombocytosis has not been found to be predictive of underlying diagnosis.5 –8 Within neoplastic diagnoses in dogs, carcinoma was the most common tumor type, resembling carcinoma-associated thrombocytosis in people. 6 Few studies have investigated the association between the severity of thrombocytosis and underlying conditions in cats. Rizzo et al evaluated 51 cats with thrombocytosis, and inflammatory/infectious disorders were the most common diagnosis in this population, and no associations with severity were identified. 13 That study did not include a control population so it is unclear if the distribution of diagnoses in these cats can be attributed to the thrombocytosis or if it could represent the typical distribution of clinical cases at this institution.
A better understanding of the diseases most commonly associated with thrombocytosis in cats would be helpful in guiding the diagnostic evaluation of cats. Thrombocytosis in people, namely essential thrombocythemia and paraneoplastic thrombocytosis, carries an increased risk of thromboembolic complications and is used as a prognostic factor in certain cancers.4,14,15,16 In cats, an increased risk of thromboembolic complications secondary to thrombocytosis has not been demonstrated, though a previous case report described a cat with an aortic thromboembolism, a marked thrombocytosis and concurrent neoplasia. 14 More information regarding this abnormality is necessary to determine the future research potential or clinical impact.
The purpose of this retrospective study was to describe the pathologic conditions associated with thrombocytosis in cats, and to investigate whether the severity of thrombocytosis was predictive of the diagnosis in cats with thrombocytosis.
Materials and methods
A search of the medical records was completed for the period between January 2011 and September 2018 for cats that had a complete blood count (CBC) performed and for which a platelet count was included. The hematologic analyzer (Abbott Cell Dyn 3700; Abbott Laboratories) used at this institution has not been validated for platelet count in cats and therefore, CBC data were not used to characterize platelet count for the cats in the study, but rather the presence of a CBC was only used as the search criteria to identify cases. The institutional protocol includes that all CBCs performed have a platelet count estimation performed by microscopic evaluation of blood smears.The microscopic evaluation was performed by trained medical technologists in all cases. The use of microscopic evaluation for platelet count estimation has been validated in cats.
17
The estimation involves counting the number of platelets per oil immersion field (1000 × magnification) in 10 microscopic fields of the monolayer. The mean platelet count is then multiplied by 15 to provide the platelet number × 103/µl of blood. The 100 × lens used in this study has an ocular ‘field number’ (FN) of 22, corresponding to our use of the multiplication factor of 15.
16
Thrombocytosis is defined in this study as a platelet count estimate greater than
For cats meeting the inclusion criteria for thrombocytosis, medical records were reviewed for signalment, diagnoses and other CBC data. Diagnostic testing was not documented in detail for each cat, but the results of feline leukemia virus (FeLV) and feline immunodeficiency virus (FIV) testing, serum iron testing and bone marrow samples were recorded if they were performed. Diagnoses were classified broadly into either neoplasia, endocrine or non-neoplastic inflammatory disease. Within each of these broad categories, diagnoses were grouped based on tumor type(s), metabolic disorder(s) or body system(s) affected, respectively. It was also noted if each cat had diagnoses in multiple categories. If no underlying disease was identified in the medical record search, the cat’s thrombocytosis was considered idiopathic. Some cats had multiple CBCs performed during the period but only the first documentation of thrombocytosis for each cat was included in the study.
Using the initial search criteria for any cat with a CBC performed during the stated period, and after excluding any cat with platelet clumping, the remaining cats were then organized by ascending date of birth. This list arranged cats by age and each cat with thrombocytosis was identified on this list. Two cats of the same age (one on either side of each thrombocytosis cat) with a platelet count estimate within normal limits (200–599 × 103/µl) were then selected for the control group in order to allow age-matching. A larger control group was selected to allow for a more robust representation of the typical population of cats and their varied diagnoses. Diagnoses for the control group were categorized in the same manner described above.
Comparisons between the two groups of numerical data were conducted using the Wilcoxon rank sum test. Comparisons of proportions of categorical data were conducted using the χ2 test of independence. In analyses, values of P <0.05 were considered statistically significant. Statistical analyses were conducted using commercially available software (Stata version 16.1; StataCorp).
Results
During the study period, 6547 CBCs were performed in cats. Of these, 311 cats were identified with platelet count estimates >600 × 103/µl. Significant platelet clumping was noted in 153 of these blood smears, so these were excluded. This resulted in 158 cats being included in the study. Based on the samples, the incidence of thrombocytosis in cats was 2.4% during the 8 years of this study. The control group contained 315 cats with platelet count estimates within normal limits. The mean age of the thrombocytosis group was 9.79 ± 4.9 years, and the mean age of the control group was 9.87 ± 4.9 years (P = 0.89). Sex distribution of cats in the thrombocytosis group consisted of three (1.89%) intact males, 80 (50.6%) castrated males, five (3.2%) intact females and 70 (44.3%) spayed females. Sex distribution of cats in the control group consisted of five (1.6%) intact males, 167 (53.2%) castrated males, eight (2.6%) intact females and 134 (42.7%) spayed females. Sex distribution was not statistically significant when comparing the two groups (P = 0.97). There were eight breeds represented in the thrombocytosis group. The most common were the domestic shorthair (n = 128, 81.0%), domestic mediumhair (n = 9, 5.7%), domestic longhair (n = 6, 3.8%) and mixed breed (n = 6, 3.8%). There were 17 breeds represented in the control group. The most common were the domestic shorthair (n = 217, 69.1%), mixed breed (n = 23, 7.3%), domestic longhair (n = 21, 6.7%), Siamese (n = 15, 4.8%), domestic mediumhair (n = 12, 3.8%) and Maine Coon (n = 7, 2.2%).
Mild thrombocytosis was identified in 120 (75.9%) cats (range 600–795 × 103/µl). Moderate thrombocytosis was identified in 20 (12.7%) cats (range 810–990 × 103/µl and marked thrombocytosis was identified in 18 (11.4%) cats (range 1005–1470 × 103/µl).
No diagnosis was recorded in nine (5.7%) cats with thrombocytosis, so these were termed idiopathic as there was inadequate information to assign a diagnosis of primary or essential thrombocytosis. No cats in either group had a bone marrow evaluation or a serum iron profile performed during the same visit as the CBC which led to their inclusion in the study. Retroviral testing was available in 42 (26.5%) cats with thrombocytosis and 122 (38.7%) control cats. One cat with thrombocytosis and 12 control cats were positive for FIV antibody. Four control cats and none of the cats with thrombocytosis had a positive result for FeLV antigen. These numbers were too small to allow for any meaningful statistical evaluation. Information regarding the stress or anxiety associated with blood collection was not available in any case pertaining to physiologic causes for transient thrombocytosis.
Of the cats with thrombocytosis and a documented diagnosis, 86 (54.4%) were diagnosed with non-neoplastic inflammatory disease, 70 (44.3%) were diagnosed with neoplasia and 48 (30.4%) were diagnosed with endocrine disease. A total of 50 (31.7%) cats had diagnoses in multiple categories, leading to the sum of major diagnostic categories to be greater than 100%. Of the major diagnostic categories, neoplasia and endocrine disease were diagnosed more frequently in cats with thrombocytosis compared with the control group (P <0.0001 and P = 0.0012, respectively) (Table 1). In addition, cats with diagnoses in multiple broad categories were noted more frequently in the thrombocytosis group compared with the control group (P <0.0001). Non-neoplastic inflammatory disease was diagnosed in a similar percentage of cats in both groups (P = 0.77) (Table 1). When distributed by severity of thrombocytosis, there were no significant associations between severity and any diagnostic category (P = 0.68) (Table 2).
Distribution of diagnoses of 158 cats from the first documentation of thrombocytosis and 315 control cats

Data are n (%). Distribution of diagnoses for the thrombocytosis and control cats differed significantly (P <0.001)
Significant differences in frequency of diagnosis
Distribution of 158 cases of thrombocytosis by severity in each of the major diagnosis categories
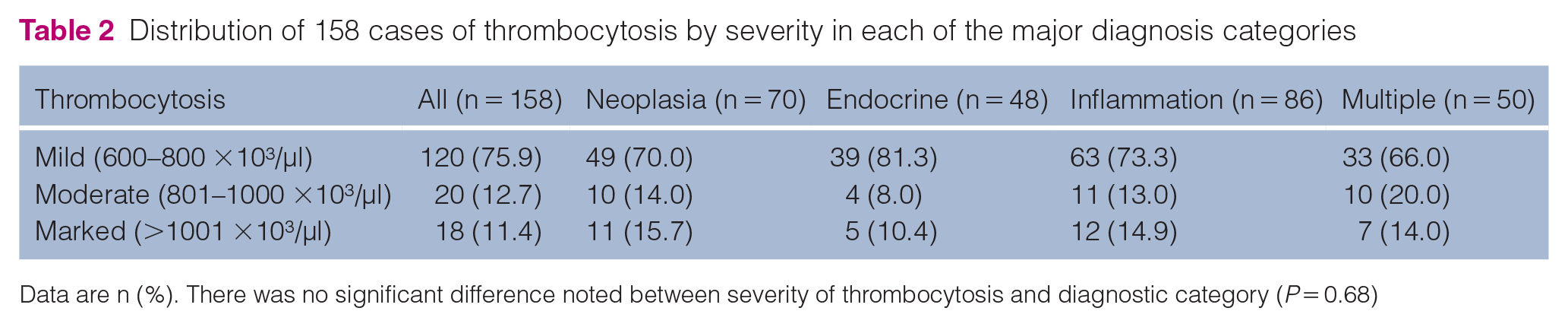
Data are n (%). There was no significant difference noted between severity of thrombocytosis and diagnostic category (P = 0.68)
Neoplasia was diagnosed in 70 cats with thrombocytosis; of those, 48 (68.6%) were diagnosed with a round cell tumor, 16 (22.9%) were diagnosed with carcinoma and seven (10.0%) were diagnosed with sarcoma. Although neoplasia was diagnosed more frequently in cats with thrombocytosis compared with the control group, no significant difference was found when comparing tumor types, with round cell tumor being the most common tumor type in both groups (Table 3). There was a significant difference between groups when comparing specific round cell tumor diagnoses within all neoplastic diagnoses. Gastrointestinal and multicentric lymphoma were more frequently diagnosed in the thrombocytosis group when compared with the control group (P = 0.03 and P = 0.01, respectively) (Table 4). Iron deficiency was not definitively diagnosed in any cat but is commonly associated with gastrointestinal diseases and with a microcytic hypochromic anemia. Three cats with thrombocytosis had a microcytic, hypochromic anemia with platelet count estimates of 645, 1050 and 1335 × 103/µl, respectively. All three of these cats had a diagnosis of neoplasia, with two cats diagnosed with gastrointestinal lymphoma (645 × 103/µl and 1050 × 103/µ) and the third diagnosed with a left pelvic limb fibrosarcoma (1335 × 103/µl). None of the control cats had a microcytic, hypochromic anemia.
Distribution of cases diagnosed with neoplasia by tumor type, endocrinopathy by disease type and non-neoplastic inflammatory disease by body system(s) affected
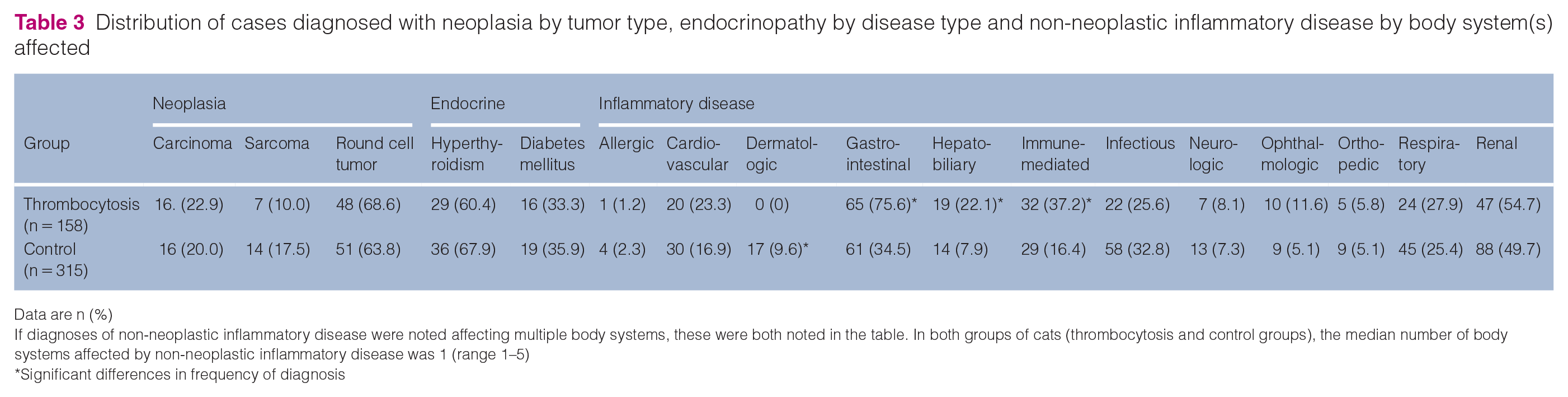
Data are n (%)
If diagnoses of non-neoplastic inflammatory disease were noted affecting multiple body systems, these were both noted in the table. In both groups of cats (thrombocytosis and control groups), the median number of body systems affected by non-neoplastic inflammatory disease was 1 (range 1–5)
Significant differences in frequency of diagnosis
Anatomic distribution of lymphoma as described in the medical record of 90 cats with or without thrombocytosis

Data are n (%)
Anatomic distribution of lymphoma as described in the medical record of 90 cats with or without thrombocytosis
Significant differences in frequency of diagnosis
The most commonly diagnosed endocrine diseases in both groups were hyperthyroidism and diabetes mellitus. Other endocrine diseases were diagnosed, including those affecting the parathyroid gland and the adrenal gland; however, there were too few of these cats to allow for statistical analysis. Although endocrine disease was diagnosed more frequently in cats with thrombocytosis compared with the control groups, similar percentages of cats were diagnosed with hyperthyroidism and diabetes mellitus when comparing the two groups (Table 3).
A similar percentage of cats were diagnosed with non-neoplastic inflammatory disease between groups (54.4% of thrombocytosis cats and 56.2% of control cats). Within this category, however, diseases of specific body systems were diagnosed with different frequencies between groups (Table 3). Gastrointestinal disease was the most common body system affected in cats with non-neoplastic inflammatory disease and thrombocytosis (65/86, 75.6%) and was diagnosed significantly more frequently in these cats when compared with control cats (61/177, 34.5%; P = 0.0024). Hepatobiliary and immune-mediated diseases were also diagnosed more commonly in cats with thrombocytosis than control cats. Conversely, dermatologic diseases were diagnosed more commonly in the control group than the thrombocytosis group (Table 3).
Discussion
The incidence of feline thrombocytosis in this study was lower when compared with previous reports where thrombocytosis was noted in 3.6% and 4.6% of cats, respectively.7,13 Had the cats with significant platelet clumping been included, this study would have yielded an incidence of thrombocytosis in cats of 4.8%. Platelet clumping is a common blood smear finding in cats due to platelet activation during venipuncture, with platelet clumping identified in up to 70% of feline blood samples. 18 When significant platelet clumping is present, the automated platelet count obtained from a hematology analyzer can be considered a minimum.18–20 Therefore, it is likely that some of the cats excluded due to platelet clumping had thrombocytosis, and therefore the distribution of diagnoses may have been different, had clumped samples been included. However, estimating thrombocytosis microscopically on a feline blood smear with clumping present would rely too heavily on subjective estimation to be meaningful data. Thus, future studies to prospectively investigate different reagents for the collection of feline blood that may decrease platelet clumping, including citrate, theophylline, adenosine and dipyridamole (CTAD) collection tubes (Becton, Dickinson), would be useful.
Physiologic conditions causing an increase in catecholamines can result in thrombocytosis. Stress or anxiety in cats associated with restraint or venipuncture may have caused catecholamine-induced thrombocytosis. However, the influence of this possibility on the platelet count estimates in this population of cats could not be assessed objectively, and so the physiologic contribution to thrombocytosis cannot be evaluated in this study.
Non-neoplastic inflammatory disease was the most common diagnosis in cats with thrombocytosis, which is consistent with what has been identified previously. 13 In the current study, gastrointestinal disease was the most common body system affected in cats with non-neoplastic inflammatory disease and thrombocytosis, being diagnosed in approximately 75% of these cases. This is consistent with what has been reported in people and dogs, in which gastrointestinal disease, both non-neoplastic and neoplastic, have been commonly associated with thrombocytosis.4 –8,13 Neoplasia was diagnosed in slightly fewer than half of cats in this study, which was a more common diagnosis in this population of cats than has been previously reported. In a previous report of 51 cats with thrombocytosis, only six (11.7%) of those cats were diagnosed with neoplasia, and of those, only two were diagnosed with lymphoma. 13 Lymphoma was the most common tumor diagnosed in all cats in the study, occurring in a similar percentage of cats with thrombocytosis vs control cats. Previous studies of thrombocytosis in cats did not include a control group, so the diagnostic distribution among cats with thrombocytosis could not be differentiated from the general hospital population. In people, thrombocytosis is not a common finding in lymphoma.16,21 Essential thrombocythemia has been sporadically associated with lymphoproliferative disorders, but this association is weak.16,21,22 In the current study, the large number of lymphoma diagnoses in cats, regardless of platelet count, likely represents the hospital population, as lymphoma is routinely treated by the clinical oncologists, and lymphoma represents an area of ongoing research for this institution. This likely also contributes to why a higher number of cats were diagnosed with neoplasia when compared with previous reports.
Multicentric lymphoma and gastrointestinal lymphoma were more commonly diagnosed in cats with thrombocytosis when compared with the control population. This has not been reported previously. In people, gastrointestinal carcinomas are commonly associated with thrombocytosis, and in certain tumor types, such as colorectal carcinoma, thrombocytosis is a negative prognostic indicator.23 –25 Carcinoma was an uncommon diagnosis in this study, but gastrointestinal lymphoma as well as gastrointestinal inflammatory diseases were more frequently diagnosed in cats with thrombocytosis when compared with the control group. Gastrointestinal carcinoma tumor cells have been shown to produce IL-6, which, in turn, increases thrombopoiesis. 25 It is not known if tumor cells in feline lymphoma directly produce IL-6 as a paraneoplastic mechanism, but IL-6 may be produced as part of the inflammatory milieu of the tumor’s chronic clinical progression, especially in virus-associated feline lymphoma.13,26–28 Feline small intestinal lymphoma has a T-cell predominant phenotype and is associated with chronic inflammatory and neoplastic changes to the gastrointestinal tract. 29 Chronic gastrointestinal disease may also be associated with low-grade gastrointestinal hemorrhage, which could lead to compensatory erythropoiesis, splenic contraction or iron deficiency, all of which have been associated with thrombocytosis.1,30
Hepatobiliary diseases and immune-mediated diseases were noted more frequently in cats with thrombocytosis when compared with controls. The liver is the primary site of TPO synthesis, so it is possible that chronic hepatobiliary disease could lead to an increase in TPO production. 3 Immune-mediated disease has been noted to be increased in dogs with thrombocytosis, speculated to be due to the common administration of exogenous corticosteroids in these diseases.6,31 A similar logic could be assumed in cats with immune-mediated disease. However, the retrospective nature of this study makes these conclusions difficult. In approximately 70% of cats diagnosed with hepatobiliary diseases or immune-mediated diseases, other diagnoses were recorded. The presence of multiple diagnoses in these cats makes it challenging to draw any conclusions about these body systems.
Marked thrombocytosis is not well described in cats. In this study, 18 cats had a platelet count estimate of greater than 1001 × 103/µl, with the highest recorded platelet count estimate in a cat with gastrointestinal lymphoma (1470 × 103/µl). This small number of cats with marked thrombocytosis precludes meaningful statistical analysis, but interestingly, the distribution of diagnoses in these cats was similar to that noted in cats with mild and moderate thrombocytosis (Table 2). The small sample size, lack of cats with primary thrombocytosis and no cats with extreme platelet counts (eg, >2000 × 103/µl) led to an inability to conclude anything about the impact or prognostic value of a marked thrombocytosis in cats.
This study represents the largest retrospective study of thrombocytosis in cats to date and is one of few studies investigating this phenomenon in domestic species. Classifying diagnosis by broad categories and primary body systems allowed for the inclusion of a large number of cases but makes it difficult to meaningfully define associations. The lack of information regarding physiological factors, such as stress or anxiety, means that this potential factor influencing the platelet count estimate in cats cannot be objectively described. This catecholamine-induced response is described broadly but has not been evaluated specifically in cats and warrants investigation. The distribution of diagnoses in cats with thrombocytosis appears unique when compared with data described in dogs and people, but a prospective evaluation would be necessary to investigate whether this finding is repeatable. The non-neoplastic inflammatory diseases were classified by body system, but specific etiology was not recorded. In addition, many cats had inflammatory diseases affecting multiple body systems, or had multiple broad diagnoses such as neoplasia and inflammatory disease, and the impact of iron deficiency could not be assessed, so the factor(s) contributing to thrombocytosis could not be elucidated beyond diagnosis. Since inflammation is a complex process influenced by many factors, future studies should include more specific measures of inflammation like serum amyloid A or C-reactive protein to allow a more meaningful investigation of association. While gastrointestinal disease has been identified in this study, and others, to be associated with thrombocytosis in cats, future targeted research should investigate if specific disease processes within this organ system are more likely to lead to thrombocytosis than others.
Conclusions
Thrombocytosis in cats is attributed to secondary or reactive mechanisms in almost all cases and is more commonly associated with inflammatory diseases of the gastrointestinal tract, hepatobiliary system or immune-mediated when compared with a control population. Neoplasia was more commonly diagnosed in cats with thrombocytosis when compared with control cats. Lymphoma, especially gastrointestinal and multicentric, is the most common tumor associated with thrombocytosis in cats. Future studies should evaluate the impact of physiologic factors, such as stress and anxiety, on feline circulating platelet numbers. Prospective evaluation of the potential use of thrombocytosis as a prognostic tool in feline neoplastic disease, namely lymphoma, is warranted.
Footnotes
Author note
A research abstract was presented at and published in the proceedings of the American College of Veterinary Internal Medicine (ACVIM) Forum 2019 in Phoenix, AZ, USA. All work was completed at the Purdue University College of Veterinary Medicine.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.