
Abstract
Case series summary
Seven cases of feline hippocampal and piriform lobe necrosis (FHN) are described, with particular emphasis on clinical, radiographic and histopathological correlations. FHN is an uncommon acute epileptic condition resembling human autoimmune limbic encephalitis and temporal lobe epilepsy. Seizures are typically focal and feature uni- or bilateral orofacial or head twitching, hypersalivation, lip smacking, mydriasis, vocalisation and motionless staring, with inter-ictal behavioural changes such as unprovoked aggression and rapid running. Emerging evidence supports an autoimmune aetiology, although disruption of hippocampal architecture secondary to brain neoplasia has also been recognised. Most commonly, however, the underlying cause remains unknown. Diagnosis is achieved clinically and with brain MRI; electroencephalography and voltage-gated potassium channel-complex autoantibodies are currently the subject of research. Affected cats are frequently refractory to conventional antiepileptic treatment.
Relevance and novel information
Following a review of the literature, including potential complicating factors and comparisons with human medicine, the hippocampus and piriform lobe are proposed as the neuroanatomical localisation for focal seizures with orofacial involvement in cats, regardless of aetiology.
Keywords
Introduction
Feline hippocampal and piriform lobe necrosis (FHN) is an acute epileptic condition characterised by focal seizures consisting of uni- or bilateral orofacial or head twitching, hypersalivation, lip smacking, mydriasis, vocalisation and motionless staring lasting approximately 5–30 s. These cats usually show inter-ictal behavioural changes such as significant unprovoked aggression or rapid running.1–7 Other less commonly reported signs are pyrexia, urinary retention, ataxia and generalised hyperaesthesia.2,3,8–10 Neurological examination is commonly unremarkable or non-specific; diagnosis is suspected based on clinical signs, supported by MRI and confirmed on post-mortem assessment. It is currently unclear whether the lesions found are the primary cause of the seizures or whether it is the seizures themselves that result in necrosis.1,5,8,9,11–13 The initial focal seizures described with FHN often progress to generalised seizures and status epilepticus, and tend to be refractory to antiepileptic treatment, which frequently leads to euthanasia.1,2,4,9,14,15
This study reports on seven cases of FHN in southeast England, reviews the available literature and compares it with the authors’ findings and experience.
Case series description
Inclusion criteria, timing and geographical origin
The MRI database of Dick White Referrals (Newmarket, UK) was searched for the words ‘hippocampus’, ‘hippocampal’ and ‘hippocampal necrosis’, over a 9-year period (2011–2020). Cats were included in the study if MRI abnormalities compatible with FHN had been detected by the reporting radiologist. Seven cases met the inclusion criteria. All cats were from southeast England (Essex, Norfolk and Suffolk). Cases 1–5 and 7 had access to the outdoors and, consequently, possible access to toxins; case 6 was an indoor-only cat. None of these cats had a medical history of seizures.
Signalment, history, and physical and neurological examination findings prior to imaging
Case 1
A 5-year-old male neutered (MN) domestic shorthair (DSH) cat was assessed for a 1-week history of focal seizures, which started after staying in a cattery. The specific ictal and peri-ictal clinical signs are summarised in Table 1. The following day the patient suffered a generalised tonic-clonic seizure that started with hypersalivation and lasted about 90 s. Upon reassessment, the haematology/biochemistry profile was unremarkable and the patient was subsequently referred. On presentation to our hospital, physical examination revealed mildly protruded third eyelids and a large firm bladder that was difficult to express; neurological examination revealed mildly reduced pelvic limb postural reactions (left worse than right). During the consultation, the patient suffered a focal seizure, which then escalated to a full tonic-clonic seizure. The cat was hospitalised and medications were administered (Table 2). Despite treatment, over the following 24 h the cat suffered five more focal seizures. Its bladder was found to be large, firm and difficult to express, requiring temporary urinary catheterisation.
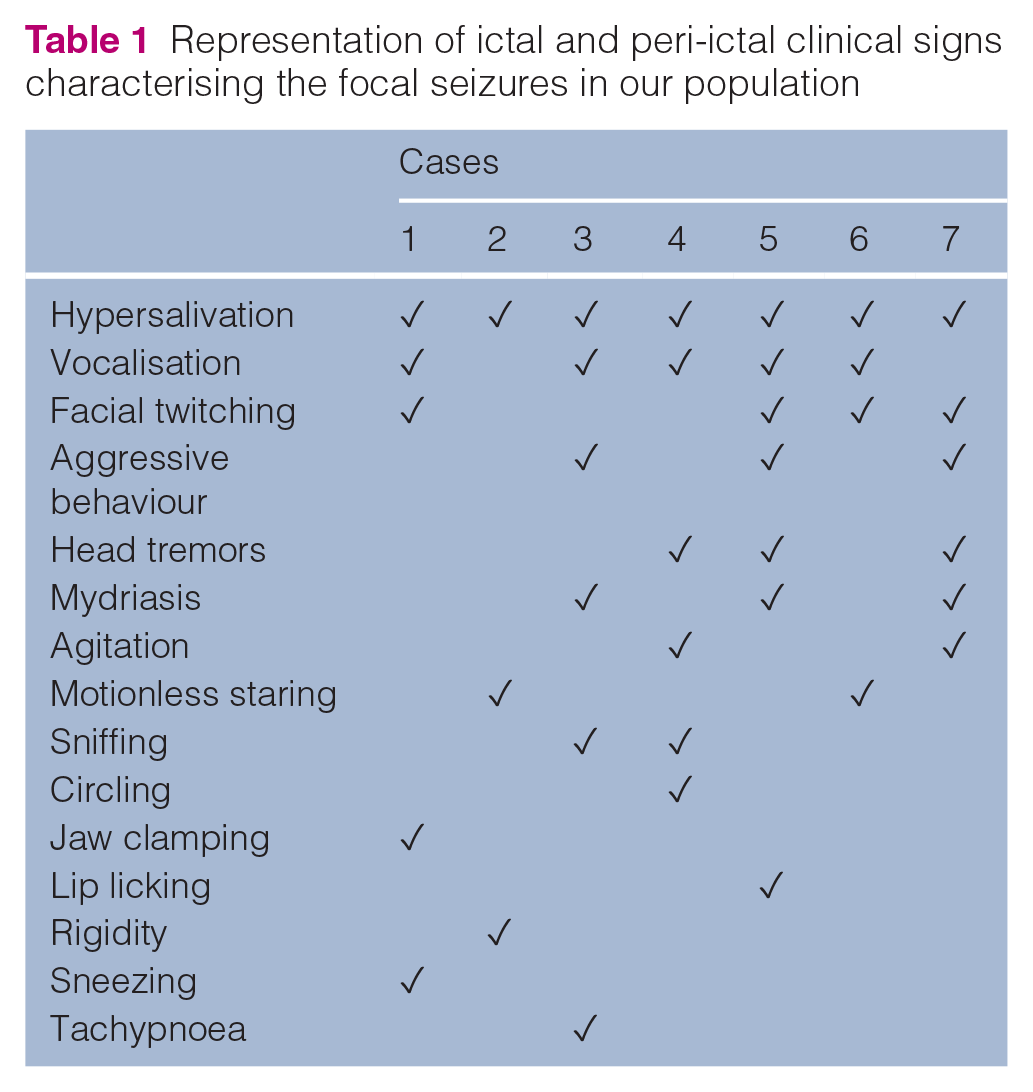
Representation of ictal and peri-ictal clinical signs characterising the focal seizures in our population
Evolution of the therapeutic protocols for each case from presentation to the referring veterinary surgeon to discharge from our hospital (correlation with outcome)

PRN = pro re nata (as required); NA = not applicable
Case 2
An 8-year-old MN DSH cat was referred following 3 days of episodic and progressively more frequent focal seizures lasting approximately 1 min (Table 1), which eventually would precede a generalised tonic-clonic seizure. Inter-ictally, the cat was subdued. On presentation, the patient was obtunded and had generalised ataxia, absent menace responses bilaterally, subjectively impaired vision, mildly reduced oculocephalic reflex bilaterally and mildly reduced postural reactions on both pelvic limbs.
Case 3
An 11-year-old MN DSH cat was assessed for sudden onset of focal seizures and diarrhoea (Table 1). On clinical examination a temperature of 39.3°C and mild-to-moderate gingivitis were noted. Over the following 24 h, the patient showed aggressive behaviour and suffered one generalised and several focal seizures. On subsequent presentation at the referral hospital, the cat was in status epilepticus and, with treatment as per Table 2, the seizures were controlled.
Case 4
A 3-year-old female spayed (FS) DSH cat was referred for multiple focal seizures and two generalised tonic-clonic seizures (Table 1), which had occurred over the previous 3 days. On presentation, physical and neurological examinations were unremarkable. After admission the patient suffered several more focal seizures lasting approximately 5–15 s, also including unprovoked hyperactivity and circling lasting approximately 2 mins; the latter seemed to be exacerbated by stress. Its temperature was 39.0°C.
Case 5
A 12-year-old MN DSH cat was assessed for the acute onset of focal seizures (Table 1). On presentation, the patient was rolling in the carrier, had passed urine and faeces, had mydriatic pupils unresponsive to light and a temperature of 41.3°C. Owing to a lack of significant response to rectal diazepam, propofol was administered. In 1 h, the patient recovered and its temperature normalised. Overnight, the cat suffered multiple focal seizures, which would stop with diazepam boluses. The following day the patient was referred. On presentation, the cat was disorientated. Physical examination disclosed a heart murmur (grade III/VI), while neurological examination revealed mildly decreased postural reactions on the left thoracic and pelvic limbs.
Case 6
An 8-year-old FS DSH cat presented to the referring veterinary surgeon for very short (5–10 s) and frequent focal seizures (Table 1). Treatment with phenobarbital (2 mg/kg q12h) was started and in 2 days the seizures stopped. The patient presented again approximately 18 months later due to seizure recurrence. The phenotype of the events was unchanged, the seizures would happen every 5–10 mins and could be controlled with diazepam boluses. On presentation, the cat’s temperature was 39.6°C. The phenobarbital dosage was initially increased to 4 mg/kg q12h but, owing to lack of improvement, over the following 36 h the dosage was increased again to 5.3 mg/kg q12h and levetiracetam was added to the treatment plan. After several doses, the patient would only hypersalivate occasionally and referral was then sought. On presentation, physical and neurological examinations only revealed anisocoria. This finding was not observed the following day.
Case 7
A 7-year-old MN DSH cat was assessed for the acute onset of agitation, unprovoked aggression towards the other cat in the household and inability to recognise the owners, which quickly progressed to more obvious focal seizures (Table 1). The patient had also been unusually lethargic and hyporexic for the previous few days and an ongoing weight loss had been noticed. On presentation, the patient was very agitated, hyper-reactive and fearful. Physical examination revealed halitosis, mild hypersalivation and subjective submandibular lymphadenomegaly. Neurological examination was limited owing to the altered mentation; the main findings were occasional head bobbing and bilateral mydriatic pupils partially responsive to light stimuli.
Diagnostic procedures
Blood tests, urinalysis and cerebrospinal fluid (CSF) analysis results can be found in Table 3; these were non-specific and, overall, unremarkable. Creatine kinase was significantly elevated, potentially owing to seizure activity (cases 4 and 5) and intramuscular sedation prior to blood collection (case 7). Urine samples were collected via urinary catheter in case 1 and via cystocentesis in cases 4, 5 and 7. CSF was collected from the cisterna magna in all patients. Brain MRI was performed in all patients under general (inhalational) anaesthesia, using a 0.4 T MRI unit (Hitachi Aperto Lucent O5). Sagittal T2-weighted (T2W) and transverse T2W, T2*, fluid attenuated inversion recovery (FLAIR), T1-weighted (T1W) and contrast-enhanced T1W images of the brain were acquired. In case 7, dorsal T2W images were additionally available and T2* was not performed in case 3. The MRI abnormalities varied from case to case (Table 4), with (T2W) hyperintensity (Figure 1) and enlargement (Figure 2) of the hippocampi commonly identified, accompanied by variable degrees of contrast enhancement (Figure 3). CSF was collected after performing imaging and under the same general anaesthesia. In case 5, a thoracic CT scan and abdominal ultrasound did not identify a cause of the seizures.
Routine bloodwork, urinalysis and cerebrospinal fluid (CSF) analysis results

Case 2 was tested for Toxoplasma gondii, bornavirus, parvovirus and feline coronavirus (FeCoV). Case 4 was tested for feline leukaemia virus (FeLV), feline immunodeficiency virus (FIV), feline herpesvirus, calicivirus, Bordetella species, Chlamydophila species, Toxoplasma gondii, bornavirus, Leishmania infantum and parvovirus. Case 6 was tested for FeCoV
RI = reference interval; NA = not applicable; ALT = alanine transaminase; AST = aspartate transaminase; ALP = alkaline phosphatase; GGT = gamma-glutamyl transferase; RBC = red blood cells; MCV = mean cell volume; MCHC = mean cell haemoglobin concentration; MCH = mean cell haemoglobin; WCC = white cell count; AGP = alpha-1-acid glycoprotein; TT4 = total thyroxine; USG = urine specific gravity; hpf = high-power field; RT-PCR = reverse transcription PCR
MRI findings for the reported cases

T2W = T2 weighted; FLAIR = fluid attenuated inversion recovery; T1W = T1 weighted; CSF = cerebrospinal fluid

Examples of T2-weighted (T2W) signal change. T2W and fluid attenuated inversion recovery transverse images at the level of the hippocampus are shown from two cases. (a) Strong and bilaterally symmetric hyperintensity in both hippocampi (case 4). (b) Asymmetric T2W hyperintensity (arrows) in the left hippocampus (case 3).

Examples of enlargement of the hippocampi. T2-weighted and fluid attenuated inversion recovery transverse images at the level of the hippocampus are shown from two cases. (a) Symmetric marked enlargement of both hippocampi (arrows) (case 4); (b) mild enlargement of the right hippocampus most apparent as it becomes larger than the left (arrowheads) (case 1).

Examples of contrast enhancement of the hippocampi. T1-weighted (T1W), T1W post-contrast and subtraction transverse images at the level of the hippocampi are shown from two cases. (a) Contrast enhancement may be subtle (best identified on the subtraction images, arrowheads) yet diffuse (case 1). (b) Focal yet asymmetric region of contrast enhancement in the left hippocampus (arrow) with a more diffuse faint patchy contrast enhancement of other portions of the hippocampus (arrowheads) (case 3).
Treatment, outcome and follow-up
The therapeutic protocols for each patient are summarised in Table 2.
Case 1
During hospitalisation, an indwelling urinary catheter was placed for bladder management. Over 4 days following the initiation of treatment, seizure frequency decreased, and at the time of discharge the patient had not had any seizure for approximately 48 h. Four weeks later the patient was still seizure-free and treatment with gabapentin was discontinued. The dexamethasone dosage was tapered over the following 3 months. The cat remained seizure-free for the following 9 months. No further follow-up was available.
Case 2
Following diagnosis, treatment with dexamethasone was started and treatment with phenobarbital was continued. Shortly after recovering from anaesthesia, the patient suffered a progressively higher number of focal seizures lasting 10–60 s, which would only temporarily stop with diazepam. At that point the owners elected for euthanasia and consented to post-mortem examination.
Case 3
The patient was discharged the day after investigations. For the following 2 months it remained seizure-free, therefore dexamethasone was tapered and stopped. Nineteen months later the cat started to suffer seizures again every 2–3 weeks. At that point phenobarbitone serum levels were 5 mg/l (reference interval [RI] 15–30) and the dosage was increased. For 1 year after this relapse, the patient remained seizure-free. The phenobarbital dosage was therefore decreased with a plan of stopping the medication within the following 6 months. No further follow-up beyond 3 years was available.
Case 4
The seizures proved difficult to control initially, but their frequency and severity reduced after a loading dose of phenobarbitone, levetiracetam and dexamethasone. The patient was also pre-emptively started on clindamycin. Four days after presentation, while hospitalised, the patient became dysuric and needed manual bladder expressions. Urinalysis and urine culture were unremarkable at that stage (see Table 3). Once recovered and seizure-free, the cat was discharged. No follow-up was available.
Case 5
The cat continued to have frequent focal seizures, which would stop only temporarily with diazepam and additional doses of phenobarbital. The patient also became pyrexic again with temperatures oscillating between 39.9°C and 40.7°C. Cytosine arabinoside was administered; however, over the following 24 h the cat continued to suffer a series of approximately 20–25 focal seizures, which could no longer be controlled. Furthermore, the cat’s bladder became consistently large, firm and very difficult to express. The owners elected euthanasia and a post-mortem examination was performed.
Case 6
Following diagnosis, the treatment plan was changed as per Table 2. At this point, phenobarbital and levetiracetam blood concentrations were, respectively, 17 mg/l (RI 15–30) and 26 mg/l (RI 5.5
Case 7
After starting dexamethasone and phenobarbital a gradual improvement was noticed, with only occasional focal seizures, normal appetite and behaviour. Levetiracetam was added to the therapeutic plan and the patient was subsequently discharged. The day after discharge, dexamethasone was increased back to 0.56 mg/kg q24h owing to seizure reoccurrence, after which the seizures stopped. Two weeks later, the cat was rechecked owing to acute lethargy, weakness, hyporexia and vacant mentation. On presentation, the patient was markedly obtunded and barely responsive. It had lost 5% of its body weight compared with 2 weeks before and a pyrexia of 39.9°C was also noted. On neurological examination it was circling to the left, head pressing and showed reduced palpebral reflex, pupillary light reflex and menace response bilaterally. At this point the patient was euthanased and a post-mortem examination was performed.
Post-mortem examination
Case 2
Microscopically, there was, bilaterally, symmetrical, multifocal, neuronal degeneration and necrosis with mild gliosis and mild perivascular cuff formation within the piriform lobes and the dentate gyri of the hippocampus, compatible with FHN.
Case 5
Histopathology of the brain revealed severe, acute, multifocal neuronal necrosis and chromatolysis with a focal proliferation of spindle cells between the left piriform lobe and the hippocampus, compatible with a fibrillary astrocytoma, to which the neuronal changes were potentially secondary. No significant inflammatory reaction was observed.
Case 7
Macroscopic examination of the brain revealed a poorly demarcated expansion of the hippocampal region and piriform lobe, which was solid, light brown and predominantly localised to the right side. Microscopically, disrupting, expanding and replacing the neuroparenchymal architecture at the level of the hippocampus, internal capsule and piriform lobe was a poorly demarcated, non-encapsulated, highly infiltrative and densely cellular neoplastic process, compatible with lymphoma (Figure 4). The neoplastic cells expanded the Virchow robin space in the adjacent neuroparenchyma, forming cuffs up to six cells thick, and were present within the meninges multifocally, ventricles and expanding the choroid plexus.

Case 7: transverse section of the brain post-fixation. There is a poorly demarcated expansion (asterisk) in the region of the hippocampus and piriform lobe on the right, which is solid and light brown with darker brown foci and causes a midline shift. On histopathology, this lesion was compatible with a lymphoma
Discussion
FHN has been reported in one publication as a relatively frequent aetiology for feline seizures, ranging between 11% and 25%. 5 Other authors considered it a rare disease or did not mention it among the causes of feline seizures at all.13,14,16 The aetiology of FHN remains unclear: there is some evidence supporting a vascular insult as the primary cause of the disease;4,17 however, the aetiology remains most frequently unknown. A neoplastic process affecting the brain and secondarily damaging the hippocampus can be considered as a differential diagnosis. Oligodendrogliomas and meningiomas have been found to cause clinical signs compatible with FHN, also in the absence of MRI findings.4,18,19 In our case series, fibrillary astrocytoma and lymphoma were diagnosed in cases 5 and 7 (Figures 5 and 6); to the best of our knowledge, these neoplasms have not previously been reported to cause focal seizures compatible with FHN. An immune-mediated inflammatory process has also been hypothesised. 2 A link between voltage-gated potassium channel (VGKC) complex antibodies and FHN has been defined,10,20,21 similarly to autoimmune limbic encephalitis (LE) causing temporal lobe epilepsy (TLE) in humans.22–24 The autoantibodies seem to be targeting leucine-rich glioma inactivating factor 1 (LGI1), which is the main known component of the VGKC complex and is strongly expressed in the hippocampal neuropil. 10 Interference with LGI1 is thought to impair its function as a VGKC complex modulator causing neuronal hyperexcitability, 10 hence the seizures. Another study conducted in a cat detected a similar autoimmune response towards other antigens leading to FHN in the absence of antibodies against the VGKC complex/LGI1. 25 In patients without evidence of inflammation on MRI, CSF and histopathology (such as case 2), it should be considered that neuronal necrosis secondary to autoimmune phlogosis could lack typical inflammatory features at later stages of disease or following treatment. In humans, 20% of LE with VGKC complex antibodies is paraneoplastic; 23 a similar link has not been demonstrated to date in cats. The fact that different aetiologies have been associated with similar presentations suggests that the characteristic phenotype of FHN is indicative of a neurolocalisation in the region of the hippocampus and piriform lobe, rather than a specific condition. In view of the documented susceptibility of the hippocampus to hypoxic insults,26,27 it seems reasonable to hypothesise that any process causing some degree of compression or disruption to the architecture of this neuroanatomical region could lead to focal ischaemia and necrosis.

Case 5, diagnosed with astrocytoma, and concurrent evidence of hippocampal necrosis. T2-weighted/fluid attenuated inversion recovery (top row) and T1/T1-weighted post-contrast (bottom row) transverse images taken at the level of the hippocampus demonstrate a marked swelling and hyperintensity of the left hippocampus with strong focal contrast enhancement (arrows, suspected location of the astrocytoma), and also some milder hyperintensity and enlargement of the right one (arrowheads).

Case 7, diagnosed with intracranial lymphoma. T2-weighted/fluid attenuated inversion recovery (top row) and T1/T1-weighted post-contrast (bottom row) transverse images taken at the level of the hippocampus demonstrate that there is marked swelling (arrows) and variable but in places strong contrast enhancement (arrowheads) of the right hippocampus, with similar but less dramatic changes in the left hippocampus (out of plane).
Although some reports suggest an infectious aetiology as the primary cause of FHN, no known infectious agent has ever been found, which was consistent with our cases. Case 6 showed increased feline coronavirus (FeCoV) serum titres and alpha-1-acid glycoprotein, but this was not deemed significant in view of the reverse transcription PCR (RT-PCR) results on CSF. The latter test has been reported to have sensitivity of up to 42% and specificity of 100% for the diagnosis of feline infectious peritonitis. 28 Furthermore, all patients were negative for the remaining known infectious causes of feline encephalitis. Considering the commonly reported pyrexia in feline and human patients with LE, which was also detected in some of our patients, a prodromal and self-limiting infection causing an autoimmune response via the mechanism of molecular mimicry cannot be excluded.21,29 Timing between the onset of clinical signs and presentation can be crucial in detecting pyrexia, as this may be associated with the acute phase of the disease. Interestingly, in both our patients with histopathologically confirmed neoplasia (cases 5 and 7), pyrexia re-occurred and/or persisted after diagnosis, while, in case 6, pyrexia was detected upon seizure re-exacerbation. Non-convulsive status epilepticus should therefore be considered as another, more likely, explanation for re-occurring pyrexia in these cases. An electroencephalogram (EEG) could also be used to reach this conclusion and guide treatment. 30
In another study, an environmental trigger such as an unknown toxin was also considered, especially in view of the fact that the reported patients were all from the same area. 1 Although this option cannot be disregarded for most of our patients, who were also outdoor cats, toxicity represents a less likely explanation for indoor cats,9,14 such as case 6.
To date, there is controversial evidence as to whether FHN represents a cause or a consequence of severe seizures.1,5,8,9,11–13,20,25 Despite this, the correlation between progression of the disease and severity of the epileptic events seems to indicate that FHN is the origin of the epileptic activity. This idea is supported by several facts. First, there is convincing experimental evidence in laboratory cats that progressive kindling of the hippocampus causes autonomic, motor and behavioural signs virtually identical to the ones suffered by FHN patients, finally resulting in generalised seizures (Table 5).31–33 Second, in cats with naturally occurring FHN, the focal seizures often progress into generalised seizures, as reported for cases 1, 2 and 4. In some cases, the focal phase may be too short to be noticed before generalisation into a tonic-clonic seizure. This worsening of the clinical condition in naturally occurring FHN matches the progression reported in experimental settings. Lastly, although some authors report the typical FHN MRI changes as post-ictal, 8 this is debatable as post-ictal MRI changes have not been described in cats, as opposed to dogs and humans.34–37 In the light of this, the possibility that FHN is a consequence of intense seizure activity is less likely. Nonetheless, more research investigating post-ictal MRI changes in epileptic cats is needed to further evaluate this possibility.
Previously proposed clinical staging system for experimentally induced feline hippocampal and piriform lobe necrosis seizures compared with the presented cases

In human medicine, the most typical manifestation of LE and secondary TLE is represented by focal seizures consisting of sensations of fear or rage, oro-alimentary automatisms, mydriasis, hypersalivation, hyperventilation and heart rate changes.38,39 Human LE is thought to be mediated by VGKC complex antibodies; 23 the latter are also associated with facial or faciobrachial dystonic seizures,21,22 which resemble the typical clinical presentation of FHN. Pakozdy et al found concentrations of VGKC complex antibodies greater than the human RIs in 36% of a group of cats with clinical signs compatible with FHN. 20 Moreover, autoantibodies against the ‘deleted in colorectal cancer’ protein were found in a feline patient with clinical signs and MRI findings compatible with FHN, in the absence of VGKC complex antibodies. 25 These results suggest that even within the possibility of an autoimmune LE causing FHN, different autoantibodies may be involved in the feline population, requiring further investigations in future research.
Typically, in FHN patients undergoing MRI, the hippocampus and the piriform lobes are T2 and FLAIR hyperintense, T1 hypointense and can show contrast enhancement. 15 The lesions can be homogenous, affecting the organ in its entirety, or only focal. 18 Despite the peculiar presentation, a diagnosis can only be postulated based on clinical presentation and/or MRI until pathology is performed (most commonly post mortem). Timing of MRI acquisition in respect to the onset of the clinical signs can also be relevant, as imaging findings are not consistent at different stages of the disease. 9 In our population, except for case 6, advanced neuroimaging was performed soon after seizure onset (median 3 days; range 559 days). In case 6, MRI was performed approximately 18 months after the first seizure and 2 days after acute seizure re-exacerbation. Unfortunately, it is impossible to establish whether imaging performed within the first days after the very first seizures would have revealed more marked changes. Specific three-dimensional volumetric sequences have been used to assess for hippocampal atrophy and asymmetry in feline limbic epilepsy, 40 and can be crucial for their detection if the lesions are subtle; however, altered size or asymmetry was noted in four of our seven cases on standard sequences. There was also no evidence of further structural disease beyond the hippocampal changes and the asymmetry was always thought to be due to asymmetric oedema rather than atrophy.
Peri-ictal urinary dysfunction has rarely been reported in cats suffering with FHN.8,10 In our cases, bladder management was difficult in cases 1, 4 and 5. This is an uncommon finding and, to our knowledge, it has only been reported in a few other cats.8,10 Feline interstitial cystitis has been proposed as the underlying process causing urinary retention in these patients: autonomic dysfunction, hippocampal changes secondary to chronic stress and stress caused by hospitalisation or the disease itself are all possible pathophysiological mechanisms.10,41 In human medicine, epileptic patients can suffer from different post-ictal urinary issues, with the most common one being incontinence (24.3%) and urinary retention being reported by up to 8.7% of epileptic patients.42,43 Urinary dysfunction is also more common in those suffering from focal seizures. 42 Aural urinary urge is reported in patients suffering from TLE,44,45 and an ictal urinary urge epileptogenic zone could be localised to the temporal lobe by invasive subdural EEG. 44 Further research is needed to define the pathophysiology underlying this process in feline patients; however, when treating FHN, the clinical consequences of an interstitial cystitis should be considered as a potential complicating factor.
EEG has been performed inter-ictally in cats with FHN. Although some patients had a normal EEG,2,9 in human medicine ictal scalp EEG is normal in 60% of patients with TLE. 46 In two cats the abnormalities detected were primarily located in the left occipital lobe,9,10 with spread to the same side; Kuwabara et al detected inter-ictal spikes and sharp waves in the temporal–parietal regions of 14 cats with seizure semiology similar to our cases. 47 EEG can also determine whether a patient is ictal, and it has been used to detect non-convulsive status epilepticus and successfully guide treatment in a cat. 30 In human medicine, patients with TLE represent nearly 70% of all epilepsy patients treated with tailored brain resection, 48 and 80% of those patients with TLE show seizure freedom for at least 2 years postoperatively. 49 If EEG is performed and interpreted more confidently and reliably in cats in the future, similar surgical techniques could also be developed in veterinary medicine.
To our knowledge, there are only a few reports of abnormal CSF in cats with FHN: in one case, CSF protein and nucleated cell count were mildly to moderately increased with mixed pleocytosis. RT-PCR did not detect feline immunodeficiency virus, feline leukaemia virus FeCoV or Toxoplasma gondii in CSF, and only showed a very weak positivity for parvovirus. The latter finding was considered secondary to sample contamination. 50 In a cat with histologically confirmed piriform lobe oligodendroglioma, CSF protein was mildly increased, 19 while in another feline patient mild pleocytosis with mononuclear predominance was detected. 2 In our patients, cisternal CSF analysis did not show any significant anomalies, similarly to other reports.1,2,9,14,15 The absence of pleocytosis or other significant CSF abnormalities does not rule out several infectious and non-infectious diseases of the central nervous system; 51 therefore, in patients with FHN, CSF analysis should always be correlated with neuroimaging and clinical findings.
Treatment of FHN is frequently challenging and this often leads to euthanasia.1,2,4,9,14,15 Affected cats should be treated promptly in the attempt of limiting the degree of hippocampal sclerosis, which represents a crucial element for pharmacoresistance.4,18 According to some reports,3,10,20,21 antiepileptic drugs (AEDs) seem to result in reduced seizure frequency and/or severity if associated with corticosteroids. Medications such as dexamethasone and prednisolone act as anti-inflammatory, anti-oedemigenous and immunosuppressive agents, and may be beneficial regardless of whether immune-mediated inflammation or neoplasia is suspected. However, more studies are necessary to define whether corticosteroids are truly advantageous in the treatment of FHN. In our cases, treatment with dexamethasone was administered to all seven patients and therefore no control individuals receiving AEDs only were available. The majority of the patients experienced a significant improvement. In case 2, it is unclear whether treatment should have been started earlier or at higher doses to limit such an extensive degree of necrosis. Cases 5 and 7 were refractory to treatment and this was likely due to the neoplastic nature of their condition.
Conclusions
FHN is a newly described disease characterised by acute focal seizures resembling human autoimmune LE and TLE. The aetiology is unclear; growing evidence supports an autoimmune nature in cats as well, although disruption of hippocampal architecture secondary to brain neoplasia has also been found. Diagnosis is currently achieved clinically and with brain MRI. The use of EEG and the interpretation of VGKC/LGI1 autoantibodies detection are currently being investigated and may allow a more confident ante-mortem diagnosis in the future. Based on the literature and our clinical experience, treatment should consist of AEDs in conjunction with immunosuppressive doses of corticosteroids. Our study contributes to the existing literature by reporting seven further cases of FHN and their diagnostic and therapeutic plan, by reviewing the available research and by proposing the hippocampus and piriform lobe as neuroanatomical structures that, if damaged, can lead to distinct focal seizures in cats, regardless of the underlying aetiology. In fact, we describe two cases with MRI findings indicative of FHN and post mortem suggesting neoplasia, meaning that even with specific imaging characteristics, different aetiologies should be considered. Pyrexia and peri-ictal urinary dysfunction are also important findings and potential complicating factors that should be accounted for when managing FHN.
Footnotes
Conflict of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognised high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee was therefore not specifically required for publication in JFMS.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work for the procedure(s) undertaken. No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.