
Abstract
Objectives
The aim of this study was to retrospectively evaluate the signalment, treatment, surgical technique and outcomes for feline symblepharon.
Methods
A retrospective medical record review and standardized grading of clinical descriptions and photographs was undertaken.
Results
Forty kittens (54 eyes) aged 3–46 weeks had symblepharon of five types in various combinations: eyelid deformation (24 kittens; 32 eyes); ankyloblepharon (four kittens; four eyes); conjunctiva-to-conjunctiva (11 kittens; 12 eyes); third eyelid-to-conjunctiva (24 kittens; 29 eyes); and corneoconjunctival adhesions (14 kittens; 16 eyes). At initial presentation, 23 (43%) eyes were affected by one type of symblepharon, 25 (46%) eyes by two types and six (11%) eyes by three types; 11 (20%) corneas were ulcerated. Twenty-four (44%) eyes of 18 (45%) kittens were managed medically. Surgery was performed under general anesthesia/sedation (30 occasions) or topical anesthesia (21 occasions) on 30 (56%) eyes of 22 kittens; 12 eyes (40%) underwent multiple surgeries. Four techniques were commonly employed: separation of conjunctival-to-conjunctival adhesions ± eyelid margins (14 eyes); resection of third eyelid adhesions ± temporary tacking of the third eyelid (modified Arlt’s pterygium technique; 18 eyes); en bloc resection of the third eyelid (two eyes); and separation of corneoconjunctival adhesions (14 eyes). Median duration of follow-up was 55 days (range 1–1051). Median symblepharon grade in kittens treated surgically improved for all types except corneoconjunctival symblepharon. Median symblepharon grade in kittens receiving medical management remained the same or improved. Corneoconjunctival symblepharon opacity decreased for eyes treated surgically but increased for eyes treated medically. Three eyes were enucleated due to complications of corneoconjunctival symblepharon. At final presentation, symblepharon persisted in 46 (85%) eyes; however, menace response was evident in 13/16 eyes and dazzle reflex in 23/23 eyes.
Conclusions and relevance
Symblepharon is a heterogeneous group of conditions with diverse anatomic involvement, clinical appearance and impact, optimal treatment and prognosis for vision.
Introduction
Symblepharon is the result of adhesions between the conjunctiva and cornea, or between and among various conjunctival surfaces. These adhesions occur following ulceration of the epithelial surfaces of these tissues and exposure of the subepithelial collagenous connective tissue. The clinical significance of symblepharon varies widely, depending on its extent and the tissues involved. However, it can be blinding or at least reduce vision through narrowing of the palpebral fissure, fixation of the third eyelid over the cornea and/or corneal conjunctivalization, and can disturb the normal distribution and retention of tears as a result of cicatrization of surface tissues – especially the third eyelid, conjunctival fornices and lacrimal puncta. Although any cause of conjunctival ulceration with or without corneal ulceration can cause symblepharon, infection with feline herpesvirus type 1 is a recognized and likely common cause in domestic cats. 1
Despite symblepharon being seen commonly in feline practice, relatively few articles describe the affected population, the extent and nature of symblepharon, medical and surgical treatments, and therapeutic outcome. Specifically, searches of PubMed and CAB Abstracts on 7 September 2022 using the terms ‘symblepharon’ along with ‘feline’ or ‘cat’ found just seven articles published between 2001 and 2021. Of these, two were review articles,1,2 and five were case reports or case series,3–7 collectively describing just 20 cats. Therefore, the present study was designed to retrospectively evaluate the signalment, medical treatment, surgical technique and outcome for kittens with symblepharon at a single institution over 20 years.
Materials and methods
Kittens with a clinical diagnosis of symblepharon between 1 January 2002 and 31 May 2022 were identified through a digital search of electronic medical records from the University of California Davis Veterinary Medical Teaching Hospital. The search term used was ‘symbl*’, so as to capture misspelled terms. Each identified record was individually reviewed to ensure all entry criteria were met, namely that (1) a clinical diagnosis of symblepharon had been made; (2) all affected kittens were ⩽1 year of age at the time of initial diagnosis; and (3) all kittens were examined at least twice within the study period by a board-certified veterinary ophthalmologist or resident in training. Eyes with concurrent congenital anomalies or ophthalmic diseases other than keratoconjunctivitis were excluded. Slit-lamp biomicroscopy was performed on all kittens. Vision and light perception were assessed using the menace response, dazzle reflex, and direct and consensual pupillary light reflexes (PLRs). Data retrieved from the medical records of all kittens meeting the entry criteria included signalment (sex, breed, age and body weight at presentation); ophthalmic examination findings (eye[s] affected, presence of ocular discharge, conjunctival hyperemia and chemosis, and results of the Schirmer tear test [STT] and fluorescein application to the ocular surface); medical treatments instituted; surgical procedures performed; period of follow-up; and final outcome. Many kittens included in this study were enrolled in another study evaluating the treatment of ocular-associated upper respiratory tract infection (Institutional Animal Care and Use Committee protocol #20962), and were enrolled concurrently in the present study.
The type and extent of symblepharon were systematically assessed and graded in a standardized manner through a retrospective review of written clinical descriptions and photographs by two authors (DJM and HS). In the present study, 38/40 kittens had at least one clinical photograph available for review, and 21 kittens had been photographed at every visit. A clinical grading system was developed for symblepharon across five anatomic types: (1) eyelid deformation; (2) eyelid marginal fusion (ankyloblepharon); (3) conjunctival-to-conjunctival adhesions; (4) third eyelid-to-conjunctival adhesions; and (5) corneoconjunctival adhesions. Eyelid deformation was graded as 0 (absent), 1 (a small notch in the eyelid margin), 2 (a broader wave-like distortion of the eyelid) and 3 (cicatricial entropion/ectropion). The extent of other types of symblepharon was graded using a semi-quantitative scale where 0 = absent, 0.5 = 0–10% of the structure affected, 1 = 11–25% of the structure affected, 1.5 = 26–50% of the structure affected, 2 = 51–75% of the structure affected, 2.5 = 76–99% of the structure affected and 3 = 100% of the structure affected. In addition, opacity of corneoconjunctival symblepharon was graded as 0 (translucent; complete intraocular examination possible), 1 (partially translucent; pupil border recognizable) or 2 (opaque; intraocular contents unable to be seen).
Ages were compared between male and female kittens, and STT results were compared between affected and unaffected eyes using the Mann–Whitney rank sum test. For all analyses, P values ⩽0.05 were considered to be statistically significant. All statistical analyses were performed using commercial software (SigmaPlot 13.0).
Results
An automated search of the electronic medical record system returned 114 kittens with a clinical diagnosis of symblepharon between 1 January 2002 and 31 May 2022. Once filtered to ensure they had been examined on at least two occasions by an ophthalmologist or resident in training, and had no concurrent ophthalmic disease, 40 kittens met all inclusion criteria. This study population comprised 20 (50%) males and 19 (48%) females; sex was not recorded for 1 (2%) kitten. Thirty-seven were domestic kittens, one was a Siamese, one was a Maine Coon cross and one was a Siamese cross. At first presentation, the median age of the kittens was 11 weeks (range 3–46; n = 39) and the median body weight was 1.1 kg (range 0.25–5.3; n = 24). The median ages (weeks) of the eight male (range 4–46) and 14 female (range 3–43) kittens were not statistically different (P = 0.177).
At first presentation, 14/40 (35%) kittens had bilateral symblepharon, 16 (40%) had only right eye involvement and 10 (25%) had only left eye involvement. Thus, 54 affected eyes were included in the present study. Symblepharon type and extent varied greatly among eyes; however, in general, five distinct types of adhesions were seen in various combinations throughout the study (Table 1). (1) Eyelid deformation due to adhesions and cicatrization within the palpebral conjunctiva were seen in 32 eyes of 24 kittens and varied in extent and magnitude. Kittens were often affected asymmetrically, sometimes with normal eyelids on one side (Figure 1a). Small wedge-shaped, angular, ‘notch-like’ defects were seen on the upper or lower eyelid, most commonly at the junction of the medial and central thirds of the upper eyelid (Figure 1b). More severe lesions included wave-like deformations involving various proportions of the upper and/or lower eyelids (Figure 1c), or cicatricial entropion or ectropion (Figure 1d). (2) In four eyes of four kittens the adhesions were between the palpebral conjunctiva just inside the eyelid margin, leading to varying degrees of ankyloblepharon (Figure 2a,b). (3) Adhesions between different regions of the palpebral, forniceal and bulbar conjunctiva were seen in 12 eyes of 11 kittens, and varied in extent, leaving variable ‘windows’ through which the cornea could be viewed (Figure 2b,c). In two eyes of two kittens these adhesions presumably also obstructed the nasolacrimal apparatus and tears accumulated between the cornea and the closed eyelids, leading to dramatic distension of the skin overlying the globe (Figure 2d,e). (4) The third eyelid was adherent to the palpebral, forniceal and/or bulbar conjunctiva to varying degrees in 29 eyes of 24 kittens (Figure 3). (5) Adhesions between the bulbar, forniceal or palpebral conjunctiva and the cornea (‘corneal conjunctivalization’) was seen in 16 eyes of 14 kittens, and varied greatly in extent and opacity (Figure 4).
Number of eyes (kittens) affected by symblepharon classified by symblepharon type and extent/opacity grade at first presentation
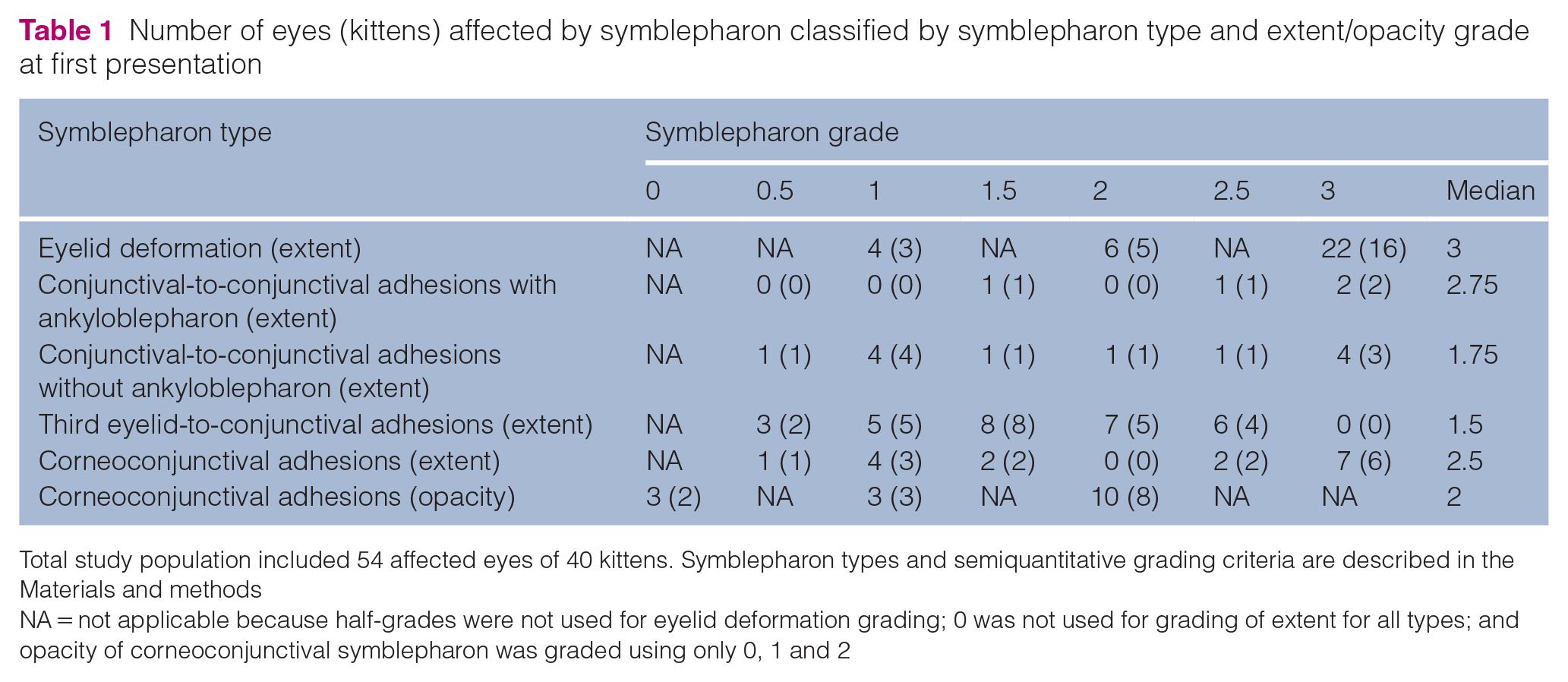
Total study population included 54 affected eyes of 40 kittens. Symblepharon types and semiquantitative grading criteria are described in the Materials and methods
NA = not applicable because half-grades were not used for eyelid deformation grading; 0 was not used for grading of extent for all types; and opacity of corneoconjunctival symblepharon was graded using only 0, 1 and 2

Clinical photographs demonstrating the varying extent of symblepharon-associated eyelid deformation. (a,b) Both eyes of a 10-week-old intact female Siamese cross kitten with an (unaffected) right eye graded as 0 (a) and a small notch defect in the upper eyelid margin at the point most typically seen in the present study and graded as 1/3 (b). (c) Right eye of a 15-week-old intact female domestic shorthair (DSH) kitten. The upper eyelid demonstrated a broader wave-like distortion, graded as 2/3. There was also third eyelid-to-conjunctival symblepharon. (d) Right eye of a 19-week-old intact female DSH kitten. Note the cicatricial ectropion and extensive deformation of the contours of the upper and lower eyelids, graded as 3/3. Grading criteria are described in the Materials and methods

Clinical photographs demonstrating the varying extent of conjunctival-to-conjunctival symblepharon. (a) Left eye of a 21-week-old intact female domestic shorthair (DSH) kitten. Note that the eyelids were completely fused (‘ankyloblepharon’), graded as 3/3, making it impossible to assess for other conjunctival adhesions. (b) Right eye of a 14-week-old intact male Siamese kitten. Note that the eyelid margins were adherent laterally (ankyloblepharon graded as 1.5/3), and the upper and lower palpebral/forniceal conjunctival regions were adherent across all but the smallest area nasally (arrow; graded as 2/3). (c) Left eye of a 9-week-old intact male DSH kitten. Note the upper and lower palpebral/forniceal conjunctival regions were adherent centrally leaving small ‘windows’ of visible cornea nasally and temporally (graded as 1.5/3); however, the eyelid margins were non-adherent (ankyloblepharon graded as 0/3). Dorsal (d) and frontal (e) views of both eyes of a 12-week-old intact male DSH kitten with complete fusion of conjunctiva (graded as 3/3) but not eyelid margins (graded as 0/3) of the right eye, and fusion of all but a tiny window of the conjunctiva laterally (graded as 2.5/3) but no eyelid marginal involvement (ankyloblepharon graded as 0/3) in the left eye. Note too that complete conjunctival fusion of the right eye has led to marked distension of the periocular skin due to retention of tears between the cornea and eyelids (‘pseudobuphthalmos’). Postoperative photographs are provided in Figure 7. Grading criteria are described in the Materials and methods

Clinical photographs demonstrating the varying extent of third eyelid-to-conjunctival symblepharon. (a) Left eye of a 7-week-old intact female Siamese cross kitten. Owing to adhesions to the palpebral conjunctiva, the third eyelid was fixed in position across a small percentage of the medial globe (graded as 1/3). There was also a small notch defect in the upper eyelid at the characteristic point where the third eyelid seems to insert. (b) Right eye of a 13-week-old intact male domestic shorthair (DSH) kitten. Here, the third eyelid was extended and adhered across a greater portion of the globe (graded as 1.5/3). Note there was also a wave-like deformation of the upper eyelid. (c) Left eye of an 8-week-old intact male DSH kitten with third eyelid-to-conjunctival adhesions causing the third eyelid to almost completely obscure the globe (graded as 2.5/3). Note there was also marked wave-like deformation of the eyelids with some ectropion. Grading criteria are described in the Materials and methods

Clinical photographs demonstrating the varying extent and opacity of corneoconjunctival symblepharon (‘corneal conjunctivalization’). (a) Right eye of an 18-week-old intact male domestic longhair kitten. Note that there was complete conjunctivalization of the cornea evident as superficial blood vessels and an altered specular reflection from the ocular surface (graded as 3/3), but that this was partially translucent, allowing visualization of the pupil border (graded as 0/2). There was also a thicker band of more opaque corneoconjunctival symblepharon dorsally, mild wave deformation of the upper eyelid and some third eyelid-to-conjunctival symblepharon. (b) Right eye of a 21-week-old castrated male domestic shorthair (DSH) kitten. The extent of conjunctivalization was graded as 3/3 and opacity was graded as 1/2. (c) Right eye of an 8-week-old intact female DSH kitten. The extent of conjunctivalization was graded as 3/3 and opacity was graded as 2/2. Grading criteria are described in the Materials and methods
At first presentation, 23 (43%) eyes had one type of symblepharon, 25 (46%) eyes had two types and six (11%) eyes had three types.
Other common clinical signs at first presentation were ocular discharge (33 affected eyes; 61%), conjunctival hyperemia (29 eyes; 54%) and chemosis (26 eyes; 48%). Fluorescein staining revealed corneal ulceration in 11 (20%) affected eyes. STTs were not conducted at all visits; however, for all kittens in which this test was conducted, median STT results on the first occasion measured were 9.5 mm/min (range 5–29) in affected eyes (n = 10) and 12 mm/min (range 2–19) in unaffected eyes (n = 6). Median STT results of affected and unaffected eyes at first presentation were not significantly different from one another (P = 0.828). STT results were above the minimum value published for adult cats (⩾9 mm/min)8,9 in 6/10 (60%) affected eyes tested and in 4/6 (67%) unaffected eyes measured.
At first presentation, menace response was reported for 20 (37%) affected eyes and was normal in 11 (55%) eyes tested, absent in eight (40%) eyes tested and slow in one (5%) eye tested. Dazzle reflex was present in all 29 affected eyes in which this test was reported. Direct PLR was reported in 21 (39%) affected eyes and was brisk and complete in 19 (90%) eyes tested and slow and incomplete in two (10%) eyes tested. Consensual PLR when affected eyes were stimulated was reported for 28 (52%) eyes and was brisk and complete in 26 (93%) eyes tested and slow and incomplete in the remaining two (7%) eyes.
All kittens received medical care appropriate for their clinical signs. Typically, this included various combinations of topically applied antibiotics (usually ofloxacin ophthalmic solution) and/or hyaluronate, and orally administered antibiotics (typically doxycycline at 5 mg/kg PO q12h) and/or famciclovir (90 mg/kg PO q12h). Antibiotics and antiviral drugs were typically given for 21 days. If kittens still had clinical signs after 21 days, treatment was continued until 7 days beyond clinical resolution.
Twenty-four eyes of 18 kittens received only medical management (Figure 5). Surgical procedures were performed on 30 (56%) eyes of the remaining 22 kittens on 51 occasions. (Each eye was considered as a separate surgical ‘occasion’.) Twelve of these eyes (40%) underwent multiple surgical corrections. Surgery was always delayed until active conjunctivitis was medically controlled. Symblepharon correction was performed under general anesthesia or sedation on 30 occasions (16 in conjunction with spay/neuter procedures) or using only topical anesthetic, as reported by Saito, 10 on the remaining 21 occasions. General anesthesia or sedation was preferred for patient immobilization when the adhesions were more major, or when timing permitted the symblepharon repair to be done in conjunction with spaying or neutering. Topical anesthesia achieved with ophthalmic tetracaine or proparacaine solution, and sometimes augmented with lidocaine gel, was used for corneal debridement, placement of a bandage contact lens, or when more minor or frequent procedures were possible due to owner availability, patient compliance and extent of adhesions. Surgical correction was always tailored to the type and extent of symblepharon but typically involved four general approaches (often in various combinations): (1) separation of conjunctival-to-conjunctival adhesions along with separation of the eyelid margins when ankyloblepharon was also present (14 eyes, 11 kittens, 25 occasions; Figures 6–8); (2) resection of adhesions between the palpebral conjunctiva and third eyelid, often with temporary tacking of the third eyelid into the medial canthus using a procedure modified after Arlt’s pterygium technique (18 eyes, 14 kittens, 20 occasions; Figures 6 and 8); 11 (3) en bloc resection of the third eyelid (two eyes, two kittens, two occasions); and (4) gentle separation of corneoconjunctival adhesions using a combination of blunt and sharp dissection (14 eyes, 10 kittens, 24 occasions; Figure 7).

Clinical photographs of the right eye of an intact male domestic shorthair kitten with symblepharon that received only medical management for 2 weeks (orally administered amoxicillin–clavulanate, L-lysine and famciclovir, and topically applied tetracycline–polymyxin ophthalmic ointment). (a) At 9 weeks of age, eyelid deformation was graded as 3/3 and conjunctival-to-conjunctival symblepharon as 2.5/3. (b) Following 2 weeks of medical management, eyelid deformation was graded as 1/3 (note the characteristic notch defect) and conjunctival-to-conjunctival symblepharon as 0 (absent). Grading criteria are described in the Materials and methods

Clinical photographs of the right eye of a spayed female domestic shorthair kitten treated medically and surgically. Medical management included (at various times) topically applied ofloxacin solution, bacitracin–neomycin–polymyxin ointment, hyaluronate gel, prednisolone acetate suspension and orally administered famciclovir. Surgery included extensive conjunctival adhesion resection and a modified Arlt’s pterygium technique at 24 and 39 weeks of age, and minor resections under topical anesthesia at 43 weeks of age. Not shown in these figures are the results of two subsequent minor resections under topical anesthesia at 44 and 47 weeks of age. (a) Intraoperative photograph at the first surgery (24 weeks of age). Eyelid deformation was graded as 2/3, conjunctival-to-conjunctival symblepharon as 1/3 and third eyelid-to-conjunctival symblepharon as 2.5/3. Note that conjunctival-to-conjunctival adhesion left a small ‘window’ through which the cornea could be visualized. (b) Immediately following the first surgery. Note that the third eyelid is fixed at the medial canthus by a 3-0 nylon purse-string-type suture. (c) Approximately 8 weeks after the first surgery. Eyelid deformation was graded as 2/3, conjunctival-to-conjunctival symblepharon as 0.5/3, third eyelid-to-conjunctival symblepharon as 0.5/3, and corneoconjunctival symblepharon as 3/3 (extent) and 1/3 (opacity). (d) Twenty weeks after the first surgery (5 weeks after the second surgery and 1 week after the third surgery). Eyelid deformation was graded as 2/3, conjunctival-to-conjunctival symblepharon as 0.5/3, third eyelid-to-conjunctival symblepharon as 0.5/3 and corneoconjunctival symblepharon as 3/3 (extent) and 0/3 (opacity). Grading criteria are described in the Materials and methods

Clinical photographs of the right eye of the same intact male domestic shorthair kitten shown in Figure 2(d,e) in which complete fusion of the conjunctiva caused marked distension of the periocular skin due to retention of tears between the cornea and eyelids. (a) At 12 weeks of age, immediately following opening of the conjunctival-to-conjunctival adhesions to release accumulated tears and reduce pseudobuphthalmos. Some corneoconjunctival adhesions were also resected. Four weeks later, further separation of third eyelid-to-conjunctival and corneoconjunctival adhesions was performed. (b) At 19 weeks of age, about 6 weeks after the first (2 weeks after the second) surgery, a focal region of granulation tissue was present on the corneal surface. (c) At 24 weeks of age, 11 weeks after the first (7 weeks after the second) surgery, the eyelids remain separated, but there was notable deformation of the upper eyelid and conjunctivalization of the cornea. (d) At 33 weeks of age, 20 weeks after the first (16 weeks after the second) surgery, the upper eyelid remained deformed; however, the extent and opacity of the corneoconjunctival symblepharon were reduced

Clinical photographs of an intact male Siamese kitten with ankyloblepharon and conjunctival-to-conjunctival symblepharon of the right eye. (a) Both eyes at 14 weeks of age. For the right eye, eyelid deformation was graded as 3/3, eyelid margin-to-margin adhesions as 1.5/3 and conjunctival-to-conjunctival symblepharon as 3/3. (b) Immediate postoperative appearance of the right eye following separation of the eyelid margins and third eyelid fixation using the modified Arlt’s pterygium technique. (c,d) Appearance 12 days postoperatively, immediately before suture removal. Grading criteria are described in the Materials and methods
One kitten also had a bilateral superficial keratectomy (once) and multiple corneal debridements, often with contact lens placement. Another kitten had a combined wedge resection and Hotz–Celsus procedure, 12 performed for unilateral entropion of the lower eyelid.
Regardless of surgical technique or anesthetic protocol, all affected eyes were routinely prepared with betadine solution diluted 1:50 in sterile saline. Surgery was typically completed using magnifying loupes, Colibri or Bishop-Harmon forceps, and Westcott or Vannas scissors. Eyelid margins were typically separated using a #15 Bard Parker or #64 Beaver scalpel blade. Arlt-type fixation of the third eyelid was typically completed using 3-0 nylon placed in a modified purse-string pattern (Figure 9). The suture was removed approximately 10 days postoperatively. Postoperative medications typically included topical application of an antibiotic or antibiotic–steroid ointment 2–4 times daily. Ophthalmic ointments were generally preferred over solutions or suspensions, to reduce wound healing and adhesion formation. Additionally, owners were instructed to forcibly open and close the eyelids frequently for the first few days following surgery in an attempt to limit the formation of postoperative adhesions.
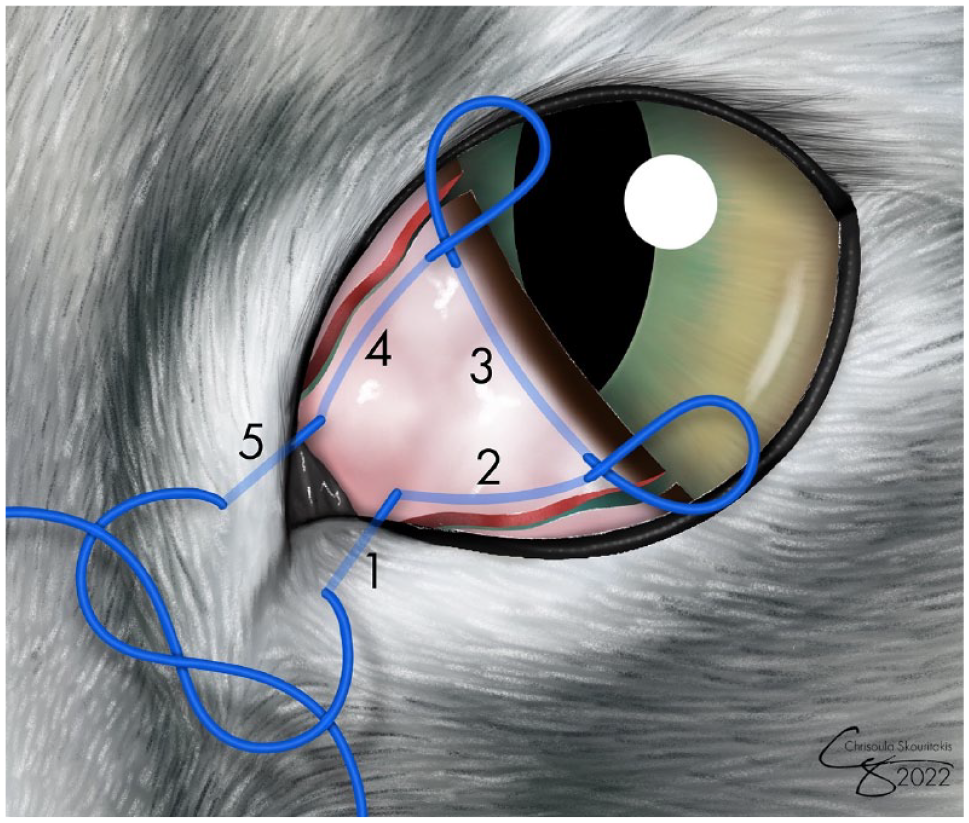
Modified Arlt’s pterygium technique. First, all adhesions between the dorsal and ventral edges of the third eyelid and the palpebral, forniceal and bulbar conjunctiva, as well as adhesions between the third eyelid and cornea, were gently resected to recreate a freely mobile, fan-shaped third eyelid. A 3-0 nylon suture in a purse-string pattern was then placed so as to retract the third eyelid into the medial canthus and restrain it there. (1) The purse string was initiated at the ventral aspect of the medial canthus by passing the suture from the skin surface into the conjunctival fornix. (2) A long subconjunctival pass was then made up the freshly cut ventral edge of the third eyelid, emerging near its leading edge. Two more long subconjunctival bites were then passed (3) across the leading edge of the third eyelid from ventral to dorsal and then (4) down the freshly cut dorsal edge of the third eyelid. (5) Finally, the suture was passed from the dorsomedial conjunctival fornix out through the skin just dorsal to the medial canthus, and the purse string was tightened to retract the third eyelid into the medial orbit and was tied. Preoperative preparation, perioperative medications and suture removal are described in the Results
Enucleation was recommended at the final visit or performed for three (6%) eyes: one right eye and two left eyes. One eye was enucleated due to rupture at the time of first attempted resection of corneoconjunctival adhesions. One eye was enucleated following multiple surgeries for eyelid-to-eyelid and extensive corneoconjunctival symblepharon, during which corneal thinning was suspected and the risk of rupture considered too great. This eye subsequently underwent histologic examination which revealed diffuse absence of corneal epithelium and replacement by loose connective tissue and small-caliber blood vessels reminiscent of conjunctival stroma but without conjunctival epithelium (Figure 10). The superficial to mid-corneal stroma was infiltrated by small blood vessels and few fibroblasts. The mid-to-deep corneal stroma subjectively lacked clefting, suggesting corneal edema. Enucleation was recommended for the third eye due to corneal thinning and marked keratoglobus with secondary ulceration, keratomalacia and staphyloma formation following resection of corneoconjunctival adhesions (Figure 11).

Photomicrograph of the left cornea of an approximately 1-year-old spayed female domestic shorthair kitten enucleated following attempted separation of corneoconjunctival adhesions. The corneal epithelium was diffusely absent and replaced by loose, hypocellular fibrous connective tissue with a few congested blood vessels and hemorrhage. Bar = 100 µm. (Inset) Blood vessels and hemorrhages were present within the superficial stroma. Smaller congested capillaries and a few fibroblasts extended into the mid-corneal stroma. Bar = 100 µm

Clinical photographs of the left eye of an intact male domestic shorthair kitten that developed marked corneal thinning and keratoglobus following symblepharon surgery. This is the same cat as shown in Figure 2(c). (a) At 9 weeks of age. Immediate postoperative appearance after conjunctival-to-conjunctival symblepharon was separated. (b,c) At 11 weeks of age. Lateral (b) and frontal (c) views 14 days postoperatively. Note the marked keratoglobus. (d,e) At 14 weeks of age. Lateral (d) and frontal (e) views 38 days postoperatively. Note the marked keratoglobus, keratomalacia and stromal keratitis. Enucleation was recommended
Median duration of follow-up from first presentation was 55 days (range 1–1051); 29 kittens (73%) were followed for at least 1 month, 11 (26%) for at least 4 months and 10 (24%) for at least 6 months. At the final examination, symblepharon was considered to still be present in 46 (85%) eyes originally affected. Considering only the 14 kittens affected bilaterally at study entry, 12 (86%) remained bilaterally affected at the end of the study. Median grade of symblepharon extent in kittens receiving medical and surgical management tended to improve during the study period for all types except corneoconjunctival symblepharon, which increased (Figure 12a). Median grade of symblepharon extent in kittens receiving only medical management tended to remain the same or improve during the study period (Figure 12b). Median grade for the opacity of corneoconjunctival symblepharon tended to decrease for eyes treated surgically and increase for eyes treated medically.
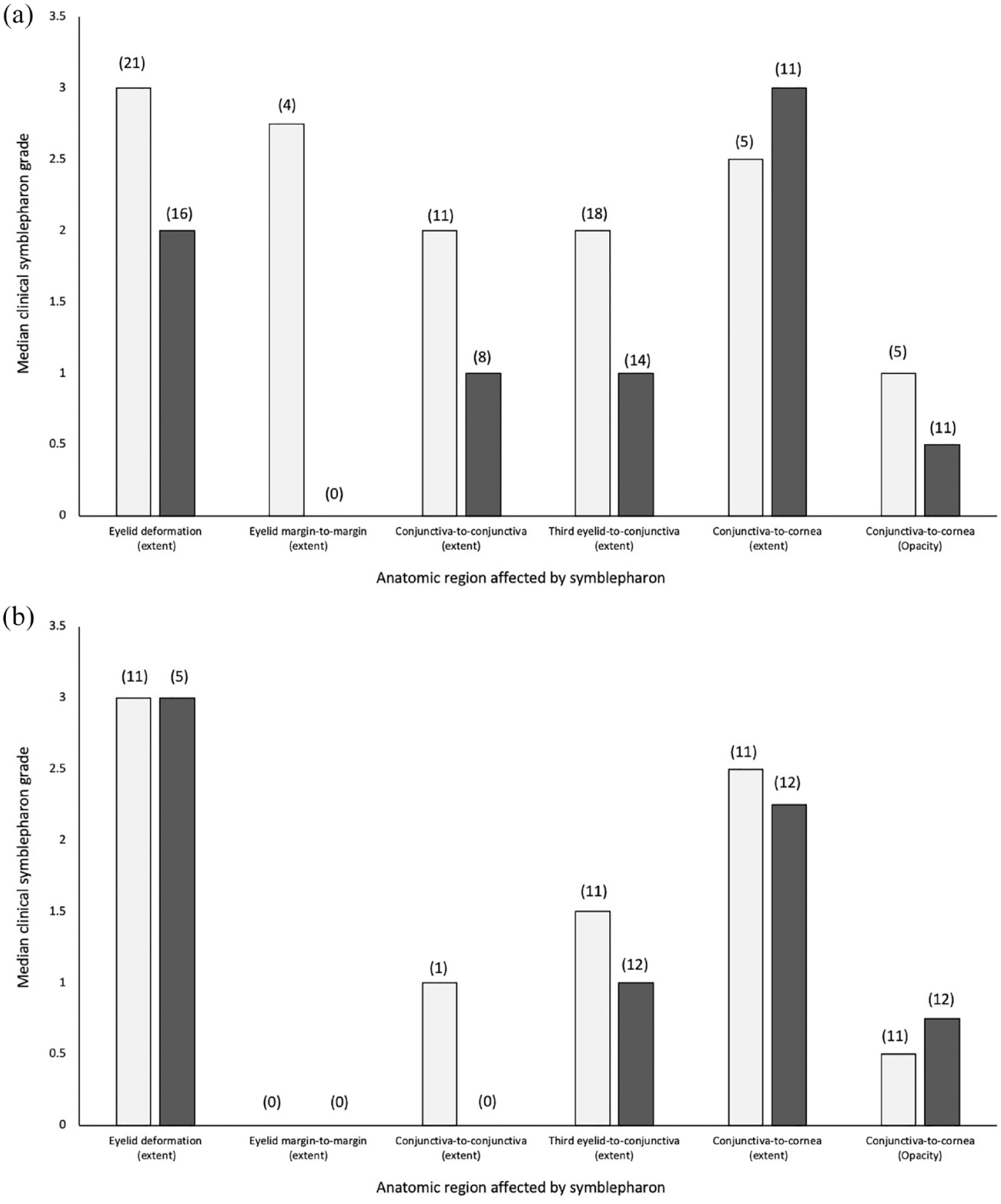
Median clinical symblepharon grades for five types of symblepharon in 54 eyes of 40 kittens treated (a) medically and surgically or (b) medically only. Gray bars represent data from the initial examination; black bars represent data from the final examination. Median period between the two examinations was 51 days (range 1–1051). Numbers in parentheses above each bar represent the number of affected eyes. Grading criteria are described in the Materials and methods
Considering the entire study period, STTs were performed on 19 occasions in 10 symblepharon-affected eyes of eight kittens (Table 2). Assessing all STT results recorded throughout the study, the median STT results for affected eyes (10 mm/min [range 5–29]) were not statistically different (P = 0.532) from those for unaffected eyes (11 mm/min [range 2–19]). Where kittens were unilaterally affected and STTs were performed bilaterally, the magnitude of the difference in STT results between the affected and unaffected eyes was calculated (12 eyes of six kittens on 14 occasions). The results were higher in the affected than in the unaffected eyes on nine occasions, and the median difference in STT results between these eyes was 7 mm/min (range 1–15). Results were lower in the affected eyes than in the unaffected eyes on three occasions, and the median difference in STT results between these eyes was 10 mm/min (range 9–12). The results were the same in affected and unaffected eyes on two occasions. Serial STTs were conducted in six affected eyes of five kittens on 16 occasions (Table 2; kittens 2, 3, 4, 5 and 6). Of these five kittens, one had STT performed prior to and periodically for 13 weeks following unilateral third eyelid removal. Relative to the one preoperative measurement, this kitten’s STT results in the surgically treated eye were unchanged or increased on the three postoperative measurements (Table 2; kitten 6).
Results of Schirmer tear testing (STT) performed on 19 occasions in 10 symblepharon-affected eyes and six unaffected eyes of eight kittens
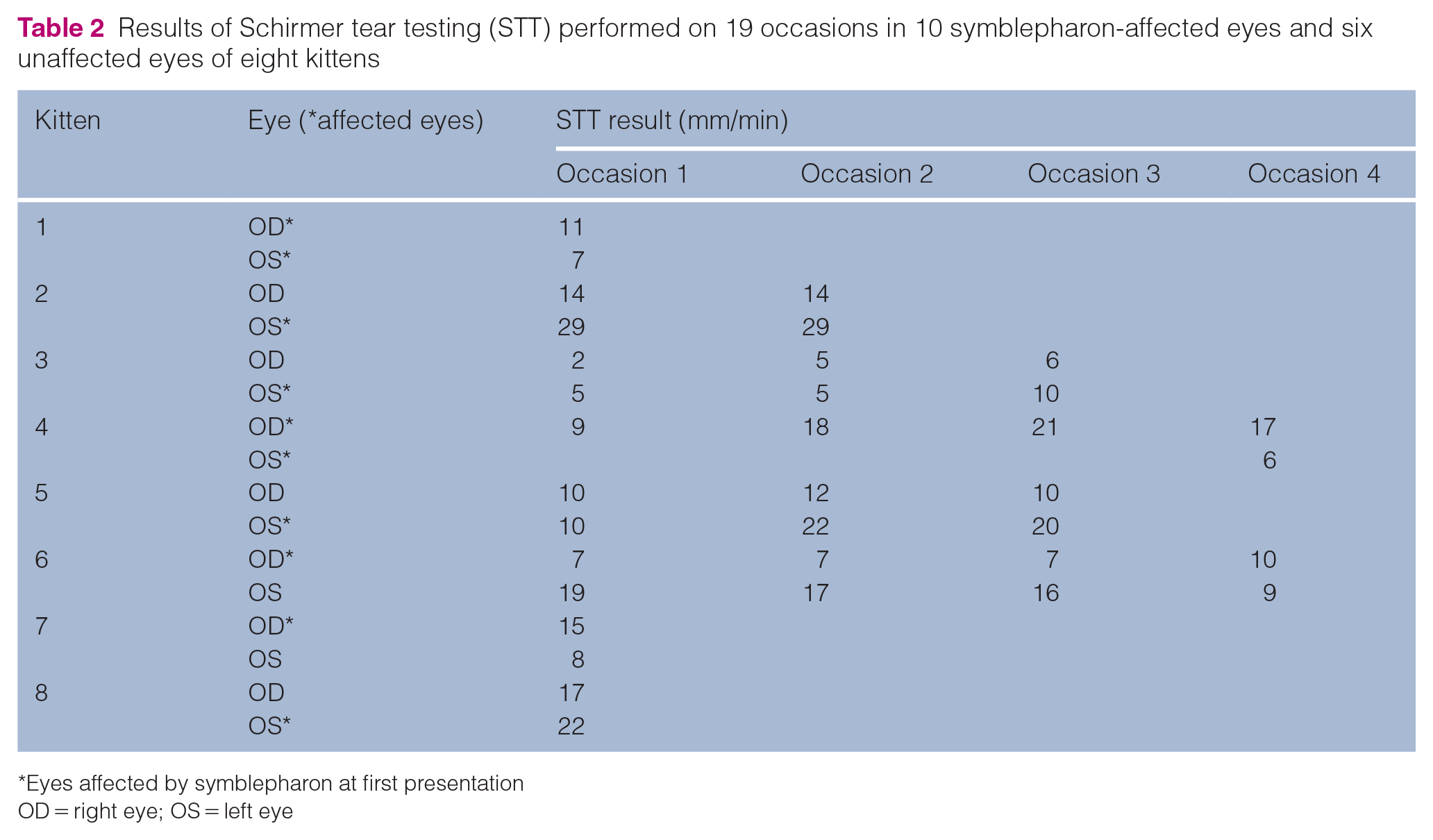
Eyes affected by symblepharon at first presentation
OD = right eye; OS = left eye
At final presentation, menace response was reported for 16 (35%) affected eyes and was normal in 11 (69%), absent in three (19%) and reduced in two (13%) of these 16 eyes. Dazzle reflex was present in all 23 affected eyes in which this test was reported. Direct PLR was reported in 23 (50%) affected eyes and was brisk and complete in 19 (83%) and slow and incomplete in four (17%) of these 23 eyes. Consensual PLR when affected eyes were stimulated was reported for 21 (46%) eyes and was brisk and complete in 17 (81%) and slow and incomplete in four (19%) of these 21 eyes.
Discussion
Peer-reviewed articles published in the English language and regarding symblepharon describe just 20 cats.1–7 Therefore, the present study represents the most detailed report of feline symblepharon to date. Although descriptive in nature, it does permit some observations and recommendations regarding this condition. Notably, we propose that symblepharon does not represent a single diagnosis but rather a heterogenous group of conditions, each with presumably similar etiology and pathogenesis but diverse anatomic involvement, clinical appearance and impact, optimal treatment, and prognosis for vision and likely comfort. Considering these criteria, our experience suggests that symblepharon should be considered as one of five types: (1) eyelid deformation; (2) conjunctiva-to-conjunctiva with ankyloblepharon; (3) conjunctiva-to-conjunctiva without ankyloblepharon; (4) third eyelid-to-conjunctiva; and (5) corneoconjunctival adhesions. Consideration in this manner facilitates decision-making regarding treatment and prognosis; however, this becomes more complex when an eye is affected by more than one type of symblepharon, which is common (57% of eyes in the present study).
Eyelid deformation was the most commonly seen form of symblepharon in the present study (59% of eyes) and was often marked, leading to entropion or ectropion. The most minor form was often overlooked at the initial examination but noted when clinical photographs were reviewed for grading. This was a small and apparently clinically insignificant notch in the upper eyelid. Interestingly, the position of this notch was highly conserved, occurring at the junction of the medial and central third of the upper eyelid. Although it is not known why symblepharon or cicatrization might have consistently occurred here, this typically corresponded to the point of insertion of the superior end of the free margin of the third eyelid. This defect was not specifically addressed therapeutically. Medical management of keratoconjunctivitis led to a reduction in the number of eyes affected by, but not the median extent of, eyelid deformation. Only one eye underwent surgery specifically directed at correction of eyelid deformation (combined Hotz–Celsus and wedge resection for entropion). However, surgical correction of other forms of entropion led to a simultaneous reduction in median extent and number of eyes affected by eyelid deformation.
Adhesions of the third eyelid to other regions of the conjunctiva formed the second most commonly observed form of symblepharon, seen in 54% of eyes. Like conjunctival adhesions elsewhere, these could be markedly vision-impairing and sometimes blinding, requiring surgical correction. Indeed, medical treatment tended to lead to an increase in the number of eyes affected with this form of symblepharon, albeit with a marginal decrease in median extent. By contrast, surgical treatment led to a reduction in the number of affected eyes and median extent grade. Attempts to save the third eyelid led us to modify a surgical technique developed by Arlt for pterygium surgery in humans. 11 While this successfully reduced the extent of corneal coverage by the third eyelid, sometimes notable portions of the cornea remained covered and – in two eyes – the third eyelid was subsequently removed. While third eyelid resection is contraindicated in dogs,13,14 the effects of this procedure on the ocular surface have not been reported in cats, to our knowledge. As a result, we began recording STT results before and after this procedure. In the one cat for which these data were available in the present study, multiple postoperative STT results were unchanged or increased relative to preoperative measurements. Apart from the relative lack of data presented here, this should be interpreted with caution for several additional reasons. First, normal STT values for kittens have not been established and it is possible that the increase we report represents maturation rather than surgical impact. Second, it is possible that surgical manipulations and/or symblepharon itself also affected tear outflow through the nasolacrimal system. Finally, work by Saito et al in the dog13,14 has revealed that some of the effects of third eyelid removal are evident only through electron microscopic assessment of the corneal surface, which was not done here.
Corneoconjunctival symblepharon was seen in 30% of eyes and varied greatly in extent and the degree of corneal opacity it caused. When treated medically, the number of affected eyes and the median degree of opacity increased, while the median extent of conjunctivalization decreased. When treated surgically, the number of affected eyes more than doubled and median extent worsened; however, median opacity decreased. A publication describing 11 cats with corneoconjunctival symblepharon reported that surgical resection was performed in six; however, the remaining five required exenteration. 6 In the present study, all three eyes requiring enucleation were due to complications of corneoconjunctival symblepharon or surgery intended to reduce it. Collectively, the prior report and our data reflect the difficulty in treating this form of symblepharon. This may reflect a loss of corneal stem cells as a critical and irreversible factor in the pathogenesis of this condition. 2 Corneal stem cells located at the corneoscleral limbus are not only vital progenitor cells for corneal epithelial repair, but also form a critical barrier to conjunctivalization of the cornea. Ablation of these cells in diseases such as Stevens–Johnson syndrome 15 and pterygium 16 permit corneal conjunctivalization similar to that noted in the present study, and are presumed to be involved in symblepharon formation in cats. Given the possible involvement of limbal stem cell deficiency in symblepharon formation, 2 surgical treatments such as the ‘simple limbal epithelial transplantation’ procedure described in humans may also be beneficial in feline patients.17,18
Adhesions between conjunctival regions other than the third eyelid were seen in 29% of eyes and caused ankyloblepharon in 7% of these. They varied greatly in extent and anatomic region, and could often be relatively easily surgically separated if there was no corneoconjunctival involvement. Postoperative recurrence was variable. The application of a combined antibiotic–corticosteroid ointment, as well as instructions for the owners to forcibly open and close the eyelids frequently for the first few days following surgery, was done with some of the cats reported here, in an attempt to limit the formation of new postoperative adhesions, and should be studied further.
Although it was one of the less common forms of symblepharon, the type causing ankyloblepharon warrants special mention. These adhesions varied in extent from clinically insignificant to those involving the entire length of the upper and lower eyelids. More extensive adhesions were blinding and, in two eyes in which the nasolacrimal drainage apparatus was presumably simultaneously blocked, led to disfigurement and likely uncomfortable distension of the subpalpebral space with tears. This syndrome produces the appearance of buphthalmos (globe distension due to glaucoma), and can be likened to pseudobuphthalmos in snakes. Recognition of this syndrome is critical since (unlike buphthalmos) pseudobuphthalmos is not vision- or globe-threatening, and affected eyes should not be enucleated. Apart from the obvious difference that the eyelids are fused closed in this condition, whereas they are open with buphthalmos, gentle palpation of the eyelid skin overlying the distension reveals a soft, fluctuant, fluid-filled space with a globe beneath it in this form of symblepharon, rather than a turgid, typically painful globe in buphthalmos. It is also interesting to compare this form of symblepharon with ophthalmia neonatorum of perinatal kittens, which experience delayed opening of physiologic ankyloblepharon. Why the fluid filling the subpalpebral space in symblepharon-associated pseudobuphthalmos in the two cats presented here was completely clear and did not become apparently altered by overgrowth of ocular surface flora or pathogens and infiltration by inflammatory cells, as occurs with ophthalmia neonatorum, is unknown. Surgical correction of ankyloblepharon is recommended as, in this series, it was relatively straightforward and carried an excellent prognosis provided that there were not simultaneous corneoconjunctival adhesions.
Conclusions
By classifying symblepharon types, we were able to identify some forms of symblepharon that were more readily amenable to surgical treatment (conjunctival-to-conjunctival adhesions with or without ankyloblepharon) than others (corneoconjunctival adhesions). Additionally, surgical procedures for ankyloblepharon and conjunctival-to-conjunctival adhesions were relatively simple when done under general anesthesia. Careful identification of these cases could therefore permit surgical care to be completed by a generalist or shelter veterinarian at the time of neutering. In the present study, we also describe two novel surgical techniques for kittens with third eyelid-to-conjunctival adhesions (the modified Arlt technique for pterygium and en bloc resection of the third eyelid). These produced good outcomes for kittens in this study but warrant further assessment of long-term effects on the tear film and ocular surface. Equally importantly, this study reveals that appropriate medical treatment for keratoconjunctivitis can reduce the severity and extent of many forms of symblepharon during this dynamic phase when adhesions are still forming and not yet stable. In the present study, medical management typically included systemically administered famciclovir and doxycycline, as well as topically applied antibiotics and hyaluronate. Finally, this study reveals that symblepharon in kittens does not represent one homogenous diagnosis, but rather manifests as a heterogenous group of conditions with diverse anatomic involvement, clinical appearance and impact, optimal treatment, and prognosis for vision and comfort.
Footnotes
Acknowledgements
The authors thank the Orphan Kitten Project and Yolo County Society for the Prevention of Cruelty to Animals, as well as others fostering and caring for these kittens; staff at the UC Davis Community Surgery and Ophthalmology Services for their collaborative care of kittens undergoing surgical procedures; and Chrisoula Toupadakis Skouritakis PhD for expert assistance with figure preparation.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
This work was financially supported by The Center for Companion Animal Health, School of Veterinary Medicine, UC Davis, Maddie’s Fund and the Orphan Kitten Club.
Ethical approval
The work described in this manuscript describes the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.