
Abstract
Objectives
The aim of this study was to collect clinical information from owners of cats with hypersomatotropism (HS) distributed worldwide, assessing the impact of HS and its treatments on cats’ quality of life (QoL) and survival time.
Methods
A survey focused on clinical presentation, diagnostic procedures, treatments, cats’ QoL and disease progression was distributed worldwide to owners of cats with HS. The owner’s perception of the cats’ QoL before and after or during treatment was defined using a score ranging from 1 (poor) to 5 (excellent). Improvement following treatment (IFT) was quantified using a score ranging from 1 (absent) to 5 (obvious). Different treatment groups, including at least five cases, were compared.
Results
A total of 127 cats were included from at least 11 different countries. Among these, 120 (95%) were diabetic and 7 (5%) were not. Out of 120 diabetic cats, 55 (46%) were treated with insulin as a single treatment (INS). Other treatments were not mentioned to owners in 35/120 (29%) cases. The median QoL score at diagnosis was 2 (range 1–5) and improved after treatment in all groups. Cabergoline (4; range 1–5), radiotherapy (4; range 2–5) and hypophysectomy (5; range 4–5) showed better median IFT scores compared with INS (3; range 1–5) (P = 0.046, P <0.002 and P <0.0001, respectively). Hypophysectomy IFT proved superior to cabergoline (P = 0.047) and was equal to radiotherapy IFT (P = 0.32). No difference was found between cabergoline and radiotherapy IFT (P = 0.99). The median survival time (MST) was 24 months (range 0–75 months). Cats treated with INS showed shorter MST (22 months; range 0–69 months) compared with cats treated with causal treatments combined (36 months; range 3–75 months) (P = 0.04).
Conclusions and relevance
Not all cats with HS will have diabetes mellitus. Causal treatments seem associated with the greatest improvements in perceived cats’ QoL and survival; such treatments should therefore be discussed with owners. Cabergoline could be an effective alternative management option.
Introduction
Hypersomatotropism (HS) is characterised by chronic excess of growth hormone (GH), usually caused in cats by a pituitary somatotroph adenoma or hyperplasia. 1 The term acromegaly defines the clinical syndrome induced by HS. The clinical signs are the consequence of the catabolic and diabetogenic effects of GH, the anabolic effects of insulin-like growth factor-1 (IGF-1) and sometimes the effect of the space-occupying pituitary adenoma. Cats with HS usually develop diabetes mellitus (DM) due to the severe insulin-resistance caused by an excess of GH. With the onset of DM, typical clinical signs of polyuria/polydipsia and polyphagia predominate, and prompt owners to seek veterinary care. Other clinical signs that can be present in cats with HS, sometimes even before the onset of DM, include broad facial features, enlargement of the feet, prognathia inferior, noisy breathing, heart murmur, plantigrade stance and polyphagia.2–4
Until 15 years ago, HS was considered a rare disease in cats, but this perception has progressively changed in recent years. The prevalence of HS among cats with DM has been estimated to be around 25% in the UK and around 18% in Switzerland and the Netherlands.5,6 HS has also recently been described in non-diabetic cats.4,7,8 The increased recognition of HS in cats justifies more research on etiopathogenesis, clinical presentation and potential causal treatments aimed to decrease serum GH and IGF-1 concentrations.
Transsphenoidal hypophysectomy has recently been reported as a consistent and highly effective treatment of HS in large populations of cats with HS and DM.9,10 Radiation therapy has proved effective in reducing both the size of the pituitary adenomas and insulin requirements, but predictable and consistent effects on GH-induced IGF-1 secretion after radiotherapy have not been demonstrated.11,12 Medical therapy with the somatostatin analogue pasireotide improved glycaemic and GH control, but it is extremely expensive.13,14 The dopamine agonist cabergoline is less expensive and widely available, though it does not seem to be uniformly effective.15,16
Discussion of treatment choice is highly relevant, not only for the potential to improve glycaemic control, but also because the lack of definitive treatment will allow disease progression, resulting in clinical deterioration and development of severe complications such as acromegalic cardiomyopathy and severe arthrosis. 17 Despite the rising awareness of feline HS and its treatment, information is lacking about the quality of life (QoL) of affected cats receiving different treatments.
The aim of this observational study was to collect owner-derived clinical and therapeutic information in a large population of cats with HS that are distributed worldwide. Moreover, we aimed to describe the impact of HS on cats’ QoL, and the efficacy of different treatments on QoL and survival time.
Materials and methods
A survey intended for owners of cats with HS was designed by creating a questionnaire comprising 39 questions, which were translated into five different languages: Italian, English, German, Spanish and Portuguese. The questionnaire focused on clinical presentation and diagnosis of HS, recommended and administered treatments, cats’ QoL before and after treatment, follow-up and survival (see file 1 in the supplementary material). The cats’ QoL before treatment, during medical therapy and after radiotherapy or hypophysectomy was defined using a categorical scoring system ranging from 1 (poor) to 5 (excellent). The improvement following treatment (IFT) was quantified using a score ranging from 1 (absent) to 5 (obvious). A free-text field was available at the end of the questionnaire to report additional relevant information about the cat. The questionnaire was imported into Google Forms and the link was distributed worldwide from 1 February 2019 to 30 September 2021 using social media, diabetic cat owners’ online forums and direct contact via email. It was also available via the Vet Professionals website (www.vetprofessionals.com/site/surveys) from 21 January 2021 to 30 September 2021. All the questionnaires submitted were evaluated by two of the investigators (AC, FF) and removed from the analysis if they were considered a duplicate or if the diagnosis of HS was questionable. The diagnosis of HS was deemed reliable if at least one major criterion or two minor criteria were reported (Table 1).
Criteria used to retrospectively confirm the diagnosis of hypersomatotropism in cats included in the study

The diagnosis was confirmed if at least one major criterion or two minor criteria were reported by the owners
GH = growth hormone; IGF-1 = insulin-growth factor-1
Descriptive statistics were performed and results reported as median (range). For a treatment group to be considered for evaluation at least five cats had to have received the same treatment or combination of treatments (eg, insulin therapy plus cabergoline or insulin therapy plus radiotherapy). The median QoL scores before and during/after treatment were compared within treatment groups using the Wilcoxon signed-rank test. The median IFT score was compared between groups receiving different treatments using the Kruskal–Wallis test with Dunn’s multiple comparisons test. Survival curves were generated by the Kaplan–Meier method and compared using the log-rank test. The data were analysed using commercially available software (Microsoft Excel; GraphPad Prism 9).
Results
A total of 150 questionnaires were submitted. Among these, 6/150 (4%) were removed from the analysis because of duplication and 17/150 (11%) because the diagnosis of HS was not sufficiently supported by the owner’s answers. Overall, information regarding 127 cats with HS were collected by 126 different owners (one respondent reported owning two different cats with HS). The total number of answers varied for each question because not all owners answered all questions. The respondents originated from USA (n = 25 [20%]), Italy (n = 24 [19%]), Argentina (n = 15 [12%]), Austria (n = 12 [9.4%]), UK (n = 8 [6.2%]), Switzerland (n = 8 [6.2%]), Canada (n = 8 [6%]), Germany (n = 2 [1.6%]), South Africa (n = 1 [0.8%]), Spain (n = 1 [0.8%]) and the Netherlands (n = 1 [0.8%]). Country of origin was not reported in 22/127 (17%) questionnaires.
Population
The median age at time of diagnosis of HS was 11 years (range 4–17 years). Overall, 89/127 (70%) cats were castrated males, and 38/127 (30%) were female (spayed = 35 [27%]; intact = 3 [2%]). Domestic mixed-breed cats were most represented (n = 76 [59%]), with seven (5%) Siamese, six (4%) Maine Coon, two (1.5%) Ragdoll, two (1.5%) British Shorthair and one each of seven other breeds, while in 28 (22%) cats breed was not reported. Data regarding body weight, lifestyle and type of diet of cats included in the study are reported in file 2 in the supplementary material.
Diagnosis of HS in cats
A complete list of clinical signs is reported in Table 2. Appetite at the time of diagnosis was described as markedly increased, increased, normal and decreased in 70 (55%), 26 (20.5%), 26 (20.5%) and five (4%) cats, respectively. Tests to support diagnosis were serum IGF-1 concentration (117/127 [92%]), advanced diagnostic imaging (CT or MRI scan) (40/127 [31%]) and serum GH concentration (27/127 [21%]). More than one diagnostic test was performed in 52/129 (40%) cats (Table 3). Serum IGF-1 concentrations were not available in 20/117 (16%) cats because owners did not remember or have access to the measured value. Among 97 (82%) cats in which it was available, it was above 1000 ng/ml in 81 (84%), between 800 and 1000 ng/ml in eight (8%), and below 800 ng/ml in eight (8%) cats. A total of 120/127 (94%) cats with HS had concurrent DM, while seven (6%) did not. All cats with concurrent DM were already diabetic at the time of HS diagnosis. Among them, 110/120 (92%) were already receiving insulin treatment. The median daily insulin dose was 14 U (range 2–66) (Figure 1). The median interval between the beginning of insulin treatment and serum IGF-1 measurement was 5 months (range 0.5–60 months).
Clinical signs reported by owners in cats with hypersomatotropism, distinguished based on the presence or absence of concurrent diabetes mellitus (DM)

Data are n (%)
Diagnostic tests performed to confirm hypersomatotropism in 127 cats
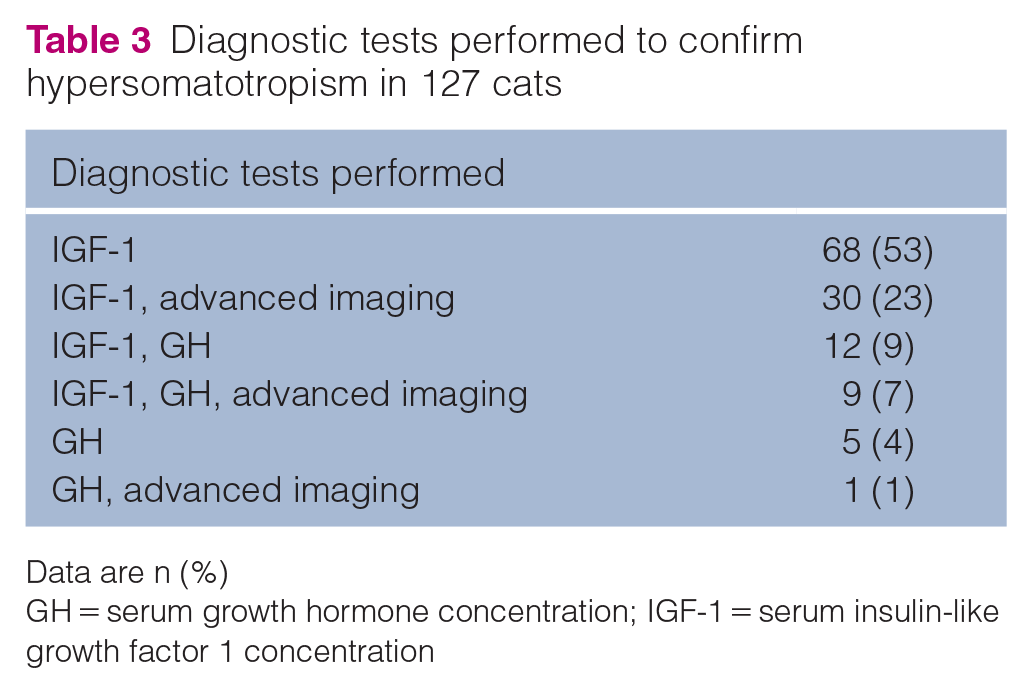
Data are n (%)
GH = serum growth hormone concentration; IGF-1 = serum insulin-like growth factor 1 concentration

Dot plot of daily insulin dosage at the time of diagnosis (left) and maximum daily insulin dosage achieved during the treatment course (right) in 120 cats with hypersomatotropism and diabetes mellitus. The solid line represents the median
Treatment of HS in cats
Treatments recommended at the time of diagnosis in diabetic and non-diabetic cats with HS are detailed in Table 4. Insulin therapy was prescribed in all 120 diabetic cats, but no further treatment was proposed to the owner in 35/120 (29%) cases. Among these 35 cases, seven (20%) owners managed to obtain further treatment for their cats. Treatments performed in all cats are described in Table 5. The median maximum daily insulin dose administered by the owners was 24 U (range 5–230 U), with three cats receiving more than 100 U q24h (Figure 1). Among the 14 cats that underwent hypophysectomy, information regarding insulin requirements after surgery was available for 12. Out of 12 cats, nine (75%) achieved diabetic remission and three (25%) experienced a marked decrease in insulin dose.
Treatments suggested in 127 cats with hypersomatotropism

Data are n (%)
Treatments performed in 127 cats with hypersomatotropism

Data are n (%)
Cats’ QoL
The median QoL score before diagnosis was 2 (range 1–5) and improved after treatment in all treatment groups. The IFT score proved superior in cats that underwent hypophysectomy compared with cats treated with insulin alone and cabergoline-treated cats; but there was no difference to radiotherapy-treated cats. No difference was found between radiotherapy-treated and cabergoline-treated cats, with both groups showing superior IFT scores compared with cats treated with insulin only (Table 6 and Figure 2). Among 120 cats that received insulin during the course of the disease, 30 (25%) experienced at least one episode of symptomatic hypoglycaemia noted by the owner, with 15/30 (50%) experiencing more than one.
Quality of life (QoL) score before and after treatment, and IFT score in different treatment groups

Data are n or median (range) unless otherwise indicated
CAB = insulin and cabergoline; HX = insulin and hypophysectomy; IFT = improvement following treatment; INS = insulin as a single treatment; RT = insulin and radiotherapy

Violin plot of IFT scores in cats treated with INS, CAB, RT and HX. The solid line represents the median. Kruskall–Wallis test with Dunn’s multiple comparisons test was used for comparison (*P <0.05, **P <0.01, ****P <0.0001). CAB = insulin plus cabergoline; HX = insulin plus hypophysectomy; IFT = improvement following treatment; INS = insulin as a single treatment; RT => radiation therapy
Follow-up and survival
Out of 127 cats, 70 (55%) developed concurrent diseases after the diagnosis of HS. Among these 70 cats, the most common diseases were chronic kidney disease (n = 25 [35%]), pancreatitis (n = 24 [34%]), heart disease (n = 11 [16%]), chronic inflammatory enteropathy (n = 9 [13%]), diabetic ketoacidosis (n = 3 [4%]), small cell intestinal lymphoma (n = 3 [4%]) and other neoplasia (n = 9 [12%]). Out of 127 cats, 47 (37%) were deceased before completion of the questionnaire. The cause of death/euthanasia was clearly stated in 38/47 (81%) (Table 7). Overall, HS directly contributed to death in at least 21/38 (55%) cases. The median survival time (MST) was 24 months (range 0–75). The MST was shorter in cats treated with insulin only (22 months; range 0–69) compared with all other treatments combined (36 months; range 3–75; P = 0.04) (Figure 3).
Causes of death* in 38 cats with hypersomatotropism

Data are n (%)
More than one cause of death could be stated

Kaplan–Meier survival curves for cats with hypersomatotropism treated with insulin as a single treatment (red dashed line) or with all other treatments combined (green solid line). The median survival time was longer in cats treated with all other treatments combined (P = 0.04)
Discussion
This large worldwide survey provides information about HS in cats from the owners’ point of view, focusing on the clinical presentation, the cats’ QoL at diagnosis, along with the effects of different treatments on QoL and the course of the disease. Data were obtained regarding 127 cats with HS from at least 11 different countries and four continents. However, the study was not designed to evaluate geographic differences of prevalence or the efficacy of specific treatments, and so regional variation cannot be excluded.5,6,15,16 In line with earlier studies, the majority of cats were male and older than 10 years.5,9,10,18 Nonetheless, 1/4 cats was female and around 10% were aged 8 years or younger, with the three youngest cats being only 4 years old. Based on these findings, HS should not be ruled out based on signalment. Although most cats were domestic mixed breed, Siamese and Maine Coons represented 5% and 4% of all cats with HS, respectively. This could be due to the high prevalence of these breeds in the general cat population or within the population of cats whose owners were prepared to respond to the survey; or, it might represent true breed predispositions. Significant breed predisposition for HS has not been previously demonstrated in cats, despite the Maine Coon breed being three times more represented among cats with IGF-1>1000 ng/ml. 5 The population of cats described in the present study showed heterogeneous epidemiological characteristics, with equal distribution in terms of lifestyle, environment and diet.
The most common clinical signs were those directly related to DM (ie, polyuria/polydipsia and polyphagia) followed by increased respiratory noise, physical changes, plantigrade stance, progressive weight gain and heart murmur, as previously described.5,18 There was a higher prevalence of plantigrade stance (20% of cats) in our study than previously reported in diabetic cats either with HS or without HS. 5 Plantigrade stance in cats with HS is usually considered the consequence of diabetic neuropathy; however, it was described in one non-diabetic cat in the present study and previously reported in 3/5 non-diabetic cats with HS.4,7,8 Sciatic neuropathy was confirmed by electrodiagnostic tests in one of these cats. 4 Of note, peripheral nerve dysfunction is a well-recognised complication of acromegaly in humans. 19
Around 5% of cats in the present study were not diabetic when diagnosed with HS and had not developed DM at the time the questionnaire was completed by the owners. The survey findings also support the suspicion, as is the case in humans, that non-diabetic cats with HS are likely more common than previously considered.
Serum IGF-1 concentration measurement was the most common diagnostic test performed, likely due to its ease of use and good diagnostic performance, with the 1000 ng/ml cutoff reported to be associated with a positive predictive value of 95% and a negative predictive value of 91% in an earlier study. 5 Interestingly, IGF-1 values below 1000 ng/ml or even 800 ng/ml were reported to be diagnostic by some owners in our survey. Several possible explanations could be considered. It is possible that some cats with HS had a serum IGF-1 result below the reported cutoffs, yet above the reference interval for cats without HS. 20 Alternatively, at least some of these cats might have been misdiagnosed. This issue is further confounded by the fact that, like in human medicine, various IGF-1 assays are being used in the clinical setting. The current survey did not obtain information on the type of IGF-1 assay used, which might possibly have affected the case definitions and results. Also, some diabetic cats had received insulin treatment for less than 6 weeks when IGF-1 concentration was measured. These cats might have had a relative insulin deficiency, increasing the risk of false-negative results. Adequate portal insulin concentration is required to stimulate the synthesis of IGF-1 by the liver. 20 Finally, some of the results could have been wrongly recollected by the owners.
Treatments aimed at eliminating the cause of HS were proposed by attending clinicians for the majority of cats. However, in one-third of cases, insulin was the only therapeutic option recommended to the owner, and other treatments were not even mentioned by the veterinarian who diagnosed HS. Despite this, some owners proceeded with further treatments on their cats after consulting veterinary specialists or after seeking advice from other sources, such as social media and online forums. This highlights the importance of detailed communication between veterinarians and cat owners about all treatment options when a cat is diagnosed with HS.
INS was the most common treatment administered, being selected by half of the owners. The insulin dose administered was extremely variable. Nonetheless, the median insulin dose was quite high, as previously described. 5 Importantly, up to 25% of cats experienced clinical hypoglycaemia, with some of them experiencing multiple episodes. This suggests that high concentrations of GH do not reliably protect against hypoglycaemic events and that frequent glucose monitoring and dose assessment are recommended. Cabergoline, radiotherapy and hypophysectomy all proved more effective in improving QoL than INS. Pasireotide was not compared with other treatments because it was used in only three cases, despite being proposed as treatment to around 10% of the owners as a previously proven successful medical management strategy.13,14 The extremely high cost of the drug likely played a role in this low uptake. Cabergoline is less expensive and widely available, but its efficacy is unclear. A recent pilot study failed to demonstrate an improvement of glycaemic control, serum IGF-1 or QoL in nine cats with HS and DM. 15 In contrast, treatment with cabergoline lead to diabetic remission in three cats with HS and DM in another report, 16 and improved glycaemic control in 25 cats with DM and HS even though their serum IGF-1 concentrations did not decrease. 21 Hypophysectomy performed better than any other treatment in our study, although, in terms of IFT, it did not reach significance when compared with radiotherapy, and radiotherapy in turn did not differ from cabergoline. The relatively low number of cats treated with hypophysectomy in our study is suspected to be the most likely explanation for the lack of clear differences. This was likely because of the high cost and limited availability of this treatment. Hypophysectomy is the only treatment capable of definitively removing the source of GH excess and achieves the highest diabetic remission rate,9,10 and so substantial improvement of QoL was expected. Randomised, head-on comparison studies with long-term follow-up are needed to provide a true comparison between treatments for HS in cats. In the present study, all cats treated with radiotherapy were analysed together, even though stereotactic radiotherapy (SRT) has proved superior to hypofractionated radiotherapy. 12 This might have decreased the overall calculated efficacy of the radiotherapy group.
Cats with HS showed a fair long-term prognosis, with an MST of 24 months. Despite this, the cause of death could be related to HS or its complications in approximately half of the cases. In addition, MST improved if any type of causal treatment was performed, reaching 32 months, which is similar to the MST of cats treated with hypophysectomy (28 and 44 months) or SRT (35 months) in previous studies.9,10,12 The most likely explanation is that causal treatments were more effective. Nevertheless, it is possible that owners whose cats had causal treatments performed were more motivated or had more financial reserves, positively affecting the survival time of their cats. Moreover, cats with more severe concurrent diseases or older age might have been withdrawn from the more invasive treatments of hypophysectomy or radiotherapy. A direct comparison between survival times for different causal treatments could not be performed due to the small group sizes and the limited number of cats that were deceased in any group. These findings further highlight the importance of causal treatment whenever feasible.
As is integral to any research based on surveying owners, the study has several limitations. All data were collected from owners who self-elected to join the survey. Recall bias might have impacted on completeness and accuracy of the information reported. As previously mentioned, HS could have been misdiagnosed in some cases. To reduce the rate of misdiagnosis, all cases were carefully reviewed by two experts, taking into account all the information available and excluding cases on the basis of a priori set rules. Misdiagnoses were thus hopefully limited and might not have markedly affected the results given the high number of cats included. Nonetheless, medical data (eg, insulin dosage, serum IGF-1 concentrations) are particularly prone to recall bias. For this reason, these data must be interpreted carefully. In addition, the QoL was not qualified in any way for the owners. Considering that each owner likely has a different understanding of the concept of QoL, and different levels of tolerance for the factors affecting it, these results represent the owner perception of the cats’ QoL rather than the cats’ actual QoL.
Conclusions
Middle- to older-aged diabetic cats with marked insulin resistance remains the most common presentation of HS. However, less typical presentations of younger and non-diabetic cats should additionally be considered. Veterinarians must carefully discuss all treatment options with the owners at the time of diagnosis. Given the survival advantage and the improvement of the QoL perceived by the owners, cats with HS should ideally be treated with hypophysectomy or radiotherapy, and if neither is feasible, cabergoline added to insulin therapy has the potential to improve affected cats’ QoL.
Supplemental Material
sj-docx-1-jfm-10.1177_1098612X221098718 – Supplemental material for Quality of life and response to treatment in cats with hypersomatotropism: the owners’ point of view
Supplemental material, sj-docx-1-jfm-10.1177_1098612X221098718 for Quality of life and response to treatment in cats with hypersomatotropism: the owners’ point of view by Andrea Corsini, Stijn JM Niessen, Diego D Miceli, Sarah Caney, Florian K Zeugswetter, Nadja S Sieber-Ruckstuhl, Carolina Arenas, Linda M Fleeman, Rodolfo O Leal, Martina Battellino and Federico Fracassi in Journal of Feline Medicine and Surgery
Supplemental Material
sj-docx-2-jfm-10.1177_1098612X221098718 – Supplemental material for Quality of life and response to treatment in cats with hypersomatotropism: the owners’ point of view
Supplemental material, sj-docx-2-jfm-10.1177_1098612X221098718 for Quality of life and response to treatment in cats with hypersomatotropism: the owners’ point of view by Andrea Corsini, Stijn JM Niessen, Diego D Miceli, Sarah Caney, Florian K Zeugswetter, Nadja S Sieber-Ruckstuhl, Carolina Arenas, Linda M Fleeman, Rodolfo O Leal, Martina Battellino and Federico Fracassi in Journal of Feline Medicine and Surgery
Footnotes
Acknowledgements
The authors would like to thank Teresa Stöckle for the German translation of the questionnaire, Maria Joana Dias for the Portuguese translation of the questionnaire, Vet Professionals and all colleagues who distributed the questionnaire. Most of all, we thank all the owners who participated in the survey and shared the story of their cats.
Author note
This paper was presented in part at the ECVIM online congress 2021.
Supplementary material The following files are available online:
File 1: Questionnaire (English version)
File 2: Selected demographic variables of the 127 cats with hypersomatotropism included in the study.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not necessarily required.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.