
Abstract
Objectives
The aim of this multicentre retrospective study was to describe the clinical presentation, imaging findings, diagnosis and outcomes of cats with retrobulbar neoplasia.
Methods
A total of 37 cats that were diagnosed with retrobulbar neoplasia and underwent advanced imaging were recruited from searches of the clinical records of two referral hospitals. All cats had neoplasia confirmed via cytology or histopathology. Data relating to the signalment, presentation, results of investigations, treatment and outcome were recorded. A review of imaging studies was performed where possible.
Results
In total, 23 cases (62%) were presented with respiratory signs. Exophthalmos was the most common ophthalmological examination finding, present in 18 cases (49%). Thirty-two cases (86%) had secondary extension of neoplasia to the retrobulbar space (most commonly from the nasal cavities), present in 20 cases (54%), of which 12 were lymphoma. In cases where contrast was administered, 28/35 (80%) had contrast-enhancing masses. Orbital extension was detected in 21 cases (57%), exophthalmos in 22 (59%), globe deformation in 12 (32%) and local lymphadenomegaly in 22 (61%). In total, 36 (97%) retrobulbar tumours were malignant. Thoracic imaging, where it was performed, was concerning for metastasis in 8/25 cases (31%), with abdominal imaging suggestive of metastasis in 5/12 (42%). The most common diagnosis was lymphoma with 19 cases (51%), with nasal lymphoma representing 12 of these, followed by carcinoma in 10 (27%). The median survival time, for cases where death was recorded, was 85 days (range 1–263 days).
Conclusions and relevance
To the authors’ knowledge, this is the largest study of neoplasia affecting the feline retrobulbar space. Retrobulbar tumours in cats are overwhelmingly malignant, and commonly due to secondary extension of tumours originating elsewhere. Lymphoma, particularly arising from the nasal cavities, was the most common cause. Cats presenting with signs suggestive of retrobulbar disease should be assessed for disease affecting any of the structures of the head.
Keywords
Introduction
The orbital tissues consist of the orbital bones, fascia, extraocular muscles, fat and the globe within. 1 The retrobulbar space lies near these, and the retrobulbar tissues include the zygomatic salivary gland (SG), masticatory and extraocular muscles, nerves, blood vessels and the lacrimal gland. 2 Also in close proximity are the nasal cavity, paranasal sinuses, cranial cavity, mandibular processes and the mouth.2–4 Diseases affecting these tissues can ultimately affect the eye and retrobulbar space.
Non-neoplastic differentials for feline orbital and retrobulbar space disease include bacterial abscess/cellulitis, mycosis, Onchocerca lupi infection, orbital foreign bodies, emphysema secondary to sinus perforation, rhinitis and eosinophilic inflammatory disease.5–17 Most feline retrobulbar tumours are reported to be malignant. 18 Owing to the anatomical proximity of other structures, secondary invasion of neoplasia into the retrobulbar space has also been described. It is reported that 57% of retrobulbar tumours in cats are secondary, and the majority of orbital neoplasia is also due to secondary extension from adjacent tissues.18,19 Invasion of nasal cavity neoplasia to the retrobulbar space appears to be common.9,20
Typical clinical signs of orbital and retrobulbar disease include exophthalmos, enophthalmos and globe deviation/strabismus.3,18,21 Other common signs of feline retrobulbar disease include nictitating membrane protrusion, proptosis, periorbital swelling, ocular hypertension (due to venous drainage compression), ocular discharge, pain on opening the mouth, lagophthalmos-associated corneal disease, resistance to retropulsion, chemosis, swelling/fistulation of the oral mucosa, cranial nerve defects and nasal discharge if the nasal cavity is involved.2–4,22,23
Epithelial tumours have been reported as the most common feline orbital and retrobulbar neoplasms, particularly squamous cell carcinoma (SCC).18,19,23 Other tumours described include lymphoma, undifferentiated carcinoma, malignant melanoma, adenocarcinoma, fibrosarcoma, chondroma, meningioma, osteosarcoma, hemangiosarcoma and feline restrictive orbital myofibroblastic sarcoma (FROMS). 19 FROMS, previously termed ‘pseudotumour’ is a highly invasive neoplasm that often progresses from unilateral to bilateral disease and is poorly responsive to therapy.3,18,19,22,24–31 SCC can mimic FROMS. 22
Radiography appears insensitive for the detection of orbital bone pathology. 32 If orbital or retrobulbar neoplasia is suspected, advanced imaging is recommended to assess the degree of local extension and plan for diagnostic sampling.3,32 Orbital bone lysis has been significantly associated with neoplasia over non-neoplastic retrobulbar disease, and globe indentation has been frequently observed with lymphoma.2,33 CT is more sensitive than ultrasonography for identifying extraorbital extension. 34 Diagnosis in cats has typically been achieved via fine needle aspiration (FNA) of the retrobulbar lesion or post-mortem histopathology.18,22,30
The literature regarding feline retrobulbar neoplasia is scarce, with little known about its aetiology and clinical findings. The prognosis for affected cats has generally been considered poor, with a reported median survival time (MST) <1 month, with 35% of dogs and cats euthanased at the time of diagnosis. 18 The aim of this retrospective study was to describe the clinicopathological findings in a larger cohort of cats diagnosed with retrobulbar neoplasia.
Materials and methods
This study was a multicentre, retrospective, descriptive case series. Medical records of two UK referral centres were searched for cats with a diagnosis of neoplasia affecting a retrobulbar space between October 2007 and February 2019 in one centre and November 2015 and September 2021 in the other. Information gathered included age, sex, breed, clinical signs, physical examination findings, imaging findings, laboratory results, diagnosis method, tumour type, treatment and any follow-up data.
Presenting signs were defined as findings described by the owner or referring veterinarian prior to referral. Respiratory signs were defined as dyspnoea, nasal discharge, epistaxis, reduced nares airflow or increased respiratory noise. Ocular signs were defined as ocular discharge, blepharospasm, nictitating membrane protrusion, exophthalmos/enophthalmos, resistance to retropulsion and any ophthalmoscopy abnormalities. Signs of swelling/mass were defined as periorbital swelling, facial asymmetry, visible mass or a history of mass removal. Physical examination and ophthalmological findings were based on assessment at the referral institution. Ophthalmological examination was preferably performed by, or under the supervision of, a board-certified ophthalmologist including neuro-ophthalmic examination, slit lamp biomicroscopy, tonometry and ophthalmoscopy.
Cases were included only if retrobulbar neoplasia was confirmed via cytology and/or histopathology and there was confirmed retrobulbar space involvement on MRI or CT studies. Review of imaging studies of the head was performed where possible by a board-certified radiologist (RD), with focus on describing any retrobulbar/ocular changes (including loss of retrobulbar fat and mass effect on other structures), primary location of tumours, and lymph node changes. Where review was unavailable, data were extracted from imaging reports verified by a board-certified radiologist. If a specific finding was not mentioned, it was recorded as absent. Primary tumour site was recorded based on radiologist opinion. If a strong suspicion did not exist, an ‘unknown’ location was recorded.
Cytology and histopathology were all performed or verified by board-certified pathologists. Final diagnosis was recorded in as much detail as possible, consistent with the pathology report. Results of additional tests, including immunohistochemistry/immunocytochemistry, were recorded if available.
Where available, details of treatment protocol and the outcome at the last contact time were recorded. Survival time where death was recorded, or total follow-up time for cases where it was not, was calculated from the date of presentation to the referral centre to the date of death or last contact.
Descriptive data were evaluated using commercial software (Microsoft Excel for Mac version 16.56). Categorical variables were expressed as frequencies and percentages. Numerical values were expressed as a median value and range.
Ethical approval was granted by the Clinical Research Ethical Review Board of one of the centres (URN SR2019-0345).
Results
In total, 37 cases met the inclusion criteria. The median age was 10 years (range 3–16 years). The median body weight was 4.16 kg (range 2.8–7.2 kg). Of the cats, 19 (51%) were spayed females and 18 (49%) were castrated males. There were 24 (64%) domestic shorthairs, three (8%) domestic longhairs, three (8%) Siamese, two (5%) British Shorthairs and five others of one each (3%): Devon Rex, Chinchilla, European Shorthair, Burmese and Maine Coon.
Clinical findings
The cases had a variety of signs reported prior to referral (Table 1), the majority with respiratory signs. Eight cases (22%) had both ocular and respiratory signs.
Presenting complaints prior to referral

Data are presented as n (%)
Twenty cases (54%) had respiratory signs noted on physical examination at the referral centre. There was nasal discharge in 14 cases (38%), of which seven had epistaxis; 14 (38%) had increased respiratory noise, 12 (32%) had facial asymmetry/mass and 11 (30%) had lymphadenomegaly. A nasal mass was observed externally in six cases (16%) and an oral lesion in six (16%). Five cases (14%) had dyspnoea and six (16%) had reduced airflow through one or both nostrils.
A total of 33 cases (89%) had abnormal ophthalmological findings (Table 2). In the five cases with anisocoria, the diseased eye had mydriasis. One cat had unilateral blindness.
Ophthalmological examination findings

Data are presented as n (%)
Three cases (8%) displayed neurological abnormalities. One had unilateral myokymia, Horner’s syndrome and trigeminal dysfunction, eventually diagnosed with primary retrobulbar adenosquamous carcinoma with cranial nerve extension. One case had general proprioceptive ataxia in all limbs with a left-sided vestibular component and was subsequently diagnosed with nasal/meningeal lymphoma and raised intracranial pressure. The other had non-ambulatory paraparesis and difficulties urinating/defecating, with T3–L3 lesion localisation, eventually diagnosed with disseminated haemangiosarcoma with presumed spinal cord involvement, haemorrhage or neoplastic embolus.
Haematological data were available for 35 cases (95%). Lymphopenia was present in 14 cases (40%), neutrophilia in six cases (17%) and six cases (17%) had anaemia. Serum biochemistry results were available for 35 cases (95%) with the most common abnormalities being hypoalbuminaemia in seven (20%), increased urea concentration in seven (20%), increased alkaline phosphatase activity in five (14%), hyperglobulinaemia in five (14%), hypoproteinaemia in five (14%), total hypercalcaemia in four (11%), hyperglycaemia in four (11%), increased creatinine concentration in four (11%) and total hypocalcaemia in three (9%).
Imaging findings
Advanced imaging of the head was performed in all cases (Table 3). Five cases (14%) underwent MRI (including all displaying neurological abnormalities), with the other 32 (86%) undergoing CT. Imaging review was available for 27 cases (73%). One cat had a retrobulbar mass that was not causing significant mass effect on surrounding structures. Intracranial/brain involvement was described/suspected in six cases (16%), with cribriform plate lysis in one (nasal lymphoma) and extension via other structures in the rest. Nineteen cases (51%) had a right-sided retrobulbar lesion, with 18 (49%) having left-sided disease. Figure 1 displays representative examples of a case with a primary tumour and a case with secondary extension to the retrobulbar space.
Advanced imaging findings*

Data are presented as n (%)
Intravenous contrast agent was not administered in two cases. Seven cases did not have cervical lymph nodes included in the imaging study and one cat had no local lymph nodes included

Post-contrast CT images, medium frequency reconstruction algorithm, WW400/WL40. (a) Primary retrobulbar lymphoma (purple arrow), with evident mass effect of the globe (yellow arrow); (b) intranasal carcinoma (yellow arrow), with retrobulbar extension (purple arrow)
Twenty-six cases (70%) underwent thoracic imaging (CT in 24, radiography in two). Twelve (46%) were normal, eight (31%) showed concern for neoplastic involvement and six (16%) showed bronchial changes only. Only one case had diagnostic sampling of a lesion performed (carcinoma, suspected primary pulmonary). Abdominal imaging was performed in 12 cases (32%; CT in 11, ultrasonography in one). In five of these, lesions suggestive of neoplasia were revealed. FNA cytology confirmed neoplasia in three cases with renal lesions – two with lymphoma of unknown origin (one of which also had a duodenal lesion which was not sampled) and one with disseminated haemangiosarcoma (in which a bladder lesion was also confirmed neoplastic with cytology). All were the same tumour type as that of the retrobulbar space. One case with a renal lesion (carcinoma of unknown origin) and one with a duodenal lesion (nasal lymphoma) did not undergo sampling of these areas. There were potential neoplastic hepatic lesions in two more cases (primary retrobulbar lymphoma and nasal lymphoma), which were not sampled.
Diagnosis
All cases had confirmation of neoplastic disease of the retrobulbar space via cytology and/or histopathology (Table 4). Twelve cases (32%) were diagnosed via cytology alone, and 17 (46%) solely via histopathology. Eight cases (22%) had both cytology and histopathology performed. Thirty-six (97%) tumours were malignant. Twelve of 20 nasal tumours (60%) were lymphoma, with two more (10%) classified as round cell tumours (suspected lymphoma). Twelve of 19 lymphoma cases (63%) had a nasal origin, as did both round cell tumours. Of the five cases with primary retrobulbar neoplasia, two (40%) had FROMS and there was one case each of SCC, adenosquamous carcinoma and lymphoma. Immunohistochemistry was performed in six cases, four of which had lymphoma, all of B-cell origin.
Classification of tumours
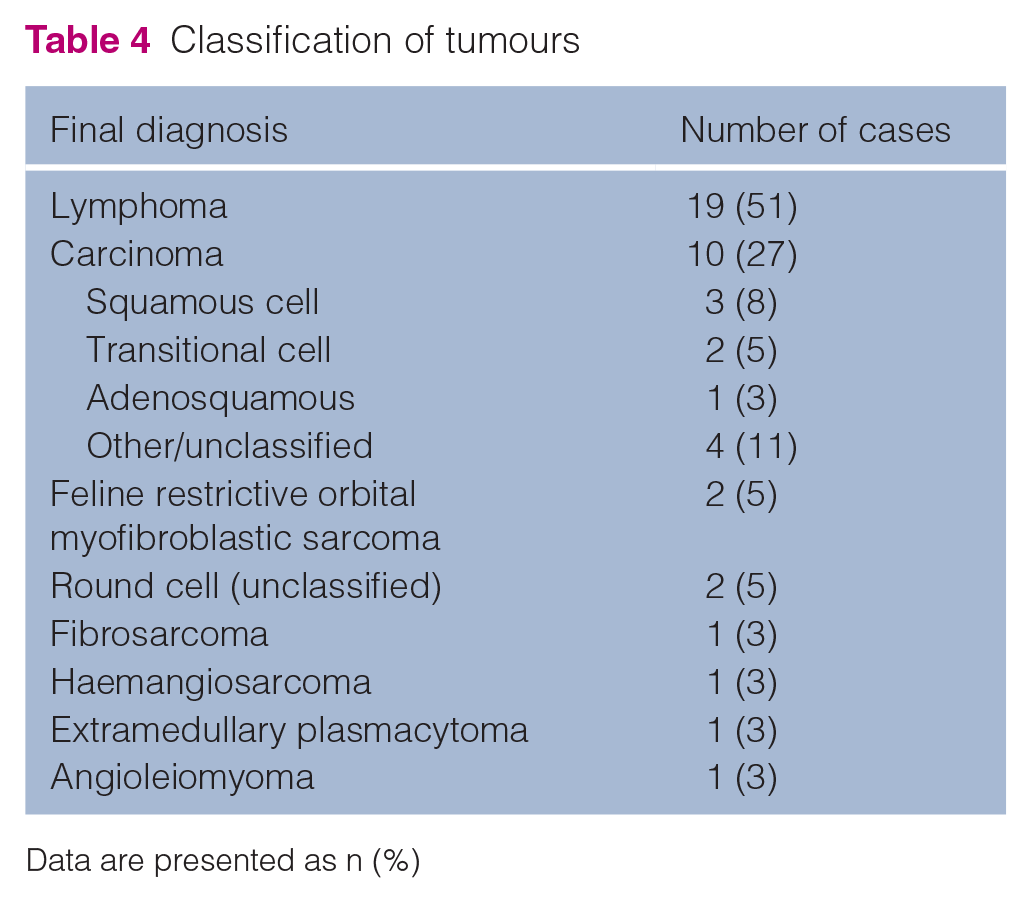
Data are presented as n (%)
Treatment
Three cases (9%) underwent exenteration and mass removal. Seventeen cases (46%) received chemotherapy (excluding glucocorticoid or non-steroidal anti-inflammatory sole-agent therapy), with protocols including vincristine and glucocorticoids for lymphoma in 12 (32%), variously alongside other agents (lomustine, cytarabine, cyclophosphamide, L-asparaginase). Carboplatin sole-agent therapy was administered to one case with fibrosarcoma and one with carcinoma. Other protocols described were chlorambucil/prednisolone (plasmacytoma), toceranib/cyclophosphamide (angioleiomyoma) and one unknown (lost to follow-up).
Outcome
Follow-up data were available for 23 cases (62%). The date of death was known for 16 cases, with the MST being 85 days (range 1–263 days). In the seven cases where the cause was recorded, all were euthanased due to their neoplasia. Three cases (8%) were euthanased at diagnosis. For the seven cases where death was not recorded, the median follow-up time at the last point of contact was 100 days (range 14–790 days). The MST for seven lymphoma cases was 89 days (range 10–213 days) and five more were lost to follow-up after a median of 151 days (range 21–790 days). Of the three cases presented with neurological abnormalities, one survived 30 days (retro-bulbar adenosquamous carcinoma) and the other two were lost to follow-up at 28 (nasal/meningeal lymphoma) and 151 days (disseminated haemangiosarcoma). The two FROMS cases survived 119 and 263 days, treated with exenteration and conservative management, respectively. Of the five cases with primary retrobulbar neoplasia, four had an MST of 121.5 days (range 30–263 days) and one was lost to follow-up after 14 days. The MST for 12 cats with secondary extension to the retrobulbar space was 67 days (range 1–213 days).
Discussion
Feline retrobulbar neoplasia has been rarely reported upon therefore, the aim of this study was to describe it in a larger case series to improve our understanding of this clinical entity.
As in previous studies, malignant tumours were more common than benign tumours – 97% compared with the 86% reported by Attali-Soussay et al in 2001. 18 A large proportion (88%) had secondary retrobulbar involvement rather than primary neoplasia. This is higher than previously reported in feline retrobulbar (57%) and orbital (71%) neoplasia.18,19
Most cases were referred with respiratory signs (23/37, 62%), which have not been particularly reported as associated with retrobulbar disease in cats previously.1,18 Many cases with respiratory signs also had evidence of mass effect/swelling or ocular disease (16/23, 70%). Respiratory signs were more prevalent than ocular, likely reflecting the predominance of secondary involvement of the retrobulbar space, most often from the nasal cavity. Previous retrospective studies of feline retrobulbar masses did not report primary nasal disease, though it was the most common primary location in canine studies.2,34 Additionally, a case series of feline sinonasal disease did observe a high prevalence of retrobulbar mass in neoplastic disease. 9 No cases with primary retrobulbar neoplasia were presented with respiratory signs here. In cats with advanced nasal neoplasia, retrobulbar involvement should also be considered.
Similar to previous reports, the most common ophthalmic abnormalities were exophthalmos, ocular discharge, nictitating membrane protrusion and decreased retropulsion.1,3,23 Although only five cases (14%) were presented with a history of exophthalmos, 18 (49%) had it noted after physical examination, increasing to 22 (59%) following imaging. Exophthalmos in cats is often subtle, particularly in the early stages of disease. Twenty-two cases (59%) had no ophthalmological abnormalities reported in the history, but only four (11%) had a normal ophthalmological assessment at the referral centre. Decreased ocular retropulsion has been considered near-pathognomic for retrobulbar disease, but the sensitivity was much lower in our series (30%) compared with previous studies in dogs.2,35 This could be due to true low prevalence, lack of retropulsion being performed as part of the examination, or the relatively smaller retrobulbar and orbital space in cats compared with dogs making it more difficult to perform. All of this suggests that exophthalmos and other ocular abnormalities can sometimes be subtle and overlooked, underscoring the importance of a thorough assessment of all structures of the head. However, retrobulbar neoplasia cannot be excluded by a normal ophthalmological examination.
The majority of cases where contrast was administered had enhancement reported, with 19/28 cases (68%) having homogeneous uptake, in contrast to canine retrobulbar neoplasia, which has been associated with heterogeneous enhancement. 2 Reduced retrobulbar fat was reported in all 28 cases that underwent imaging review, and this finding has also commonly been reported (85%) in canine retrobulbar neoplasia. 2 Other imaging findings also had prevalence similar to those previously reported for canine disease, with exophthalmos in 22 cases (59%) orbital involvement in 21 (57%), zygomatic SG deformation in 17 (46%), globe deformation in 12 (32%) and zygomatic SG enlargement in two (5%) compared with 68%, 75%, 40%, 53% and 5%, respectively. 2
In contrast to previous reports of retrobulbar/orbital neoplasia, where carcinomas predominated, lymphoma was most common here.18,19 A small MRI case series of nasal tumours by Tanaka et al also had lymphoma cases predominating. 20 Nasal lymphoma in particular was the most commonly identified tumour type, representing 32% (12 of all cases), or 38% (14 cases) if round cell tumours suspected to be lymphoma were included. In cats, the nasal cavities have been reported to be the most common extranodal lymphoma site, and lymphoma as the most common nasal tumour.36–38
Retrobulbar neoplasia in dogs and cats was previously reported to have a poor prognosis. 18 Owing to the low number of cases within each group of tumour or treatment type, meaningful statistical analysis of the impact of different clinicopathological or imaging features on survival was not possible here. For cases with lymphoma, the MST was 89 days, similar to the MST of 85 days for the total study population. There were two long-term survivors lost to follow-up at 700 (nasal lymphoma with renal metastasis) and 790 days (lymphoma at base of skull). These were both treated with L-asparaginase, cyclophosphamide, vincristine and prednisolone, with cytarabine also part of the protocol for the former. Nasal lymphoma has been consistently described as having a prolonged survival when treated with chemotherapy and/or radiotherapy.21,39 Mean reported survival times with treatment are 12–30 months.36,40–42 The lower MST in the five nasal lymphoma cases in our study where survival time was known (89 days) may suggest that retrobulbar involvement could be a negative prognostic factor. However, retrobulbar involvement has not previously been consistently associated with poorer outcomes in feline lymphoma.42,43 One case report indicated that treatment of nasal lymphoma with orbital involvement can result in prolonged survival. 29 Primary retrobulbar lymphoma – present in one case here, which survived 124 days with cyclophosphamide, vincristine and prednisolone – has been described rarely in both cats and dogs.26,44–48 Complete remission and a possible survival time of over 4 years has been observed. 44
Feline nasal lymphoma has been found to be predominantly of B-cell origin (72–95%).37,49–51 Of the four lymphoma cases in our study (three nasal) that underwent immunocytology/immunohistochemistry, all were B-cell. Primary retrobulbar lymphoma in both cats and dogs may have a high prevalence of T-cell and T-cell rich B-cell when compared to other forms of the disease.45,46 Mixed morphology of nasal lymphoma has also been reported. 49 It is unknown if morphological subtyping of retrobulbar lymphoma may aid treatment or affect prognosis.
Two cases with FROMS constituted 40% of the primary retrobulbar neoplasms. FROMS appears to present primarily with ocular signs before observation of a visible mass.30,31 This was also apparent for the cases here, one of which had exophthalmos and one had ocular discharge and nictitating membrane protrusion.
This study has several limitations, mainly relating to its retrospective nature. Staging procedures and treatment plans were not standardised, which, along with a heterogeneous disease population, makes meaningful comparisons between groups difficult. Despite this, all cases benefited from advanced imaging, with most being reviewed by a board-certified radiologist. Not all cases were examined by a board-certified ophthalmologist, meaning subtle changes were more likely to have been missed. In addition, rigid inclusion criteria requiring a confirmed neoplastic diagnosis made inclusion of a larger number of cases challenging. Histopathology was unavailable for every case; however, cytology often allowed determination of the main tumour type. A large proportion of cases had lymphoma, for which cytological diagnosis is often sufficient.19,49
Conclusions
Our study found that most feline retrobulbar tumours are malignant and secondary involvement is more common than primary. Lymphoma was the most common diagnosis, and the nasal cavities were the most common primary location. To the authors’ knowledge, this study is the largest description of feline retrobulbar neoplasia to date.
Footnotes
Author note
These results were presented, in part, as a poster presentation at ECVIM-CA Congress 2020.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee, while not necessarily required, was nonetheless obtained, as stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.