
Abstract
Case series summary
The aim of this case series was to describe the clinical features and treatment of paronychia in cats diagnosed with patellar fracture and dental anomaly syndrome (PADS). Clinical records, photographs, microbiology, cytology and histopathology reports were collected, and follow-up was obtained. Five cats with paronychia were included. All five cats had multiple digits of multiple limbs affected and eventually underwent amputation of the third phalanx of one or multiple digits. A total of 36 digits were affected, 17% (n = 6/36) resolved with medical management and 83% (n = 30/36) were eventually treated successfully by amputation. The cats had treatment with numerous courses of antibiotics (range 7–20; mean 11 courses) over periods of time ranging from 10 to 67 months (mean 32 months).
Relevance and novel information
Chronic paronychia may be an additional clinical feature of PADS and the probable mechanism involves poor integrity of osteopetrotic bone, loss of normal nailbed anatomy and secondary osteomyelitis of the distal phalanx. Medical management with antibiotics, anti-inflammatory therapy and steroid treatment may improve the clinical signs in the short term; however, in severe instances, amputation of the third phalanx of the affected digit seems to be necessary to resolve repeated recurrences and discomfort. Additional information on the long-term outcome is required. In any cat with atraumatic patellar fractures and/or retained deciduous teeth, paronychia may require surgical management if medical management is unsuccessful.
Introduction
Patellar fracture and dental anomaly syndrome (PADS) is a phrase that has been coined to help describe cats with the common features of patellar fractures and, in most cases, additional dental anomalies.1,2 These cats commonly present at a mean age of 28 months when they sustain their first patellar fracture. In more than 50%, a fracture of the contralateral patella occurs with a mean gap of 3 months. 3 Other abnormalities have been noted, such as persistent deciduous teeth and/or unerupted permanent teeth, and mandibular and maxillary abnormalities, such as abscesses and osteomyelitis.2,4 In nearly half of affected cats, additional fractures to other bones and humeral intercondylar fissures occur.1–3,5 Furthermore, in our experience, a small number of cats affected by PADS develop persistent and recurrent paronychia.
Paronychia is an inflammation of the folds of tissue surrounding the nail. This can be associated with digit swelling, discomfort and/or lameness.6,7 One or multiple digits of one or multiple limbs can be affected. The two most common presentations of paronychia in cats are exudation with crusting and pedal pruritus with waxy exudate. 8 Feline paronychia is not common. It has been reported to be an extension of a primary skin disease or secondary to hyperadrenocorticism or neoplasia. 9 The primary skin disease could include bacterial dermatitis, dermatophytosis and pemphigus foliaceus located in one or multiple nailbeds.8,10 Depending on geographical location, notoedric mite infestation is reported as a causative agent.8,11 Primary pulmonary neoplasia or local squamous cell carcinoma are neoplastic diseases associated with paronychia in the cat.12,13
Establishing the cause and treating feline paronychia can be challenging.6,7,13 It is important to be aware of the causes of paronychia to be able to provide appropriate treatment for affected cats. Amputation of digits is invasive but sometimes necessary for diagnosis and treatment of feline digit disease. The aim of this case series is to report on the clinical and histological and radiographical features of paronychia in cats with PADS and their treatment outcome.
Case series description
Cats with a history of paronychia and patellar fractures were recruited from the database of cats with PADS; case information on affected cats has been collected since 2005 (SL-H). Cases in the database included cats with the following clinical features: transverse patellar fractures with or without dental anomalies (including persistent deciduous teeth and unerupted adult teeth) and with or without atraumatic fractures to other bones. Of the cases identified, all information submitted to the database was collated and further case follow-up was performed. Where available, records of clinical history, pictures of paronychia, radiographs and microbiology and histopathology reports were included. The database had a total of 218 cats (August 2020), seven of which had paronychia recorded. Two cats were excluded owing to insufficient information. The results and treatments for five affected cats are summarised in Tables 1 and 2, and given in more detail on a case-by-case basis. A total of 36 digits were affected, 17% (n = 6/36) resolved with medical management and 83% (n = 30/36) were eventually treated successfully by amputation. The cats had treatment with numerous courses of antibiotics (range 7–20; mean 11 courses) over periods of time ranging from 10 to 67 months (mean 32 months). Follow-up was performed by contacting owners and veterinarians; mean follow-up time was 41 months.
Summary of presentation of patellar fracture and dental anomaly syndrome per case

Corresponding number in the ‘Patellar fracture and dental anomaly database’
FN = female neutered; DSH = domestic shorthair; MN = male neutered; Y = yes
Summary of investigations and treatment per case

Corresponding number in the ‘Patellar fracture and dental anomaly database’
P3 = third phalanx; LH = left hindlimb; RH = right hindlimb; D = digit; LF = left forelimb; RF = right forelimb
Case 1
An 18-month-old neutered female domestic shorthair (DSH) cat (number 51 in the ‘Patellar fracture and dental anomaly database’) located in the UK, presented with left hindlimb lameness (case 8 in a previous study). 4 Radiographs revealed bilateral patellar fractures, and multiple persistent deciduous teeth were noted on clinical examination. At approximately 3 years of age, paronychia was first noted to the left hindlimb (digit unknown). The paronychia initially resolved with empirical systemic antibiotic treatment. Over the course of 5 years, multiple episodes of paronychia of the toes on the right and left hindlimbs occurred. For treatment details, see Table 3 and Figure 1. The paronychia only affected the hindlimbs and a total of eight antibiotic courses were prescribed. Paronychia of digit 4 of the right hindlimb resolved with medical management. At 8 years of age the cat was markedly affected by paronychia of digit 2 on the left hindlimb. Radiographs showed soft tissue swelling adjacent to the affected digit. Culture and sensitivity were performed. As there was no improvement on symptomatic treatment, the affected digit was amputated. At the time of writing, 29 months later, no further paronychia had occurred. The cat was well in itself, despite chronic osteomyelitis of the mandible with a persistent draining tract sinus, associated with unerupted teeth.
Detailed description of paronychia treatment of case 1, patient number 51
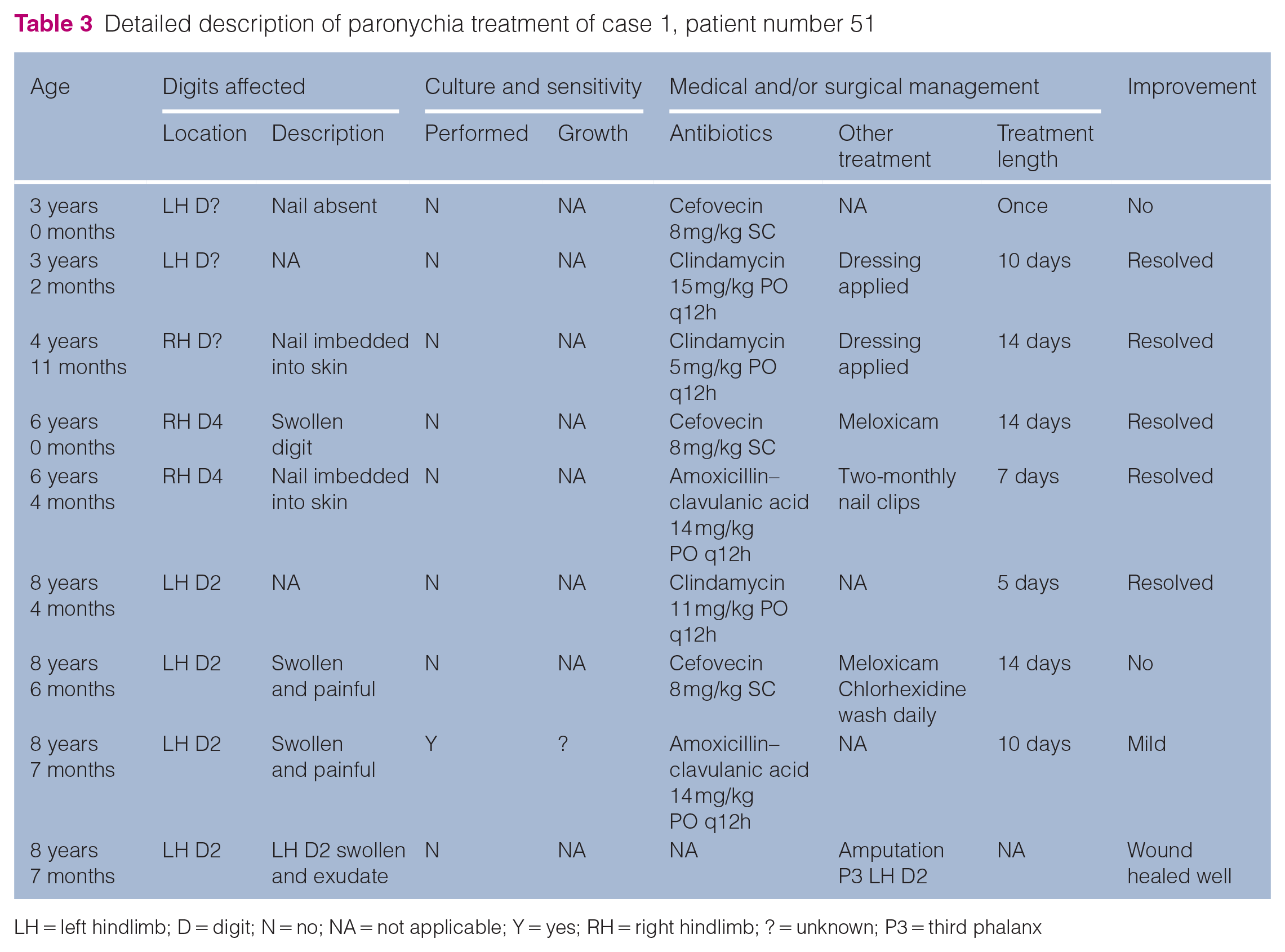
LH = left hindlimb; D = digit; N = no; NA = not applicable; Y = yes; RH = right hindlimb; ? = unknown; P3 = third phalanx

Digits affected by paronychia in case 1, patient number 51: RF = right forelimb; LF = left forelimb; RH = right hindlimb; LH = left hindlimb; black = not affected; dark grey = amputated; light grey = resolved with medical management
Case 2
A neutered female DSH cat, located in the UK (number 83 in the database), presented at 1 year of age for recurrent nailbed infections, specifically digit 1 on both forelimbs. Ten antibiotic courses were prescribed on seven different occasions over the course of 10 months. A total of four digits were affected on both thoracic limbs. Empirical and culture-based (performed twice) antibiotic treatment did not resolve the paronychia. The cat was referred to a dermatologist and topical treatment was started. Further treatments were performed by the general practitioner. Owing to discomfort, amputation of the third phalanx (P3) of digit one of both forelimbs, and digits two and five of the right forelimb were performed within the year (Figure 2). Based on medical records, histopathology indicated osteomyelitis. All wounds healed well, and no further paronychia occurred over the following 4 years. At approximately 4 years of age, the cat fractured both patellae, despite being an indoor cat. The last follow-up was at age 6 years; no further paronychia had occurred. For treatment details, see Figure 3 and Table 4.
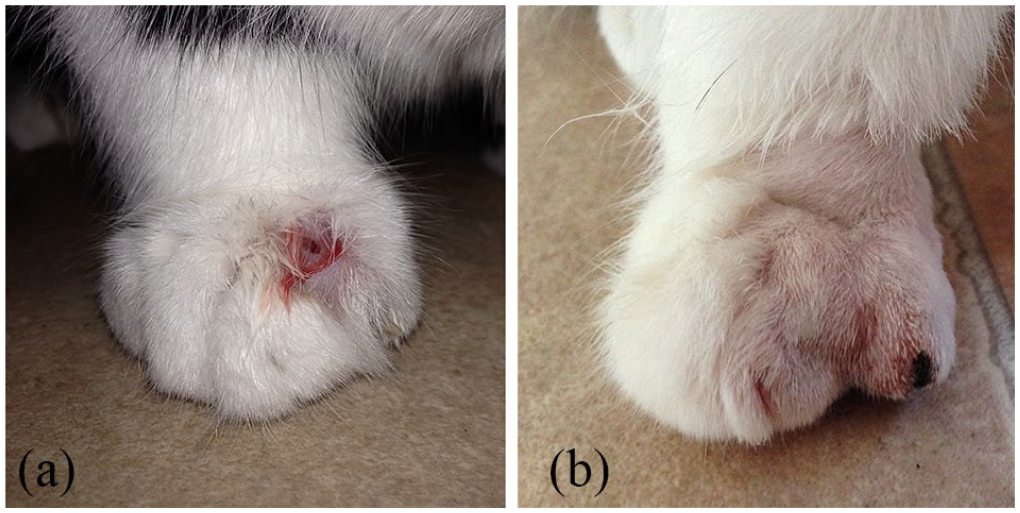
Case 2. (a) Severe paronychia noted on right forelimb digit 2. Local swelling, alopecia, ulceration and serosanguinous discharge is noted. (b) Post-amputation of third phalanx of right forelimb digit 2

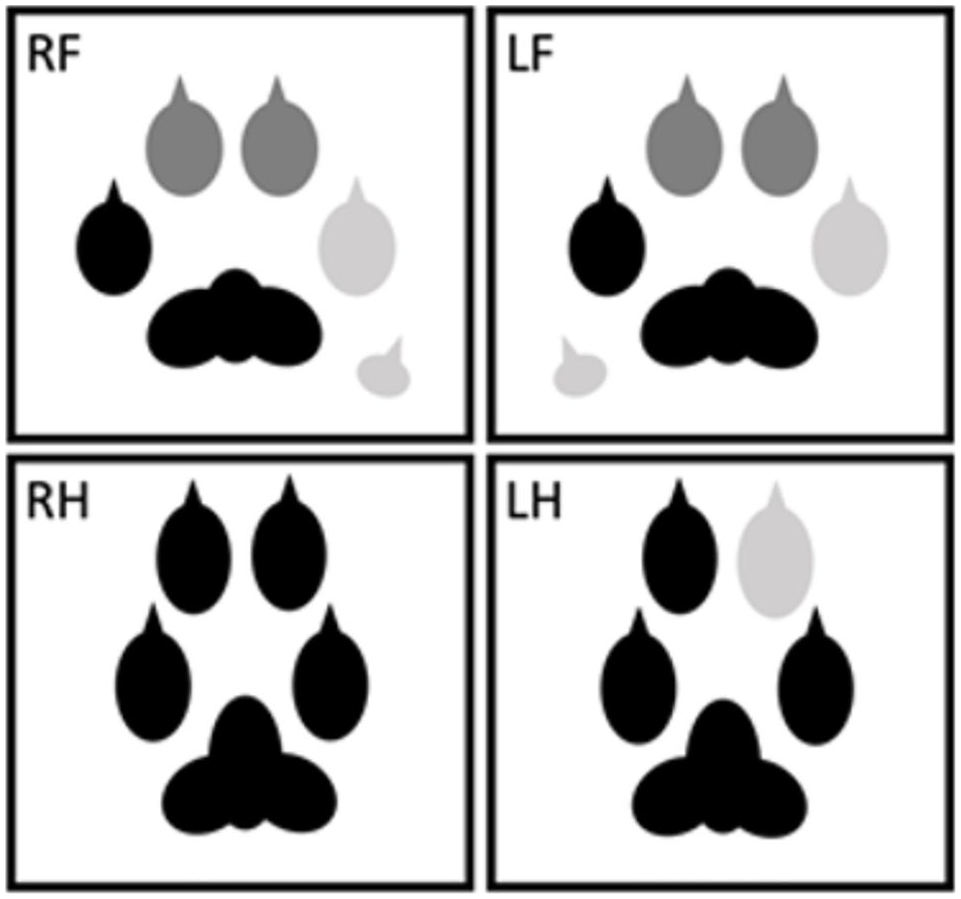
Digits affected by paronychia in case 2, patient number 83. RF = right forelimb; LF = left forelimb; RH = right hindlimb; LH = left hindlimb; black = not affected; dark grey = amputated
Detailed description of paronychia treatment of case 2, patient number 83
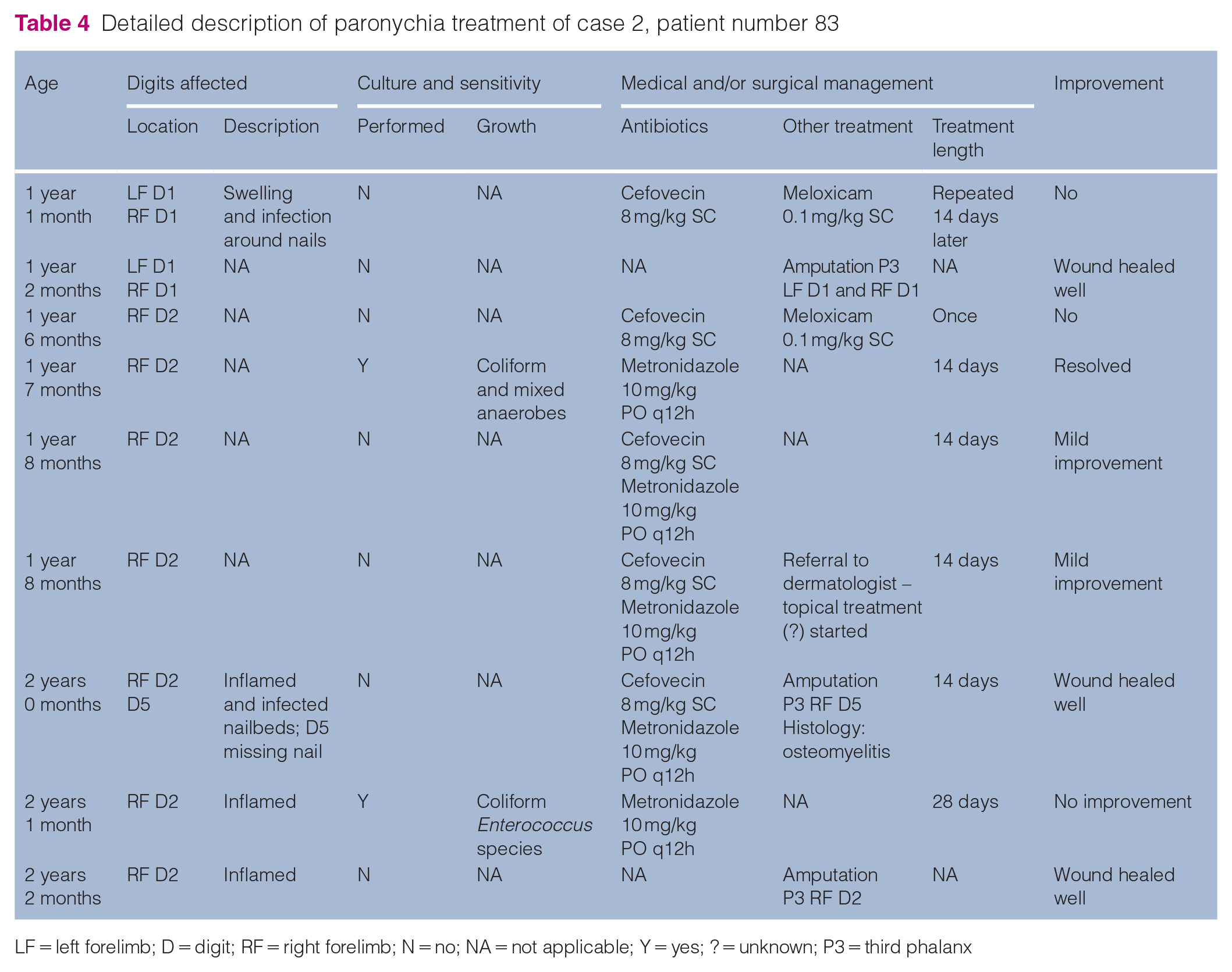
LF = left forelimb; D = digit; RF = right forelimb; N = no; NA = not applicable; Y = yes; ? = unknown; P3 = third phalanx
Case 3
A neutered female DSH cat, located in the UK (number 104 in the database), presented at approximately 4 years of age for paronychia of digit one of the left forelimb and the left hindlimb (digit unknown). It was medically managed for 4 years with empirical and culture-based (performed five times) antibiotics and topical treatments. For treatment details, see Figure 4 and Table 5. Twenty antibiotic treatments were prescribed on 18 occasions. Treatments were sometimes successful; however, relapse of paronychia was common. While under treatment, the cat sustained bilateral patellar, right tibial and right lateral humeral condylar fractures. A CT scan showed multiple unerupted and retained teeth. Three limbs were intermittently affected, leaving the right hindlimb unaffected. A total of nine digits were affected, with five resolving with medical management. At 7 and 8 years of age, P3 of digits 3 and 4 of the right and subsequently the left forelimb were amputated for chronic paronychia (Figures 5 and 6). Two distal phalanges were evaluated histologically. The bones showed large amounts of retained cartilage, which was interpreted as retained primary spongiosa, and one phalanx was necrotic and heavily colonised by bacteria (Figures 7 and 8). The other phalanx had suppurative inflammation replacing the keratin claw and osteomyelitis of the palmar aspect of the ungulate process (not shown). At the time of writing, 4 months after amputation, the wounds had healed well and there was no recurrence of clinical signs.
Digits affected by paronychia in case 3, patient number 104. RF = right forelimb; LF = left forelimb; RH = right hindlimb; LH = left hindlimb; black = not affected; dark grey = amputated; light grey = resolved with medical management
Detailed description of paronychia treatment of case 3, patient number 104

LF = left forelimb; D = digit; LH = left hindlimb; ? = unknown; N = no; NA = not applicable; Y = yes; RF = right forelimb; P3 = third phalanx

Case 3: moderate paronychia of digit four of the right forelimb. Local inflammation and exudation are noted

Case 3: severe paronychia of digits 3 and 4 of the right forelimb. Marked ulceration and inflammation is present, exposing the bone of the third phalanx of digit 4

Case 3: distal phalanx (haematoxylin and eosin stain). The red dashed line outlines the entire profile of the distal phalanx, although the ungulate process (UP) was not sampled within the tissue section. The blue dashed lines outline the keratin claw (KC) and second phalanx (P2). Bone with cartilage of the retained primary spongiosa is particularly abundant in the extensor process (EP) and flexor tubercle (FT)

Case 3: distal phalanx (haematoxylin and eosin stain). The structure of osteopetrotic bone was characterised by cartilage (C) irregularly intermingled with bone (B). In this area of osteonecrosis, spaces that would normally contain fibrovascular tissue are occupied by necrotic debris (N) and inflammatory cell infiltrates (arrows)
Case 4
A neutered female 2-year-old DSH cat, located in the USA (number 210 in the database), was presented with a right patellar fracture. A chronic left patellar fracture and multiple persistent deciduous teeth were noted. At approximately 2 years of age, paronychia was first noted of digit one of the left forelimb and digits one and three of the right forelimb. For 14 months symptomatic treatment was trialled, involving a total of nine antibiotic courses. Culture and sensitivity were performed three times. A total of seven digits on only the forelimbs were affected. Radiographs were performed (Figure 9). The bones in both thoracic limbs showed a heterogeneous slight increase in bone density. For treatment details, see Figure 10 and Table 6. Owing to recurrent infection and discomfort, the third phalanx of all forelimb digits was amputated. During surgery, osteomyelitis was suspected owing to disintegration of the phalanges during the procedure. The amputated digits were placed in neutral buffered formalin and submitted for histopathological evaluation with routine processing and staining (haematoxylin and eosin). Each of the examined phalanges had abnormal organisation of bone that was characterised by hyaline cartilage intermingled with both mature lamellar bone and unmodelled amorphous bone (Figures 11 and 12). The overall density of bone was increased – no marrow tissue was present and intertrabecular vascular spaces were largely obliterated by cartilage or bone. At least two of the phalangeal bones had areas of suppurative inflammation, consistent with osteomyelitis (not shown). Five months after surgery the patient had recovered well and, as of the time of writing, the hindlimb nailbeds continue to show no sign of paronychia.

Case 4: radiographs performed as part of further investigations of paronychia. A heterogeneous slight increase in bone density was noted. An intravenous catheter was placed in the left cephalic vein. Marked soft tissue swelling was noted at digit one of the left forelimb and digit four of the right forelimb

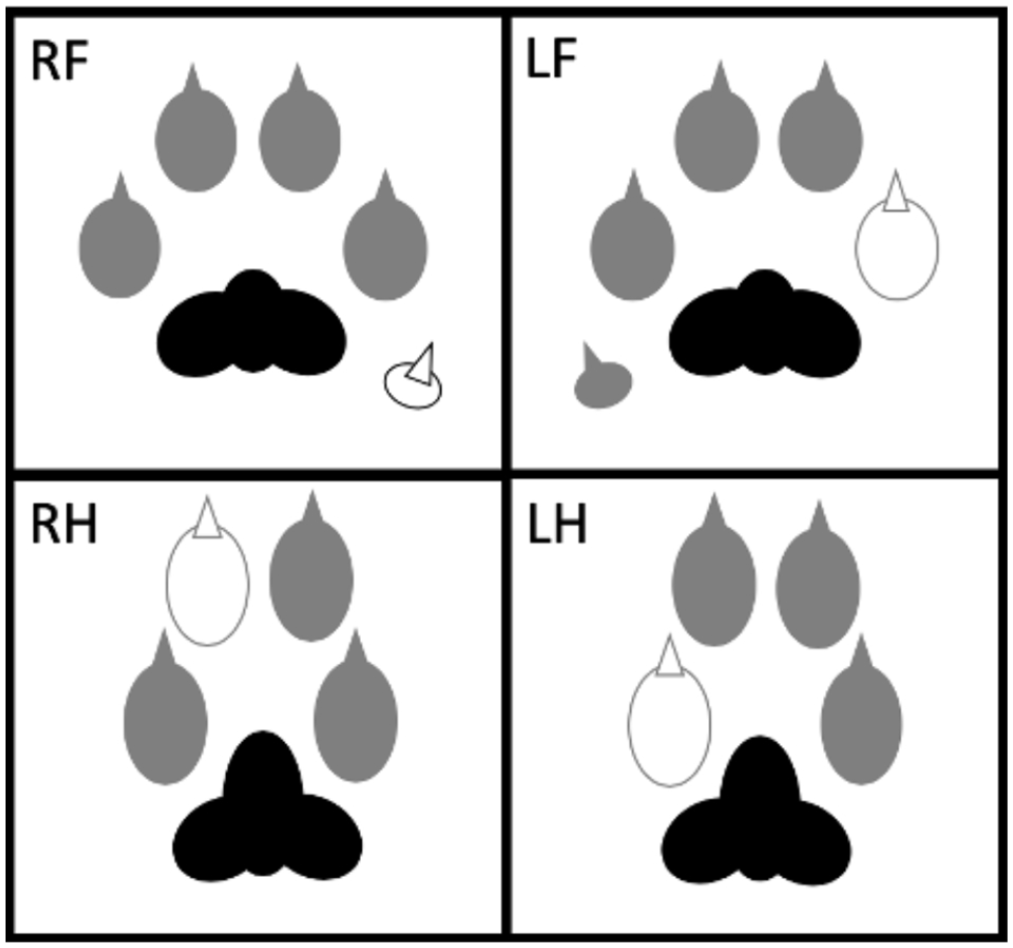
Digits affected by paronychia in case 4, patient number 210. RF = right forelimb; LF = left forelimb; RH = right hindlimb; LH = left hindlimb; black = not affected; dark grey = amputated; white = amputated, not affected
Detailed description of paronychia treatment of case 4, patient number 210
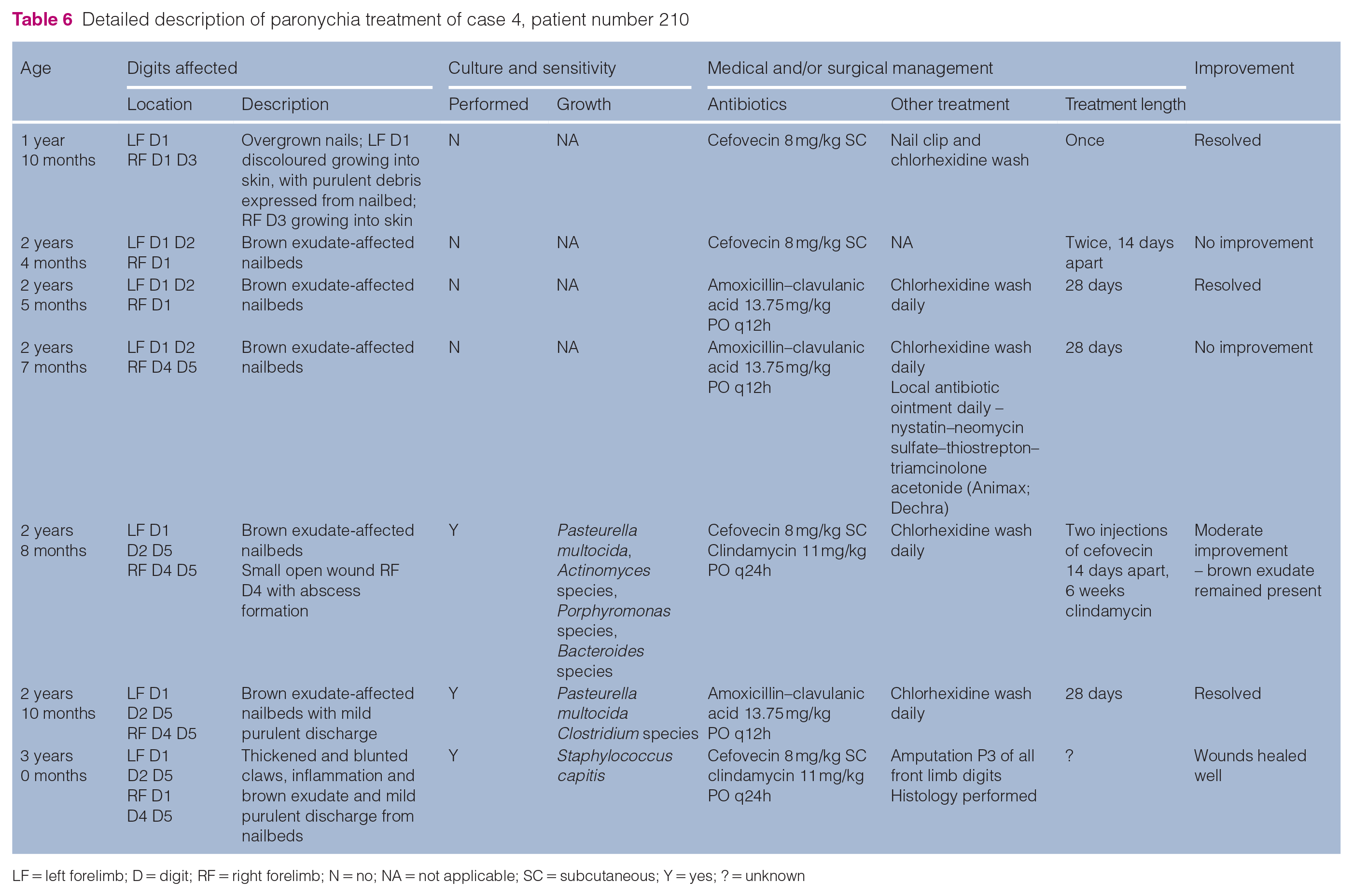
LF = left forelimb; D = digit; RF = right forelimb; N = no; NA = not applicable; SC = subcutaneous; Y = yes; ? = unknown

Case 4: distal phalanx (haematoxylin and eosin). A section from a relatively less affected digit has trabecular bone throughout most of the distal phalanx, although the extensor process (EP) has finely textured osteopetrotic bone with abundant cartilage. KC = keratin claw; P2 = second phalanx; UC = unguicular crest; FT = flexor tubercle

Case 4: distal phalanx (haematoxylin and eosin). Hyaline cartilage (C) is intermingled with bone (B), which includes both mature lamellar bone and unmodelled amorphous bone. The true density of bone is not apparent and clear space separating islands of cartilage and bone is an artefact of processing
Case 5
A 1-year-old neutered male DSH cat, located in the USA (number 215 in the database), presented for the extraction of deciduous teeth. Within a couple of months it sustained patellar fractures. At approximately 1.5 years of age paronychia was noted of the left hindlimb (digit unknown). For over 20 months the cat was medically managed with empirical and culture-based (performed once) antibiotics. A total of seven antibiotic courses were prescribed. Immunosuppressive medication was trialled. Treatments were sometimes successful; however, relapse of paronychia was common. All four limbs and a total of 14 digits were affected at some time period. For treatment details, see Figure 13 and Table 7. Owing to relapse and discomfort, amputation of P3 of all digits at 3 years of age was performed. At 10 years of age the cat sustained a right tibial fracture. At 11 years of age the cat was reported to be doing well and no further issues relating to the toes had occurred.
Digits affected by paronychia in case 5, patient number 215. RF = right forelimb; LF = left forelimb; RH = right hindlimb; LH = left hindlimb; black = not affected; dark grey = amputated; white = amputated, not affected
Detailed description of paronychia treatment of case 5, patient number 215

LH = left hindlimb D = digit; ? = unknown; NA = not applicable; LF = left forelimb; RF = right forelimb; RH = right hindlimb; N = no; P3 = third phalanx; SC = subcutaneous; Y = yes
Discussion
Paronychia in cats with PADS has not previously been reported. Chronic paronychia is an additional clinical feature of PADS. Besides patellar fracture and deciduous teeth, mandibular and maxillary abnormalities and other fractures have been reported in cats suffering from PADS.1–5 All cats included herein had patellar fractures and persistent deciduous teeth. Three of the five cats sustained other non-traumatic fractures in their life. All five cats had persistent nailbed inflammation, with recurrent infections. Antimicrobial therapy with or without non-steroidal anti-inflammatory drugs were trialled, which would often lead to temporary or no improvement of clinical signs. All cats had multiple digits of multiple limbs affected and eventually underwent amputation of the third phalanx of one or multiple digits.
Paronychia caused by bacterial infection can successfully be treated with antibiotics. If paronychia is unresponsive or relapses occur following a course of antibiotics, further investigations should be performed to identify the underlying disease, such as culture and sensitivity, dermatophyte culture, skin scrapes, cytological examination and/or nailbed biopsy. 8 This was not always performed in the cases reported herein, and antibiotics were readily used without the benefit of culture and sensitivity results. Antibiotic prescribing was not always used according to the guidelines of the cascade and the authors strongly recommend the guidelines are followed to minimise the development of antibiotic resistance.
In challenging cases of paronychia or cats with severe discomfort, onychectomy can be performed as treatment and to assist in obtaining a definitive diagnosis. 12 Owing to the invasiveness of this procedure, it should only be considered for cats with recurrent and/or severe signs that do not resolve with medical management. In all the PADS cats reported herein, their signs could be considered recurrent, severe and non-responsive to medical management for the majority of the affected digits. A total of 36 digits were affected in this study, 17% (n = 6/36) resolved with medical management and 83% (n = 30/36) were treated successfully by amputation. Based on our study, we cannot conclude why paronychia sometimes resolved with medical management. It could be because of insufficient follow-up, or because of a different underlying pathology. Amputation should only be considered once medical management with investigations and proper use of antimicrobials, analgesia and topical treatment have failed.
Histopathological results were available for affected digits from two of the cats in this study (cases 3 and 4). These revealed abnormal bone of the distal phalanx with retention of cartilage. Both of these cats also had at least one digit in which neutrophilic inflammation involved digital bone, causing osteomyelitis with variable osteolysis and osteonecrosis, loss of the cornified claw sheath and/or ingrowth of nailbed epithelium. Based on these findings it could be speculated that persistent paronychia in cats with PADS involves break down of usual anatomical barriers to infection, particularly on the palmar/plantar aspect of the ungulate process of the distal phalanx. Underlying abnormal bone structure could render bone less likely to respond favourably to antimicrobial therapy, although a specific mechanism is not clear.
Research regarding the process and origin of PADS is ongoing. It is suspected that cats with PADS suffer from insufficiency fractures, where fractures occur when abnormally weakened bone is loaded normally. It has been postulated that these cats may have an underlying primary bone disorder. Primary bone modelling is suspected to be abnormal, and the abnormality is exacerbated in bones with a higher rate of remodelling. One of the affected cats had a generalised and marked increase in bone density on radiographs, throughout its skeleton, a phenomenon known as osteopetrosis. 1 The presence of cartilage within the distal phalanges of cats in this study also supports a form of osteopetrosis that is characterised by cartilage remnants of the primary spongiosa. Osteopetrosis has been well described in humans. 14 It is a rare genetic disorder where patients have an increase in bone density due failure of bone resorption, specifically, a defect in osteoclast activity.14–16 Patients suffer from persistent deciduous teeth, pathological fractures and osteomyelitis.14,16 Depending on the form and severity of their disease, they are at increased risk for infections owing to, among other factors, impaired vascularity, anaemia and leukopenia. 17 Osteopetrosis leads to poorly developed bone marrow causing anaemia, pancytopenia, osteomyelitis and sepsis.4,14,18,19
Limitations of this case series are the small number of cases, the retrospective nature and variability of acquisition of information based on owner perception and clinical notes, particularly the specific digits involved.
Conclusions
Chronic paronychia is an additional clinical feature of PADS and the probable mechanism involves poor integrity of osteopetrotic bone, loss of normal nailbed anatomy and secondary osteomyelitis of the distal phalanx. A prospective study is warranted to document the frequency of paronychia in PADS and to investigate the pathogenesis further. In any cat with atraumatic patellar fractures and/or retained deciduous teeth, it is recommended to pay specific attention to the nailbeds. These lesions are commonly chronic in appearance and do not respond well to medical management. When medical management is instituted, antibiotics should be used according to the cascade and ideally following appropriate investigations to determine the cause. Amputation is not recommended as a first-line treatment and appropriate investigation and medical management of paronychia is recommended. Amputation should, however, be considered for cases where paronychia is unresponsive to medical management.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article’
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognised high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee was therefore not specifically required for publication in JFMS.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.