
Abstract
Practical relevance:
The ability to recognize, diagnose and treat corneal disease is essential for maintaining vision and comfort in feline patients. Being able to correctly identify appropriate techniques for surgical cases is of particular importance for success when performing corneal surgery.
Clinical challenges:
Many different corneal diseases present with similar clinical signs, and it can be hard to determine the appropriate treatment for individual patients. It is essential for the clinician to understand the indications for corneal surgery, instrumentation needed and microsurgical principles prior to attempting these procedures. The prognosis following surgery and potential complications should be discussed with the client.
Audience:
This review article aims to assist in decision-making and to provide detailed guidance for primary care clinicians considering referral of cats for corneal surgery. The review outlines common feline corneal diseases and associated surgical therapies performed by veterinary ophthalmologists, highlighting appropriate instrumentation and case selection. Some surgeries are explained in depth for ophthalmologists and residents in training.
Equipment:
Although some procedures may be performed with common surgical equipment and supplies, most require specialized ophthalmic instrumentation and expertise, which entails significant microsurgical training and practice, as well as financial investment. Most of the procedures require an operating microscope for the best surgical outcomes; however, surgical loupes may be sufficient in some cases. Evidence base: This review article compiles information from many published references on feline corneal diseases and surgeries, complemented by the experience of the authors.
Brief review of corneal anatomy and ophthalmic examination in the cat
Most feline corneal conditions, including feline keratitis (one of the most common), can be readily diagnosed with a thorough ophthalmic examination. Briefly, vision testing, neuro-ophthalmic evaluation, adnexal and anterior segment examination, Schirmer tear test, tonometry, fluorescein staining and fundic examination should be performed on all patients presenting with ophthalmic clinical signs. Once a list of problems and possible diagnoses has been formulated, therapeutic planning can begin.
Before performing corneal procedures and surgeries in cats, it is vital to review and understand the anatomy of the feline cornea. This is an avascular structure that consists of four main layers: epithelium, stroma, Descemet’s membrane and endothelium. The epithelium, Descemet’s membrane and endothelium are relatively thin, while the stroma makes up approximately 90% of the corneal thickness. The cornea tends to be thickest in the periphery and thinnest in the center, which is a very important principle to consider when performing corneal surgery. Depending on the method used for measurement, central corneal thickness in the cat typically ranges from 0.4 to 0.6 mm. 1
The innervation of the feline cornea is also important to understand when treating corneal disease. The ophthalmic division of the trigeminal nerve gives rise to the long ciliary nerves, which innervate the cornea. These nerves are more numerous in the anterior cornea and, therefore, superficial corneal disease may be more painful than deep corneal disease. 2 Regardless, adequate analgesia and topical anesthesia are imperative when performing corneal surgery, which always has the potential to be painful.
Proparacaine and tetracaine are the most commonly used topical anesthetics in veterinary ophthalmology, and some procedures can be performed using only topical anesthesia. Additionally, it is important to remember that corneal surgery itself may lead to disruption of the long ciliary nerves and may therefore cause decreased corneal sensitivity. When corneal sensitivity is affected, the patient is not stimulated to blink normally, which can lead to inadequate spread of the tear film and drying of the ocular surface. Eventually this can cause corneal ulceration (neurotrophic keratitis) and possibly other undesirable sequelae such as corneal sequestrum formation.

Feline corneal disease: when is surgery indicated?
There are several disease processes for which corneal procedures and/or surgeries may be indicated. A brief overview of each disease is provided below, while a number of the procedures themselves will be described in a later section. These descriptions are intended to assist primary care clinicians in determining what disease process is occurring and to develop a proper understanding of the procedures to relay to clients. From there, the clinician can determine whether referral for surgery is indicated. Important considerations when recommending corneal surgery are described in the box. These surgeries should be performed by specialists who have adequate knowledge and training in microsurgical techniques.
Keratitis
Keratitis is one of the most common ophthalmic issues seen in the feline patient. The condition is typically characterized as ulcerative or non-ulcerative, and there are several underlying causes for both types of corneal inflammation. This review article focuses primarily on ulcerative keratitis, which warrants surgical intervention more commonly than non-ulcerative keratitis.
Ulcerative keratitis is typically the result of a primary ocular disorder or an external inciting cause, including, but not limited to: feline herpesvirus (FHV-1), incomplete or inadequate eyelid closure, tear film instability, foreign bodies, bacterial conjunctivitis and adnexal disease (eg, entropion, eyelid agenesis, lagophthalmos). 3 These underlying conditions predispose the cornea to ulceration and, from there, the ulcer may be defined in several ways. Some ulcers remain superficial and sterile, and may heal within a few days with no intervention, although it is usually recommended that any corneal ulcer is treated with prophylactic topical antimicrobials to prevent infection. If the corneal ulcer persists after 1 week, it is then classified as indolent, or non-healing. It is important to note that any ulcer can become indolent, and this should not be confused with a spontaneous chronic corneal epithelial defect (SCCED), a specific type of indolent ulcer seen in dogs that has a unique patho-physiology and treatment.
Indolent ulcers are common in brachycephalic cats and are often related to FHV-1 infection. Adnexal disease, trauma and corneal dystrophy may also lead to persistence of a corneal ulcer. Typically, indolent ulcers are treated with topical antimicrobials and a cotton swab epithelial debridement. If an underlying cause for the ulcer is found (FHV-1, adnexal disease, foreign body), this should also be treated to promote healing of the ulcer. 4 Although cotton swab epithelial debridement is commonly performed in conjunction with grid keratotomies and/or diamond burr debridement in canine patients with SCCED, grid keratotomies may predispose cats to corneal sequestration and should not be performed. 4
A case series describing superficial lamellar keratectomy for the treatment of refractory corneal ulcers in 36 cats reported variable results for healing. 5 A 2019 abstract described the use of diamond burr debridement for non-healing corneal ulcerations, with or without corneal sequestra, in nine cats. 6 In this report, all cats were fluorescein negative at the last recheck examination, and corneal brunescence was absent or decreased in eyes with concurrent sequestra. No complications were reported at follow-up (obtained after varying amounts of time) in this small group of cats. 6 Based on this abstract, diamond burr debridement may be a therapeutic option in cats with non-healing corneal ulcers, but practitioners should use this modality with caution.

Corneal ulcers that have progressed beyond the epithelium may be characterized as anterior stromal, mid-stromal, deep stromal or descemetocele. Corneal perforations may occur quickly once the ulcer deepens, and surgical intervention is often recommended for deep ulcerative keratitis to preserve vision and/or the globe. In the authors’ experience, if the ulcer is infected or malacic, 24-48 h of intense antimicrobial and antiprotease treatment, as described by Maggs et al, 7 may encourage better outcomes.
Many techniques for surgical repair of deep ulcerative keratitis or corneal perforation have been described in domestic species; however, the basic principles of these grafting procedures are similar regardless of the species or type of graft being performed. The purpose of a grafting procedure is to provide tectonic support and vascularization to the cornea to facilitate healing. Although some deep stromal ulcers or descemetoceles will heal with medical management, the healing time may be longer, the ulcer may heal with less stroma leading to a weakened area of cornea (corneal facet or divot) or the ulcer may perforate during healing. Corneal surgery is often recommended for these reasons.
For deep ulceration without corneal perforation, a single grafting procedure (conjunctival pedicle flap, corneoconjunctival transposition [CCT]) will typically suffice to provide tectonic and vascular support (Figure 1). For corneal perforations, several tissues have been used alone or in conjunction with conjunctival grafts to provide additional support to the cornea. In general, these materials are trimmed to the same size or just slightly bigger than the defect and are sutured into the defect to stabilize the cornea and create a seal before placing an additional graft if necessary. In the feline patient, the following grafting materials have been described for corneal reconstruction, with variable results: homologous and heterologous lamellar and penetrating transplants with frozen or fresh feline cornea (corneal transplant),8,9 porcine bladder,10-14 porcine small intestinal submucosa (SIS),10-12,15,16 bovine pericardium 17 and equine amniotic membrane. 18 Although not reported in cats specifically for corneal perforation, CCT has been successfully performed in dogs with full-thickness corneal defects. 19

(a) Descemetocele in a 14-year-old male neutered domestic shorthair cat that presented with severe feline herpesvirus keratitis. (b) Postoperative conjunctival pedicle graft at 4 weeks. Note the graft is becoming incorporated within the cornea and the sutures are dissolving. The cornea surrounding the graft is clear
Corneal sequestrum
Corneal sequestration is a condition characterized by accumulation of pigment in the cornea in conjunction with corneal stromal collagen degeneration (Figure 2; see also the case notes on page 12). Cats with FHV-1 infection and brachycephalic cats tend to be pre-disposed.20,21 Corneal sequestra can vary in size, shape, location and depth, and surgical intervention is the preferred treatment to remove the lesion.

(a) Four-year-old Persian cat with corneal sequestrum and corneal vascularization; (b) 1 week postoperatively following a penetrating keratoplasty for sequestrum removal; (c) 2 weeks postoperatively; (d) 2 months postoperatively; and (e) 1 year postoperatively. Courtesy of Ellison Bentley, University of Wisconsin-Madison
Numerous procedures have been described in the treatment of this unique feline condition, including: superficial lamellar keratectomy alone or with a bandage contact lens; 20 lamellar keratectomy with cyanoacrylate adhesive; 22 lamellar keratectomy with porcine small intestinal submucosa graft;10,16,20 lamellar keratectomy with amniotic membrane; 23 lamellar keratectomy with CCT;24-26 lamellar keratectomy with conjunctival flap (pedicle, 360°, hood); 20 lamellar keratectomy with bovine pericardium; 17 heterologous penetrating keratoplasty; 27 and fresh and frozen homologous and heterologous lamellar keratoplasties.8,28,29 These procedures produce variable results depending on the size and depth of the corneal sequestrum. In the authors’ experience, superficial keratectomy alone or superficial keratectomy with a conjunctival flap or CCT are successful in most cases. Corneal clarity varies depending on the procedure, but CCTs have been associated with less scarring. 25 When removing the sequestrum, it is important to remove all discolored, abnormal tissue, or recurrence is likely. A study of 97 cats (109 eyes) noted that 28.9% of cases of unilateral sequestrum eventually developed a sequestrum in the contralateral eye. 25
Dermoids
Dermoids, or choristomas, can occur in cats, specifically Burmese and Birman breeds. They are congenital defects defined as benign masses of cytologically normal, typically haired, skin cells in an abnormal location. In feline patients, dermoids are commonly located temporally (laterally) and may involve the eyelid margin, skin, bulbar conjunctiva or a combination of these structures. Dermoids do not affect vision if they do not involve a large portion of the cornea, but they can be uncomfortable and can cause secondary issues such as keratitis or difficulty blinking.30,31
Surgical excision is often curative for dermoids of the cornea, conjunctiva or adnexa. 30 If the dermoid involves the cornea, a lamellar keratectomy must be deep enough to ensure removal of all skin, including hair follicles, to prevent recurrence. 32 If the dermoid involves the adnexa, an appropriate corrective eyelid (blepharoplasty) procedure may be needed after removal of the dermoid.
Feline acute corneal hydrops
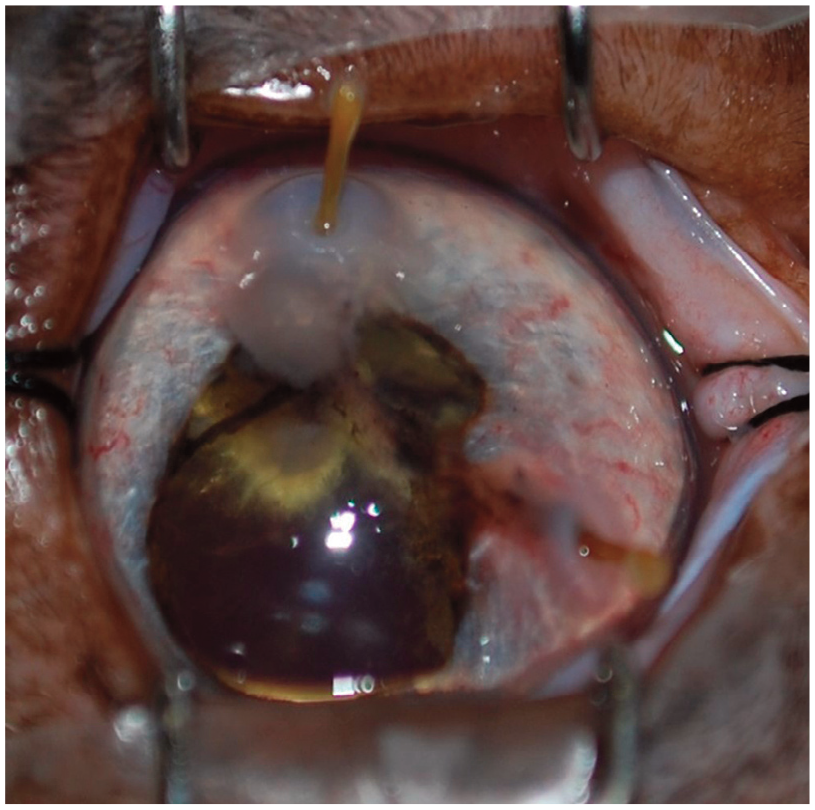
Feline acute corneal hydrops, also known as feline acute bullous keratopathy, is a unique condition of the feline cornea characterized by an acute onset of a focal, geographic or complete area of stromal fluid accumulation (corneal hydrops) (Figure 3). 33 This condition is simple to diagnose, as the cornea is visibly abnormal with marked edema and protrusion, particularly notable when examined from the side. The edema accumulation is thought to be caused by acute Descemet’s membrane rupture.34,35 Although an underlying etiology has not been identified for this condition, there is research to suggest an association with systemic ciclosporin administration. 34 Left untreated, this condition can lead to corneal rupture, loss of vision and ultimately loss of the eye.

Two-year-old male neutered Siamese cross that presented with an acute onset of corneal edema and distortion (curvature) of the corneal surface. This cat was diagnosed with feline acute corneal hydrops and a third eyelid flap was performed with a good outcome
Although various surgical procedures, including superficial keratectomy, conjunctival pedicle graft 34 and penetrating keratoplasty with corneal transplant,8,34 have been performed successfully, nictitating membrane flaps (also called third eyelid flaps) have been reported to have a 90.5% success rate when used alone or in conjunction with a grafting procedure for treatment of feline acute corneal hydrops.33,34
Neoplasia
Because the cornea is an avascular structure, corneal neoplasia is considered rare. Still, pathologic changes including vascularization, chronic inflammation and exposure to ultraviolet radiation can lead to formation of squamous cell carcinoma (SCC), hemangioma and hemangiosarcoma, and these tumors have been documented in the feline cornea or at the limbus.36-39
Owing to the aggressive nature of corneal SCC in cats, enucleation or exenteration is typically recommended,36,37 although a lamellar keratectomy may be performed before considering eye removal to confirm diagnosis. In a 2013 case report of corneolimbal SCC in two cats, both animals’ affected eyes were removed before any surgical therapies could be instituted. 36
Although not documented in cats, there are case reports describing lamellar keratectomy followed by cryotherapy, topical chemotherapy with mitomycin C 40 and/or strontium-90 beta radiation for corneal SCC in canine and equine patients; results have been variable. 41 Use of 5-fluorouracil as pulse or monotherapy has also been reported in canine patients.42,43 Although mitomycin C has been used in the treatment of other tumor types in cats, 44 the safety of treatment with this agent in cats is extremely variable and, as such, it should be used with extreme caution. 5-Fluorouracil is contraindicated for use in cats.
There are few reports of corneal vascular tumors (hemangiosarcoma and hemangioma) in cats.38,39 In a 2011 case report, Cazalot and colleagues performed a lamellar keratectomy to the mid-stroma followed by superficial diathermy and a nictitating membrane flap for management of a hemangiosarcoma. The histopathology showed complete margins, but the mass eventually regrew, and the owner ultimately elected enucleation. Based on this report, enucleation may offer the best chance for non-recurrence. 38
Traumatic corneal disease
Traumatic corneal injuries are not uncommon in domestic species (small animals, as well as equine, bovine and other livestock species) and can range in severity from a superficial linear laceration to a full-thickness corneal perforation that may or may not involve the lens. In most scenarios, feline corneal lacerations are caused by cat claws or foreign bodies. In one 2017 study by Braus and colleagues, all six cats suffering corneal and lens lacerations lived an indoor/outdoor lifestyle; 45 thorn injury was the documented cause of 3/6 injuries (Figure 4) and the remaining three injuries had unidentified causes. 45
Two-year-old spayed female domestic shorthair cat that presented with a cactus thorn penetrating the cornea, iris and lens. The pupil was dyscoric (abnormally shaped) and a cataract was forming at the penetration site in the lens. The injury had been present for at least 3 days. The thorn was removed carefully, and the wound was closed primarily. In cases of ocular trauma, such as this, the cat may develop an ocular sarcoma, and so the patient should be monitored closely for ocular changes
For superficial, uncomplicated traumatic corneal injuries, corneal cytology and/or corneal aerobic culture and sensitivity testing should be performed following a full ophthalmic examination. Medical management with appropriate topical antimicrobials, with or without topical mydriatics and systemic anti-inflammatories, should suffice for treatment. If initial medical therapy is not successful, surgical intervention may be considered.
Corneal lacerations/injuries that involve more than 50% of the stroma and/or are full thickness through the cornea almost always require surgical correction to preserve vision and/or the globe. If the laceration is linear and uncomplicated with no incarcerated uveal tissue, the defect may be closed primarily. Depending on tissue apposition and stability of the wound, a conjunctival graft may be indicated. The most common type of graft used for long, linear lesions is a bridge (bipedicle) graft.
In severe cases, penetrating corneal injuries may also involve the lens. Lens capsule rupture can lead to severe phacoclastic lens-induced uveitis and these injuries should be treated promptly for the best outcomes. Phacoemulsification in conjunction with corneal repair is typically recommended when the lens injury is greater than 1.5 mm in diameter. 45 The six cats in the aforementioned study by Braus et al had a favorable outcome following combination surgery for corneal and lens lacerations. Although follow-up time was less than 1 year, all cats were visual at the last recheck examination. 45 Outcomes appear to be more variable in canine patients. 45
It is important to monitor feline eyes with a history of trauma because it has been suggested that severe ocular trauma and/or lens surgery can lead to formation of feline ocular post-traumatic sarcoma. Tumor formation can occur even years after the inciting event. 46
Preoperative and anesthetic considerations, instrumentation and set-up
Preoperative considerations
As with any surgical procedure, it is essential to consider the overall health of the patient and perform a comprehensive preanesthetic work-up. Depending on the patient’s age and comorbidities, this typically consists of a thorough physical examination, heart and lung auscultation, and a complete blood count and serum biochemistry panel at a minimum.
Once the patient is deemed a good anesthetic candidate, it is important to prepare the client for potential risks and complications of the chosen procedure. In the authors’ experience, it is valuable to appropriately manage owner expectations at the beginning of treatment, especially if the prognosis for vision or globe retention is questionable, or if recurrence is possible.
Important surgical and anesthetic principles
For most of the procedures discussed below, general anesthesia is required, with varied systemic and topical therapeutic protocols following surgery. For the purpose of this discussion, the reader can assume the patient is systemically healthy. If the patient has underlying conditions, consultation with appropriate specialists is recommended, and the anesthesia protocol can be adjusted accordingly. The authors’ intention is to provide some helpful hints regarding anesthesia, but readers should note that full discussion of anesthetic protocols and drug mechanisms is beyond the scope of this article and relevant texts should be consulted for further information.
Once the patient is placed under anesthesia, appropriate ‘rough’ (non-sterile) and sterile preparation should be performed using dilute iodine solution (1:50) and sterile saline (see box on page 7). It is important to note that chlorhexidine should never be used in or around the eye due to its potential toxic effects. Individuals performing presurgical preparation should use extreme caution when manipulating the patient’s head and eye, as many of the diseases described result in a fragile cornea.
Upon moving to the surgical suite, proper head positioning is a critical step in assuring adequate visualization of the cornea. Most surgeons place the patient in dorsal or lateral recumbency and use a vacuum pillow (Figure 5) to ensure precise head positioning. The cornea should be oriented parallel to the table and facing the ceiling. The surgeon should be mindful of the endotracheal tube when manipulating the head and neck. Placing a wire-guarded endotracheal tube can prevent airway occlusion and inappropriate extubation during complicated positioning. The surgeon should have a comfortable chair, preferably with arm rests, and adjust the chair and table height accordingly to ensure proper surgical positioning and technique.

(a) Vacuum pillow; (b,c) vacuum pillow with patient’s head properly positioned in dorsal recumbency. Note the use of a guarded endotracheal tube, which is important when positioning patients in this manner

Top center: stainless steel surgical sponge bowl with 4 x 4 gauze. Top row of instruments, left to right: wire (Barraquer) eyelid speculum, 0.12 mm Colibri-style forceps, straight tying forceps, curved tying forceps, left corneal section scissors, right corneal section scissors, non-locking curved microneedle holders (spring-handled), Beaver blade handle with number 64 Beaver blade directly above, 0.3 mm Bishop-Harmon forceps. Bottom row of instruments, left to right: Stevens tenotomy scissors, 0.3 mm Colibri forceps, 0.3 mm fixation forceps, Westcott tenotomy scissors, Vannas scissors, Martinez corneal dissector, Westcott stitch scissors

Appropriate magnification (x 4 to x 10) is essential for corneal procedures and can be achieved with a surgical microscope or surgical loupes of high optical quality. 47 While surgical loupes may be sufficient for skilled surgeons to perform routine corneal surgery in select cases, a surgical microscope is the gold standard, and is a definite requirement for more complicated procedures (as noted, where relevant, in the following discussion).
Another important principle of corneal surgery is adequate irrigation of the cornea throughout the procedure. Sterile balanced salt solution is commonly used for this purpose. Irrigation of the cornea prevents corneal drying, which can cause corneal erosions, and also promotes optimal tissue handling and visualization. A few drops of irrigating solution can be applied to the cornea approximately every 30 s during the procedure, or more frequently for patients with tear film disorders. 47
Lastly, a neuromuscular blocking agent may be necessary to relax the extraocular muscles, and thereby decrease tension on the fragile globe and provide maximal visualization of the cornea. These medications paralyze the entire patient, and mechanical ventilation is needed for the duration of the medication’s action. 47 In addition to neuromuscular blockade, one or two stay sutures of 4-0 to 6-0 silk can be placed in the episclera at the 12 or 6 o’clock position to help with visualization, if needed.

Corneal procedures
General ophthalmic principles
Although each procedure varies slightly depending on the patient, some general surgical principles apply in terms of fixating, incising and suturing the cornea.
Broadly speaking, incising an intact globe with normal intraocular pressure is easier than incising a perforated globe with low intraocular pressure because the intraocular pressure dictates the stabilization of the globe. Therefore, if the intraocular pressure is low or the eye is leaking aqueous humor, the surgeon will need to fixate immediately next to the incision to make an appropriate cut. 47
General handling principles apply when suturing the cornea; however, it is extremely important to place corneal sutures at an appropriate depth (approximately 75-90% of the corneal stroma) to achieve a watertight seal with no gaping of the wound. Additionally, sutures should be placed approximately 1-2 mm from the wound edge and should be symmetric on both sides of the wound. When placing a suture, the needle should be grasped at the midpoint and directed so that it enters the cornea
perpendicularly. The curve of the needle should be followed while using fine motor movements to propel the needle through the stroma until the needle emerges from the cornea. 47
Lamellar keratectomy
✜
✜
✜
A lamellar keratectomy involves incising and removing the cornea at variable depths, which will always result in removal of the epithelium and some of the underlying stroma.
To begin, a number 64 Beaver blade (brush cutter blade) is used to outline the abnormal portion of the cornea to an appropriate depth that will remove the lesion. If stay sutures have been placed, gentle traction can be applied to the appropriate suture as a point of fixation. Alternatively, the globe can be fixed using Bishop-Harmon forceps or 0.3 mm fixation forceps. Depending on subsequent procedures (ie, conjunctival pedicle graft, lamellar keratoplasty), a square or circular incision may be made (square for the former, circular for the latter). After the area has been outlined, 0.12 mm Colibri forceps are used to grasp and elevate the edge of the cornea being removed. Carefully, a number 64 Beaver blade is used to dissect the corneal lamellae (Figure 7). After this incision is started, a Martinez corneal dissector is used to continue the dissection within the same lamellar plane. If the surgeon chooses to continue sharp dissection with the Beaver blade, it is more difficult to keep the blade in the same plane of dissection; gentle traction of the cornea being removed will allow for controlled dissection in the same plane. The Beaver blade or corneal dissection scissors can be used to complete the keratectomy on the remaining side. If diseased cornea remains (ie, brunescence from sequestrum or suspected neoplasia), the same procedure can be carefully repeated until corneal clarity is seen. Note that maintaining consistent depth with multiple keratectomies can be challenging.

Superficial lamellar keratectomy being performed. The surgeon had already outlined the area to be removed and here used 0.12 mm Colibri forceps (right) to grasp and elevate the edge of the cornea being removed. The number 64 Beaver blade (left) was used to dissect the corneal lamellae
In general, a grafting procedure that provides tectonic support is recommended if the excised portion of cornea is 50% depth or more.
Corneal laceration repair
✜
✜
✜
The method chosen to repair a corneal laceration largely depends on the extent of the lesion. For relatively uncomplicated linear corneal lacerations greater than 50% stromal depth, the wound may be closed primarily in a simple interrupted pattern with 7-0 to 9-0 absorbable suture material. Other suture patterns, such as simple continuous and shoelace, have also been described, though the authors’ preference is simple interrupted. Tissue apposition is of utmost importance, and special care should be taken to ensure sutures are not too loose or overtight. The first suture should be placed in the middle of the wound, and subsequent sutures should be placed at each end of the wound. From there, simple interrupted sutures should be placed according to the ‘law of bisection’; in other words, the sutures should be placed in the middle of each section until all sutures are approximately 1 mm apart. It is common that the initial sutures loosen as the wound is closed and tension becomes evenly distributed; these initial sutures may need to be replaced once the wound is mostly closed if this occurs. A bipedicle conjunctival graft may be indicated for full thickness wounds to provide tectonic and vascular support.
For corneal lacerations that involve uveal prolapse, the prolapsed tissue should be replaced into the anterior chamber when possible. This typically can be accomplished by tamponading the tissue back into the anterior chamber using an iris spatula and viscoelastic material (hyaluronic acid, methylcellulose) while suturing the wound. Successful repair is still achievable, but anterior synechiae are likely in these cases.
Conjunctival grafts
✜
✜
✜
Conjunctival autografts have been described in various patterns (pedicle, bridge, hood, 360°, tarsopalpebral, free island) for
treatment of many corneal diseases in dogs, cats and horses. The following discussion focuses on conjunctival pedicle grafts, which are the most frequently used corneal grafts in cats. These grafts are harvested from the bulbar conjunctiva most commonly or, occasionally, from the palpebral conjunctiva. They provide vascular and structural support to the cornea for deep ulcerative keratitis or following lamellar keratectomy.
After the patient is positioned in dorsal recumbency, a keratectomy (described above) or debridement of epithelium from the wound edge is performed to encourage graft adhesion. Calipers can be used to measure the size of the lesion and the distance from the limbus to the distal edge of the lesion to ensure appropriate width and length of the graft. Colibri forceps (0.3 Pierse) and blunt-tipped Stevens tenotomy scissors or Westcott tenotomy scissors are used to harvest the donor bulbar conjunctiva, most often from the superior temporal quadrant. Carefully, a small snip is made with tenotomy scissors in the conjunctiva approximately 1-2 mm from the limbus. The edge of the cut conjunctiva is lifted carefully with Colibri forceps and the scissors are inserted. The conjunctiva is carefully dissected from underlying Tenon’s capsule using blunt and sharp dissection, taking special care to keep the tips of the scissors up. The graft should remain thin, and the surgeon should be able to clearly see the tips of the scissors through the conjunctiva.
Next, the graft is incised approximately 1 mm from the limbus for the length of the graft, taking care to remove any Tenon’s capsule from underneath. The following incision is approximately 90° to the first incision toward the fornix and should be about 1-2 mm wider than the measured defect. The final incision is parallel to the first incision, creating the pedicle that will be rotated onto the cornea. It is important that the graft has no traction at the base and that the base is as wide as, or wider than, the tip to decrease the risk of necrosis. Any portion of the distal graft that is grasped during harvesting may need to be transected to discourage necrosis.
Cardinal sutures should be placed, first through the graft and then through the edge of the defect (see discussion of suturing principles on page 8). After the simple interrupted cardinal sutures have been placed, the remaining graft can be secured using simple interrupted sutures or by oversewing a simple continuous suture. Most surgeons use 8-0 or 9-0 absorbable suture material for conjunctival grafts in cats. A limbal tacking suture can be placed to relieve tension, and the conjunctival defect may be closed if the surgeon deems it necessary. 47
Lamellar keratoplasties
✜
✜
✜
The most common lamellar keratoplasty used for feline corneal disease is the CCT. The following discussion focuses on this type of graft, which includes the anterior stroma and epithelium and is autologous. Although CCTs have been described for numerous corneal diseases, the basic indication for using this graft is a deep axial defect with sufficient clear cornea to transpose into the recipient bed.
To begin, diseased cornea should be removed via debridement or lamellar keratectomy, as described above. A number 64 Beaver blade is used to make two diverging, halfthickness corneal stromal incisions from each edge of the defect and continued over the limbus, approximately 1 mm into the conjunctiva. In the authors’ experience, making the conjunctival incisions slightly more divergent than the corneal incisions allows for better coverage and fit of the graft. Next, the edge of the outlined donor cornea is grasped with 0.12 mm Colibri forceps and lifted slightly. As with a keratectomy, the lamellae are carefully dissected using a Martinez corneal dissector or number 64 Beaver blade, continuing toward the limbus. Once the donor cornea has been properly dissected, the 0.3 Colibri forceps can then be used to elevate the edge of the conjunctival incision, and tenotomy (Westcott or Stevens) scissors used to perform gentle blunt dissection of the conjunctiva from the underlying Tenon’s capsule and episcleral tissue.
Once fully dissected, the attachment of the graft at the limbus is transected using tenotomy scissors, taking special care to ensure there is no perforation of the donor graft in any area. If the edge of the donor corneal graft is diseased or grasped during harvesting, it should be trimmed. Next, the graft will be sutured in place with two cardinal sutures in each corner of the recipient bed. The rest of the graft may be attached using simple interrupted or simple continuous suture patterns. 47 Most surgeons use 8-0 or 9-0 absorbable suture material for this surgery.
Penetrating keratoplasties
✜
✜
✜
Penetrating keratoplasties are more commonly known as corneal transplants. Although these techniques may be utilized for several of the disease processes discussed in this article, corneal transplantation is complex, and a detailed description of the different procedures is beyond the scope of this review.
Postoperative care
In general, most patients should wear an Elizabethan collar following corneal surgery to allow for proper healing. Some surgeons prefer to place a single lateral temporary tarsorrhaphy to provide additional corneal protection for the days following surgery, but this is not a general requirement.
Use of specific topical antibiotics, mydriatic agents, artificial tears, systemic antibiotics, systemic anti-inflammatories and pain medications may be determined by the veterinarian to provide proper analgesia and infection control. If the cornea was infected preoperatively, more aggressive antimicrobial therapy may be warranted. Conversely, if there was no infection present, prophylactic use of antimicrobials may be warranted.
Suture removal is not needed if absorbable suture material was used; however, absorbable suture may lead to granulation tissue formation. If non-absorbable suture was used, suture removal should be performed approximately 21 days postoperatively.
For most corneal procedures, the authors recommend a 1-week postoperative recheck. If there are no complications and the cornea is healing well, the next recheck is typically 3-4 weeks postoperatively, at which time the sutures should be dissolving and the Elizabethan collar may be removed.
Key Points
✜ A good understanding of feline corneal diseases and microsurgery is required prior to recommending and performing corneal surgery.
✜ Corneal lacerations/injuries, deep ulcerative keratitis or corneal perforation, corneal sequestra, dermoids, corneal neoplasia and some indolent corneal ulcers often require surgical correction.
✜ Individuals performing presurgical preparation should use extreme caution when manipulating the patient’s head and eye, as many corneal diseases have a fragile cornea.
✜ Appropriate microsurgical instrumentation, training and magnification are essential for good corneal surgical outcomes. Most of these surgeries should be performed by ophthalmologists.
✜ Adjunctive medical therapy and proper postoperative care is imperative for corneal surgical success.

Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.