
Abstract
Objectives
The aims of this study were to evaluate serum symmetric dimethylarginine (SDMA) and creatinine concentrations in cats with urethral obstruction pre- and post-decompression of the obstruction, and to determine if pre-decompression values were predictive of post-decompression renal function, as measured by SDMA and creatinine.
Methods
This was a prospective observational study. Twenty-five client-owned cats with urethral obstruction were hospitalized for decompression of the obstruction. Serum SDMA and creatinine were prospectively assessed at presentation, 24 h post-decompression and 5–20 days post-decompression. Urinalysis and culture were assessed at presentation and at the final follow-up. Exclusion criteria included positive urine culture, reobstruction or failure to obtain required samples.
Results
Mean SDMA concentration dropped by 41.8% from an initial pre-decompression concentration of 17.6 µg/dl to 10.3 µg/dl 24 h post-decompression (P <0.001). The mean creatinine value dropped by 38.4% from an initial pre-decompression concentration of 2.5 mg/dl to 1.5 mg/dl 24 h post-decompression (P <0.001). There was no association between SDMA concentration at initial presentation and SDMA concentration 5–20 days after urethral catheterization (Spearman’s ρ = 0.205, P = 0.314). Creatinine concentration upon initial presentation was associated with the 5–20 day values after urethral catheterization (Spearman’s ρ = 0.583, P <0.002). Twenty percent of cases were excluded due to bacterial growth on initial urine culture. SDMA and creatinine concentrations were significantly higher in these cases (median 59 µg/dl and 10.9 mg/dl, respectively) compared with those with negative cultures (median 14 µg/dl and 1.6 mg/dl [P <0.002 and P <0.001], respectively).
Conclusions and relevance
Both SDMA and creatinine decreased significantly after urethral catheterization, suggesting that renal function post-decompression cannot be predicted by the pre-decompression concentrations of these values.
Introduction
Measurement of glomerular filtration rate (GFR) is the gold standard for assessing renal function in dogs and cats. 1 However, GFR measurement is cumbersome, and therefore more easily measured surrogate markers of GFR are more clinically practical. Blood urea nitrogen (BUN) and creatinine are commonly used surrogates of GFR; however, both can be affected by extrarenal factors (breed, protein intake, muscle mass), leading research to focus on identifying more sensitive and specific biomarkers.2–4
Symmetric dimethylarginine (SDMA), a product of L-arginine methylation, has been investigated as a renal biomarker in cats, with studies documenting an inverse linear relationship between SDMA and GFR.5,6 In cats with chronic kidney disease (CKD), SDMA has been found to be a more sensitive marker for GFR than creatinine. 6 Several studies in dogs with CKD have also identified SDMA as a more sensitive marker for GFR than creatinine, though another study in dogs with CKD found similar diagnostic performance between SDMA and creatinine in early detection of decreased GFR.7–9 SDMA has not been investigated in cats with acute kidney injury (AKI) and limited information regarding SDMA and AKI in dogs is available. No published data are available regarding SDMA in cases of post-renal azotemia in dogs or cats.
Urethral obstruction (UO) is a common emergency in male cats, thought to most commonly result from sterile cystitis and urethritis, resulting in urethral spasm, edema or urethral plug formation. 10 Most cats with UO are otherwise healthy; however, urolithiasis and infection occur in a minority of cats with lower urinary signs (10–22% and 2–15%, respectively).11–14 UO causes an abrupt increase in nephron tubular pressure, resulting in decreased GFR and post-renal azotemia. Relief of a urinary obstruction typically results in a decrease in BUN and creatinine, suggesting that the magnitude of azotemia during an obstruction is not indicative of underlying renal function. 15 While SDMA has not been studied in feline UO, an understanding of its physiology would suggest that SDMA should parallel creatinine in these patients.
Anecdotally, some feline patients with UO are assigned a poor prognosis based on the severity of kidney biomarker elevation prior to decompression, leading to client hesitance for treatment and referral. Given the potential outcome of euthanasia, understanding the relationship between severity of kidney biomarker increase and long-term prognosis is essential.This study aimed to evaluate serum SDMA and creatinine concentrations in cats pre- and post-decompression of the UO, and to determine if pre-decompression values were predictive of post-decompression renal function, as measured by SDMA and creatinine. We hypothesized that SDMA would mirror creatinine in pre- and post-decompression UO. We also hypothesized there would be no association between pre- and post-decompression SDMA, indicating that in the setting of a UO, an increased SDMA is not predictive of post-decompression renal function, and an increased SDMA can be reflective of UO and possibly other post-renal causes of azotemia.
Materials and methods
This prospective, observational study was conducted at The Animal Medical Center from January 2016 to August 2017. Client-owned cats admitted to the hospital for treatment of UO were eligible for enrollment. The study protocol was reviewed and accepted by The Animal Medical Center's Institutional Animal Care and Use Committee and informed consent was obtained prior to enrollment. UO was diagnosed based on palpation of a large, turgid urinary bladder that could not be manually expressed, in conjunction with non-productive stranguria.
Blood was obtained at the time of admission for assessment of serum SDMA, BUN, creatinine and potassium concentrations. Immediately following urethral catheterization, a urine sample was obtained from the catheter and submitted for urinalysis and urine culture and sensitivity. A lateral radiograph of the abdomen was performed to confirm appropriate urinary catheter placement and to assess for radiopaque cystoliths. Cats were hospitalized for a minimum of 24 h with a urethral catheter in place. If the catheter was inadvertently removed or determined to be non-patent during the first 24 h, it was replaced within 8 h. All cats received intravenous fluids at rates determined by the attending clinician based on hydration status. Additional treatments included antiemetics, proton pump inhibitors, H2 antagonists, alpha-adrenergic antagonists and opioid pain medications. Some cats received empiric antibiotics while pending urine culture results.
Twenty-four hours after initial urethral catheter placement, a second serum sample was obtained to reassess renal parameters. Cats were discharged from the hospital once they were observed to urinate successfully after removal of the urethral catheter.
Cats were re-evaluated a median of 10 days (range 5–20 days) following the UO event, at which time blood was obtained for reassessment of renal parameters. Urine was obtained via cystocentesis and submitted for urinalysis and culture. If only a small volume of urine could be obtained, then only a culture was submitted.
Cats were excluded from the study if they were <1 year of age, had known pre-existing renal disease, if bacterial growth was identified on urine culture at any point during the study, if the cat showed evidence of reobstruction for >8 h during the study period, if the cat was hospitalized for <24 h, if the cat underwent cardiopulmonary arrest or was euthanized during the study period, or if sufficient samples could not be obtained at the appropriate time points. Cats undergoing surgery (such as perineal urethrostomy, cystotomy) during the study period were included. Cats that received antimicrobials were included if antimicrobials were started <1 h from the time of urine sample collection and the cultures were negative at all time points.
Serum creatinine and BUN concentrations were determined by enzymatic colorimetric methods by IDEXX. 2 The reference interval (RI) used for BUN concentrations in healthy cats was 16–37 mg/dl. The RI for creatinine concentrations in healthy cats used the IDEXX Laboratory standard of 0.9–2.5 mg/dl. Serum SDMA concentrations were determined by immunoassay by the same IDEXX laboratory, as previously described.16,17 The RI for SDMA concentrations was 0–14 μg/dl. The RI for potassium concentrations was 3.7–5.2 mmol/l.
Urine was analyzed via physical, chemical and microscopic analyses. Physical analysis consisted of visual inspection of color and clarity, and urine specific gravity measured by refractometry. Chemical analysis consisted of dipstick (Multistix; Siemens Healthcare Diagnostics) analysis of pH, protein content, glucose concentration, ketones, hemoglobin, bilirubin and urobilinogen. Microscopic analysis consisted of assessment for leukocytes, erythrocytes, bacteria, epithelial cells, mucus, casts and crystals, using an inverted microscope.
Urine culture was performed using agar plates; bacterial identification was performed using matrix-assisted laser desorption/ionization time-of-flight mass spectrometry, 18 and antibiotic sensitivities were determined using the Vitek system (bioMérieux). Urine cultures were deemed negative if no growth was noted after 48 h. If the culture was positive for bacterial growth, the minimum inhibitory concentration for antimicrobials were determined by a commercial automated system.
Statistical analysis
To account for individual patient variation, repeated measures were analyzed using a linear mixed model with SDMA or creatinine as the outcome variables, time as the fixed effect and cats as the random effect. P values generated from the mixed models were adjusted using the Holm–Bonferroni method. Owing to non-normality of the residuals, the log forms of both SDMA and creatinine were used to ensure homoscedasticity and verified by residual plots for both regression models. Percentage change from baseline was calculated using mean baseline scores as defined by Vickers. 19 The Mann–Whitney U-test was used to compare creatinine and SDMA concentrations among the cats with positive and negative urine cultures. To investigate the relationship between SDMA and bacteriuria, an exploratory analysis on the excluded samples with positive urine cultures was also conducted. Pearson’s χ2 test was used to test independent proportions. Confidence intervals for proportions were calculated using the binomial exact method. Associations were analyzed using Spearman’s ρ correlation coefficient, due to its robustness to outliers and non-normally distributed data. Continuous variables not reported as model estimates were reported as median and range. Statistical significance was set at alpha = 0.05. All data manipulation and analysis were conducted using R version 3.5.3 with the following packages: tidyverse, and lme4.20–22
Results
During the study period, 59 cats (61 cases of UO) were hospitalized for UO and deemed eligible for inclusion in the study. Twenty-six cases met the inclusion criteria. The reasons for exclusion of 35 UO cases were failure to return for follow-up assessment (n = 14 [40%]), bacterial growth on initial (n = 12 [34%]) or follow-up (n = 4 [11%]) urine culture, repeat UO during the study period (n = 1 [3%]), hospitalization for <24 h (n = 1, 3%), euthanasia during the study period (n = 1 [3%]), age <1 year (n = 1 [3%]) and cardiopulmonary arrest during the study period (n = 1 [3%]). One cat was included twice for two separate UO events, 5 months apart. Another cat was hospitalized twice for two separate UO events and met the inclusion criteria for the first UO but had a positive urine culture at the time of presentation with the second UO, and the second event was excluded from analysis. Twelve of the 35 excluded cases (34%) and four of the included cases (15%) had evidence of radiopaque uroliths or mineralized sediment on diagnostic imaging, totaling 16/61 cases (26%). No cats in this study had a perineal urethrostomy.
The 25 cats (26 UO cases) included in the study ranged in age from 1.3 to 16 years (median 4.8 years). Breeds represented included domestic shorthair (n = 21), Russian Blue (n = 2), domestic longhair (n = 1) and Korat (n = 1). The median duration of hospitalization was 2 days (range 1–7). Three cats underwent surgery (two cystotomy and one percutaneous cystolithotomy) during the hospitalization period. UO was idiopathic in 22 of the included cases (85%) and secondary to radiopaque urolithiasis in four (15%). One case remained azotemic with a creatinine of 4.3 mg/dl, a BUN of 33 mg/dl and an SDMA of 42 μg/dl at 5–20 days post-decompression. This cat presented in hypovolemic shock with severe hematuria upon decompression of the obstruction and required multiple blood transfusions due to urinary bladder hemorrhage.
The mean SDMA value dropped by 41.8% from a pre-decompression concentration of 17.6 μg/dl to 10.3 μg/dl 24 h post-decompression (P <0.001; Table 1, Figure 1a). The mean decrease in SDMA over the entire study period, relative to baseline, was 26.3% (P <0.024), with a mean SDMA of 13.0 μg/dl at 5–20 days post-decompression. The mean creatinine value dropped by 38.4% from a pre-decompression concentration of 2.5 mg/dl to 1.5 mg/dl 24 h post-decompression (P <0.001; Table 2, Figure 1b). The mean decrease in creatinine over the entire study period, relative to baseline, was 32.0% (P <0.006), with a mean creatinine concentration of 1.7 mg/dl at 5–20 days post-decompression. No difference in mean creatinine nor SDMA concentrations were observed between the 24 h and 5–20 days post-decompression time points (P >0.079).
Mean symmetric dimethylarginine (SDMA) concentration from initial pre-decompression through 5–20 days post-treatment
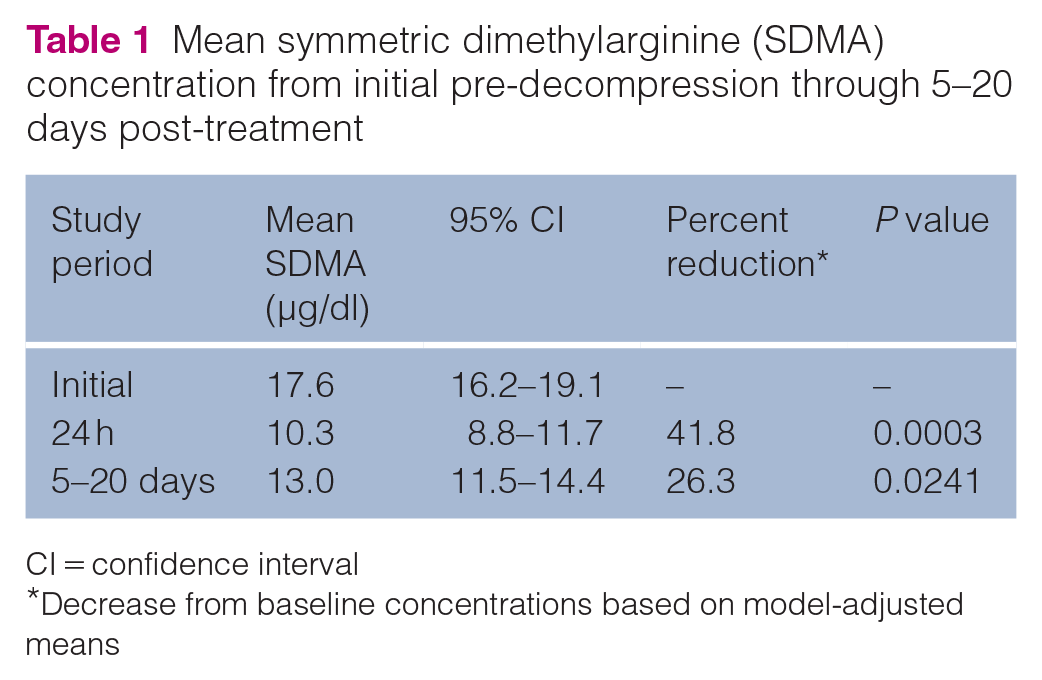
CI = confidence interval
Decrease from baseline concentrations based on model-adjusted means

Trend in (a) symmetric dimethylarginine (SDMA) values and (b) creatinine values from the initial pre-decompression time point to the 5–20 day post-decompression time point
Mean creatinine (mg/dl) concentration from initial pre-decompression through 5–20 days post-treatment

CI = confidence interval
Decrease from baseline concentrations based on model-adjusted means
Pre-decompression SDMA values were observed to be associated with pre-decompression creatinine values (Table 3, Figure 2a). The 24 h post-decompression SDMA values were observed to be associated with creatinine values 24 h post-decompression (Table 3, Figure 2b). No association was observed between the 5–20 day post-decompression SDMA and creatinine values (Table 3, Figure 2c).
Comparison of symmetric dimethylarginine (SDMA) and creatinine pre- and post-decompression


Association between (a) initial symmetric dimethylarginine (SDMA) values and initial creatinine values, (b) 24 h post-decompression SDMA values and 24 h post-decompression creatinine values and (c) 5–20 day post-decompression SDMA values and 5–20 day post-decompression creatinine values
No association was observed between the pre-decompression SDMA values and creatinine values at 24 h or 5–20 days post-decompression (Table 3). When pre-decompression creatinine was compared with 24 h post-decompression SDMA values there was a significant association, but no association was observed when pre-decompression creatinine values were compared with 5–20 days post-decompression SDMA values (Table 3).
SDMA values pre-decompression were associated with SDMA values 24 h post-decompression (Table 3, Figure 3a). There was no association between pre-decompression SDMA values and SDMA values 5–20 days post-decompression (Table 3, Figure 3b). Pre-decompression creatinine values were associated with creatinine values 24 h post-decompression (Table 3, Figure 4a) and 5–20 days post-decompression (Table 3, Figure 4b).

Association between (a) initial symmetric dimethylarginine (SDMA) values compared with SDMA values 24 h post-urethral catheterization and (b) initial SDMA values compared with SDMA values 5–20 days post-urethral catheterization

Association between (a) initial creatinine values compared with creatinine values 24 h post-urethral catheterization and (b) initial creatinine values compared with creatinine values 5–20 days post-urethral catheterization
Twelve of 61 cases (19.7%) were excluded from the study owing to the presence of bacterial growth on urine culture at the time of presentation with a UO. Of these cases, one had a urinary catheter in place within 30 days of enrollment. An underlying cause of bacteriuria was not identified in the other 11 cases. The most common organism cultured on initial cultures was Escherichia coli (found in 50% of cases). One-third of positive cultures (n = 4/12) had growth of multiple organisms. Bacterial growth was low (1–10,000 colony-forming units [CFU]/ml) in four cases, moderate (10–50,000 CFU/ml) in four cases and marked (>50,000 CFU/ml) in four cases.
SDMA values were higher in cats with a positive culture (median 59 μg/dl [range 10–100]) than cats with a negative culture (median 14 μg/dl [range 5–100]; P <0.002 [Figure 5a]). Similarly, creatinine values were higher among cats with a positive culture (median 10.9 mg/dl [median: 10.9 mg/dl; range 1.3–20.9]) than cats with a negative culture (median 1.6 mg/dl [range 0.3–22.8]; P <0.001 [Figure 5b]). Additionally, hyperkalemia was more common in cats with positive cultures (83% [n = 10/12]) than in those with negative cultures (24% [n = 12/49]; P <0.014).

Boxplot of (a) symmetric dimethylarginine (SDMA) values and (b) creatinine values in cases with and without a positive culture. Whiskers represent × 1.5 the interquartile range
Discussion
The results of this study confirm a positive correlation between SDMA and creatinine in the setting of a feline UO. This correlation is consistent with prior studies of SDMA and creatinine in dogs and cats with CKD.6,8 This study found no association between pre-decompression SDMA and either creatinine or SDMA values in the follow-up period 5–20 days post-decompression of the UO.
SDMA concentrations were observed to decrease by 42% within the first 24 h and remained decreased upon follow-up evaluation 5–20 days later. This decline in SDMA is presumed to represent restoration of GFR after urethral patency is re-established. While prior research has validated SDMA as a marker of CKD,5,8 the data presented here suggest that UO is also a potential cause of increased SDMA in cats, and post-renal etiologies should be considered when SDMA is found to be increased. While a component of CKD cannot be definitively ruled out in these cases, the decline in SDMA values over the course of the study suggest that an increased SDMA with UO is not caused by permanently reduced renal function, and the prognosis of a patient should not be based on an SDMA or creatinine value obtained at presentation.
No association was found between SDMA and creatinine values at the 5–20 day time point, despite associations between SDMA and creatinine at the pre-decompression and 24 h time points. Seven cats had increased SDMA values above the RI at the 5–20 day time point, compared with only one cat with an increased creatinine at that time point. This may reflect a delay in recovery of GFR in these patients, indicating that renal recovery following UO may occur over a longer period. Future studies assessing renal parameters in cats with UO over several months post-decompression may help further clarify the time period over which renal recovery occurs in these patients.
An unexpected finding in this study was the prevalence (19.7%) of bacterial growth on initial urine culture. Whether positive cultures represented true infection or iatrogenic contamination during catheterization is unclear, as all urine samples were obtained via catheterization. A 2019 study by Cooper et al on the incidence of bacteriuria in cats with UO found that none of the 34 cats in that study had bacteriuria at the time of presentation with UO, when urine was obtained by cystocentesis. 23 Thirteen percent (n = 4/31) of cats in that study developed bacteriuria after the indwelling urethral catheter was placed; two of which had their catheter in place for 48 h and two for 72 h. These findings suggest that the bacteriuria in the present study may have been more likely to be catheter-associated rather than representative of true infection.24,25 However, given that the majority of cases with positive urine cultures in the present study had moderate-to-high growth of a single organism, bacteriuria may be more common than previously thought in cats with UO and urine cultures may be indicated as part of the minimum database in these cases.
Cats with bacterial growth on initial urine culture were found to have higher SDMA and creatinine concentrations at the time of presentation, compared with cats with no growth on initial culture. This may suggest a component of renal azotemia, as caused by pyelonephritis, or could suggest that cases of prolonged or severe UO are more prone to developing infection. Given the severe azotemia in the majority of these cases, it is also possible that these patients were more debilitated on presentation, with a potentially higher likelihood of contamination of the urine sample due to the emergent nature of the unblocking procedure and less time being taken to ensure aseptic technique. Therefore, it is unclear if the bacteriuria was a cause or consequence of the UO in these cases. Further studies are needed to better define the relationship between positive urine cultures and renal parameters in cats with UO.
This study has several limitations, many inherent to the management of a UO. Because of poor owner compliance, a number of patients failed to complete the study, limiting the sample size enrolled. The final recheck visit took place over a relatively long timespan (5–20 days) to accommodate the schedules of the cats’ owners. Patients were included in the study regardless of their hydration status; therefore, some patients likely had a component of pre-renal azotemia, and intravenous fluid therapy may have accounted for some improvement in renal parameters. Fluid therapy was not standardized in this study, and many patients with UO experience some degree of post-obstructive diuresis following relief of the obstruction. Additionally, the willingness of patients to eat or drink following relief of their obstruction varied greatly. These factors likely contributed to differences in hydration status among cases, thereby affecting renal parameters. Additionally, many patients received alpha-1 antagonists, which may have resulted in transient hypotension or other adverse effects (lethargy, diarrhea), which could impact renal function or hydration status, respectively. The duration of time over which the UO had been present for each patient could not be accurately determined, and this likely was a major factor affecting both the degree of SDMA and creatinine elevations, and the rate of return of these values to baseline, for these patients. Renal azotemia may have been present in some cats because of underlying CKD or acute kidney injury associated with the UO event or other factors. Some cats had normal renal parameters at the time of initial presentation with UO, resulting in minimal change in renal parameters over the course of the study. This likely contributed to the association between some pre- and post-decompression values. This study did not assess GFR in cats, as this would have been impractical in the setting of managing cats with UO; therefore, conclusions regarding whether SDMA is truly a reflection of GFR following relief of a UO cannot be made. Given prior studies that have shown a correlation between GFR and SDMA and minimal effects of extrarenal factors on SDMA, it can be inferred that the improvement in SDMA over the course of the study reflects restoration of GFR following relief of the obstruction. Another limitation is that urine cultures were obtained via catheterization, as opposed to cystocentesis, which likely excluded cats that developed catheter-associated bacteriuria during urethral decompression. Cats obstructed with uroliths were included in this study, even though they underwent another anesthetic event for stone removal, which may have affected GFR and SDMA levels upon recovery.
Conclusions
This study demonstrated that in the setting of a feline UO, SDMA and creatinine are positively correlated, suggesting that SDMA is a marker of post-renal azotemia in cats. Based on these data, an increased SDMA should not be interpreted to solely represent renal dysfunction, and urinary obstruction should be considered as a differential diagnosis in any patient with an increased SDMA. The results of this study suggest that bacteriuria and urolithiasis may be more frequent in cats with UO than has been historically reported, and bacteriuria may be more prevalent in more severely azotemic UO cats. Further studies are warranted to assess the relationship between positive urine cultures and renal parameters in cats with UO.
Footnotes
Acknowledgements
The authors would like to acknowledge all staff and owners involved in the care of patients enrolled in the study.
Author note
This study was presented as an abstract at the 2018 ACVIM Forum in Seattle, WA, USA.
Conflict of interest
IDEXX Laboratories holds a patent on the proprietary immunoassay methodology for measuring symmetric dimethylarginine (SDMA) concentration (United States Patent No US 481,690 B2; Date: July 9, 2013 Murthy et al, Methods for Detecting Symmetrical Dimethylarginine) and manufactures the IDEXX SDMA Test evaluated in this study. IDEXX Laboratories provided client incentives for this study.
Funding
Financial support for this study (client incentives) was provided by IDEXX Laboratories.
Ethical approval
This work involved the use of non-experimental animals only (owned or unowned animals). Established internationally recognized high standards (‘best practice’) of individual veterinary clinical patient care were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.