
Abstract
Objectives
The aim of this study was to evaluate and compare the long-term clinical outcomes and quality of life of cats having undergone perineal urethrostomy (PU) or prepubic urethrostomy (PPU).
Methods
This clinical study followed 28 cats (PU, n = 22; PPU, n = 6) that underwent a urethrostomy, with a minimum of 1 year postoperative follow-up. Medical records, pet owner surveys and urologic laboratory tests were used for assessment. Urologic laboratory tests included serum symmetric dimethylarginine (SDMA), serum creatinine, urinalysis, urine specific gravity (USG), urine protein:creatinine (UPC) ratio and urine culture.
Results
The main indications for urethrostomy were multiple catheterizations and PU stricture. The overall complication rates of PU and PPU were 31.8% and 83.3%, respectively. Recurrent urinary tract infection (UTI) and urine scald dermatitis were less frequent in PU than in PPU cats (UTI 22.7% vs 66.6%; dermatitis 4.5% vs 83.3%). Bacteriuria was present in 77.2% and 100% of PU and PPU cats, respectively. Owner satisfaction rates were excellent in 81.8% of PU and 33.3% of PPU cases.
Conclusions and relevance
A proportion of cats that underwent urethrostomy showed bacteriuria, recurrent UTIs and increased levels of SDMA. PPU is important as a salvage procedure; however, it should be limited to cases in which standard techniques for PU cannot be performed, owing to the potential for recurrent complications and lower owner satisfaction.
Introduction
Feline lower urinary tract disease (FLUTD) is one of the most common diseases encountered in the clinical setting. 1 This disorder is characterized by dysuria, hematuria, stranguria, pollakiuria, periuria and appetite alteration.2,3, Urethral obstruction also has been reported in 28.6% of FLUTD cases. 3
Urethrostomy is indicated in cases of recurrent urethral obstruction or where medical management does not sufficiently relieve the urethral obstruction. These cases include urethral strictures, penile deformities, urethral neoplasms, foreskin edema and iatrogenic urethral disruption through inappropriate urethral catheterization.4,5 Perineal urethrostomy (PU) is a technique associated with penectomy, in which a new ostium for the urethra is created in the perineal region. 5 Some proximal urethral obstructions may not be suitable for PU and a more cranial urinary diversion, such as prepubic urethrostomy (PPU) or transpubic urethrostomy, 6 is indicated. These salvage urinary diversion procedures frequently have reported complications, such as urinary incontinence, urinary tract infections (UTIs), peristomal dermatitis, subcutaneous urine leakage and stenosis.4,5,7 Hence, this study aimed to evaluate and compare the long-term clinical outcomes and quality of life (QoL) for cats following PU or PPU.
Materials and methods
Study design
This research was developed in accordance with the Ethical Principles of Animal Experimentation, adopted by the Committee of Ethics for the Use of Animals of the State University of Ceará (CEUA–UECE; 8438995/2018).Medical records from the Veterinary Hospital of the State University of Ceará and Catus Veterinary Clinic were reviewed and cats that had undergone a urethrostomy between July 2014 and July 2017 were selected from a database. The criterion for inclusion in this study was a minimum of 1-year postoperative follow-up. Cats with a diagnosis of chronic kidney disease (CKD) prior to the date of urethrostomy were excluded. CKD diagnosis was based on increased serum creatinine and serum symmetric dimethylarginine (SDMA), proteinuria and poor corticomedullary distinction as observed by ultrasound. Pet owners of cats eligible for this study were contacted and offered a follow-up consultation. At the time of the follow-up, they were asked to fill out a questionnaire. Concomitantly, patient blood and urine samples were collected for analysis.
Pet owner survey
The survey was constructed to elucidate the following: cat age at castration; number of prior obstruction events; immediate and later postoperative alterations, including signs of FLUTD (hematuria, stranguria or periuria) and dermatitis at the surgical area; and level of satisfaction with the surgical outcome and QoL for the cat. QoL was assessed based on the preservation of urine continence, social behavior with the owners and signs of pain. The survey included an explanation for owners on how to define these clinical signs.
Medical record review
The data from the medical records reviewed included age, body condition score, main clinical signs observed, history of CKD, surgical technique, reason for surgical indication and perioperative interventions. Data were related to the time of surgery. Records of UTI frequency confirmed by urine culture were also obtained.
Laboratory analysis
Blood and urine samples were collected with fasted and normohydrated animals. Blood was collected from the cephalic or jugular vein (0.5–1 ml) and stored in a tube without anticoagulant. Serum creatinine and SDMA levels were assessed by liquid mass spectrometry (CataLyste-IDEXX).
Urine collection was performed by cystocentesis for urinalysis, urine protein:creatinine (UPC) ratio and urine culture. Urine specific gravity (USG) was measured using a refractometer. Chemical examinations were performed with a Multistix SG Reagent Strip. Urinary creatinine concentrations were determined using the modified Jaffé method in an ADVIA 1650/Mega Bayer automated apparatus. Urine protein concentration was established using the colorimetric method with pyrogallol red using an automated device (ADVIA 1650/Cobas Mira Plus). The UPC ratio was obtained by dividing the urine protein concentration by the urine creatinine concentration. The BD CLED Agar/MacConkey II Agar kit was used for the urine culture and an antibiogram was performed with the Kirby & Bauer disk diffusion technique. A urine pellet was obtained by centrifuging urine at 112 g for 5 min and then discarding the supernatant. The pellet was examined with a light microscope at × 400 magnification. All blood and urine analyses were processed within 4 h of collection.
CKD staging
Cats were classified as having stage 1, 2, 3 or 4 CKD according to International Renal Interest Society (IRIS) guidelines using creatinine and SDMA values. 8 Patients with increased values of either creatinine or SDMA were reassessed after 2–3 weeks. CKD staging was determined based on a persistent increase of either creatinine or SDMA. Cats with serum creatinine >1.6 mg/dl were considered azotemic. Laboratory reference intervals (RIs) of SDMA and USG were defined, respectively, as 0–14 µg/dl and 1.035–1.060. Samples with UPC ratios of <0.2 were classified as non-proteinuric.
Statistical analysis
The collected data were documented and tabulated. Statistical analyses were performed using GraphPad Prism 5.0 (GraphPad Software). Either a χ2 or Fisher’s exact test was used to compare two groups for categorical variables, as deemed appropriate. Following confirmation of normal distribution, an unpaired Student’s t-test or a Mann–Whitney U test was carried out to compare the creatinine, SDMA, USG and UPC ratio data between PU and PPU groups. The statistical significance level was defined as P <0.05. The data are presented as mean ± SD.
Results
Thirty-five cats were identified as having undergone urethrostomy (Figure 1). Seven cats were excluded from the analysis, either owing to their history of CKD (n = 5) or because the owners declined follow-up (n = 2). Therefore, 28 cats that had been submitted for PU (n = 22) or PPU (n = 6) were included in this study. The time lapse after surgery spanned 12–24 months, depending on when the surgical procedure was performed.

Study flowchart. CKD = chronic kidney disease
Medical record review
All surgeries were performed by the same surgeon using a technique described by Wilson and Harrison 9 for PU and by Baines et al 10 for PPU. Preoperative treatment consisted of acid–base stabilization with intravenous crystalloid fluid therapy, pain management with opioid analgesic (tramadol hydrochloride 2 mg/kg q8h), cystocentesis whenever necessary and urethral catheterization whenever possible. For postoperative treatment, opioid analgesic was prescribed orally for 4 days and an Elizabethan collar was worn by all cats immediately after recovery from anesthesia to prevent self-mutilation of the surgical site. An antibiogram-based therapy was prescribed whenever urine microbial culture was positive. Where indicated, dietary management of FLUTD was performed based on urine sediment assessment.
The preoperative clinical data of the cats that underwent urethrostomy are given in Table 1. The most common indication for PU was recurrent FLUTD (54.5%), followed by urethrostomy stricture and penis/urethra trauma (Figure 2a,b). The main recommendation for the PPU technique was PU stricture (83.3%) (Figure 2c). The only case of PPU performed in a female cat was due to adherence and fistulation of the uterus in the urethra, subsequent to an elective ovariohysterectomy. The median age of the patients that underwent PU and PPU was 3.38 and 2.5 years, respectively. Regarding preoperative reproductive status, 68.1% of the cats that underwent PU and 100% of the cats that underwent PPU were already neutered. Most PU cats (72.7%) were fed a dry diet, while 50% of PPU cats were fed a mixed diet (wet and dry). The body condition score (BCS) of preoperative patients was analyzed. A total of 59.1% of the patients referred for PU and 66.7% of patients indicated for PPU had high BCSs (4–5, on a scale of 1–5). Multiple catheterization was reported in 90.9% and 83.4% of PU and PPU cases, respectively.
Preoperative clinical history of cats that underwent either perineal urethrostomy (PU) or prepubic urethrostomy (PPU)
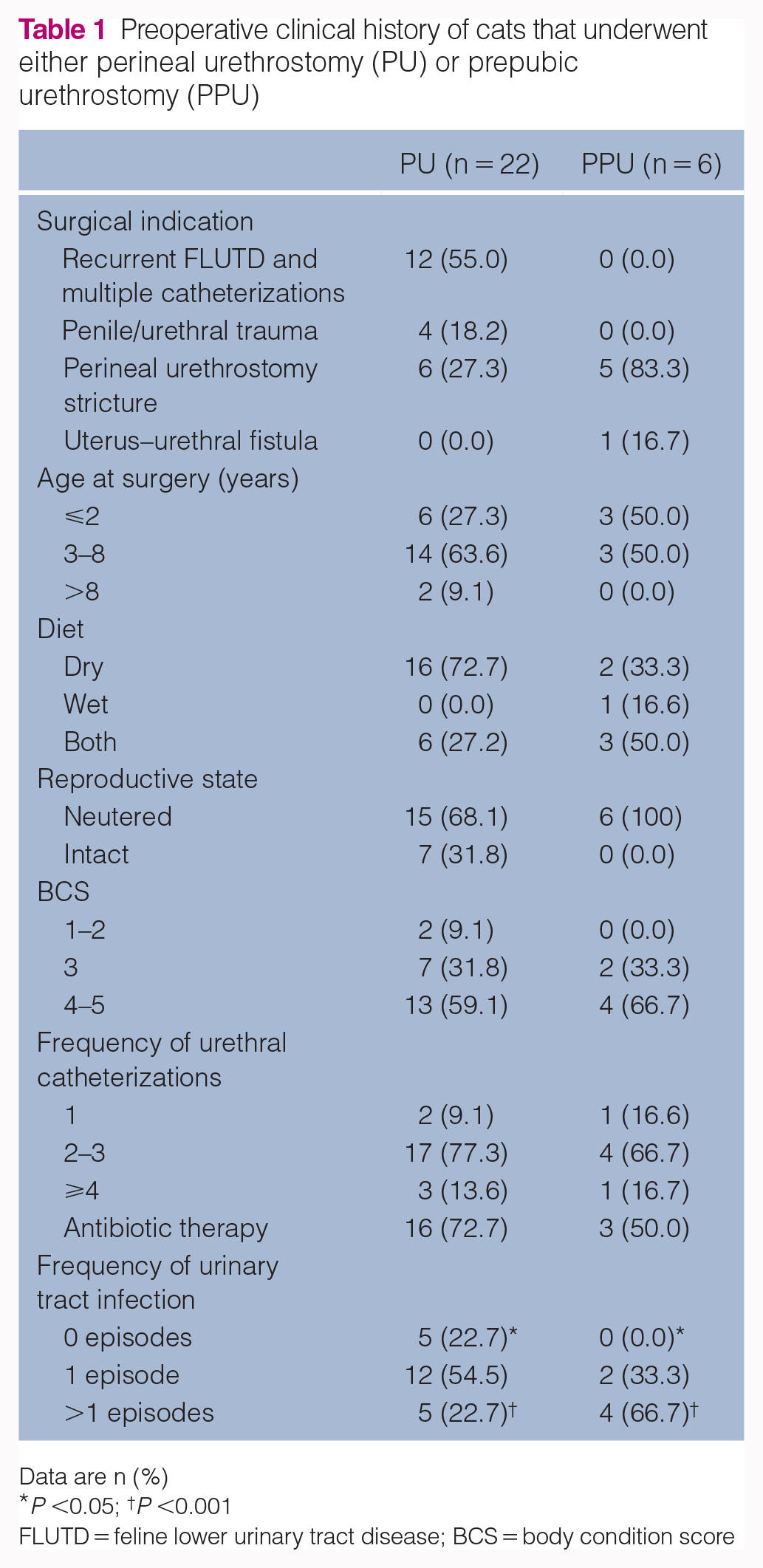
Data are n (%)
P <0.05; † P <0.001
FLUTD = feline lower urinary tract disease; BCS = body condition score

(a) Urethral rupture with extravasation of urine into the scrotum; (b) penis laceration and urethral stenosis; (c) perineal urethrostomy stricture
In 72.7% of PU cases, preoperative antibiotic therapy was administered after catheterization. The same was done in 50.0% of PPU cases. Calcium oxalate bladder urolithiasis was diagnosed in two cats (9.1%), 18 and 20 months after PU. This was not observed in any animals that had undergone PPU.
Pet owner survey
The main transient postoperative complication with both PU and PPU was hematuria (72.7% vs 83.3%) (Table 2).The overall complication rate was 31.8% for PU and 83.3% for PPU (P <0.05). Recurrent signs of FLUTD were less frequent in PU than in PPU patients (22.7% vs 66.7%; P <0.05). A significantly less common complication of PU was peristomal dermatitis around the urethral ostium, which was present in only 4.5% of cats. However, this was present in 83.3% of cats that had undergone PPU (P <0.0001). Urinary incontinence was observed in one case of PPU (16.7%) in the immediate postoperative period, with no subsequent recovery of function. Recurrent lower UTIs (>1 episode) were less frequent in PU than PPU cats (22.7% vs 66.6%; P <0.001).
Postoperative clinical history of cats that underwent either perineal urethrostomy (PU) or prepubic urethrostomy (PPU; 12–24 months follow-up)

Data are n (%)
P <0.05; †P <0.0001
FLUTD = feline lower urinary tract disease
The continued use of a commercial acidifying diet in the postoperative period for 30 days was followed in most cases (77.3% of PU and 50.0% of PPU patients). Owner satisfaction after urethrostomy was considered excellent in 81.8% of PU cases and 33.3% of PPU cases (P <0.05).
Laboratory analysis
Laboratory analysis evidenced no significant difference between the two cohorts. SDMA levels were above the RIs in 22.7% of PU and 16.6% of PPU cases (Figure 3). Creatinine values were above the RI in 27.2% of PU cases. The USG was outside of the RI in 9.0% of PU cases, and UPC ratios were outside of the RI in 13.6% of cases.

Distribution of individual values of the analyses of cats that had undergone perineal urethrostomy (PU) or prepubic urethrostomy (PPU): (a) creatinine; (b) symmetric dimethylarginine (SDMA); (c) urine gravity density; (d) urine protein:creatinine (UPC) ratio. Horizontal lines indicate the limit of reference values of each test
Both the PU and PPU cohorts showed leukocyturia (90.9% vs 100%), hematuria (77.3% vs 83.3%), triple phosphate crystalluria (68.2% vs 33.3%) and bacteriuria (77.3% vs 100%). Staphylococcus species were the most common microorganism found in urinary culture of these patients, followed by Escherichia coli and Streptococcus species (Table 3).
Results of sediment analysis and urine culture of cats that underwent either perineal urethrostomy (PU) or prepubic urethrostomy (PPU; 12–24 months follow-up)
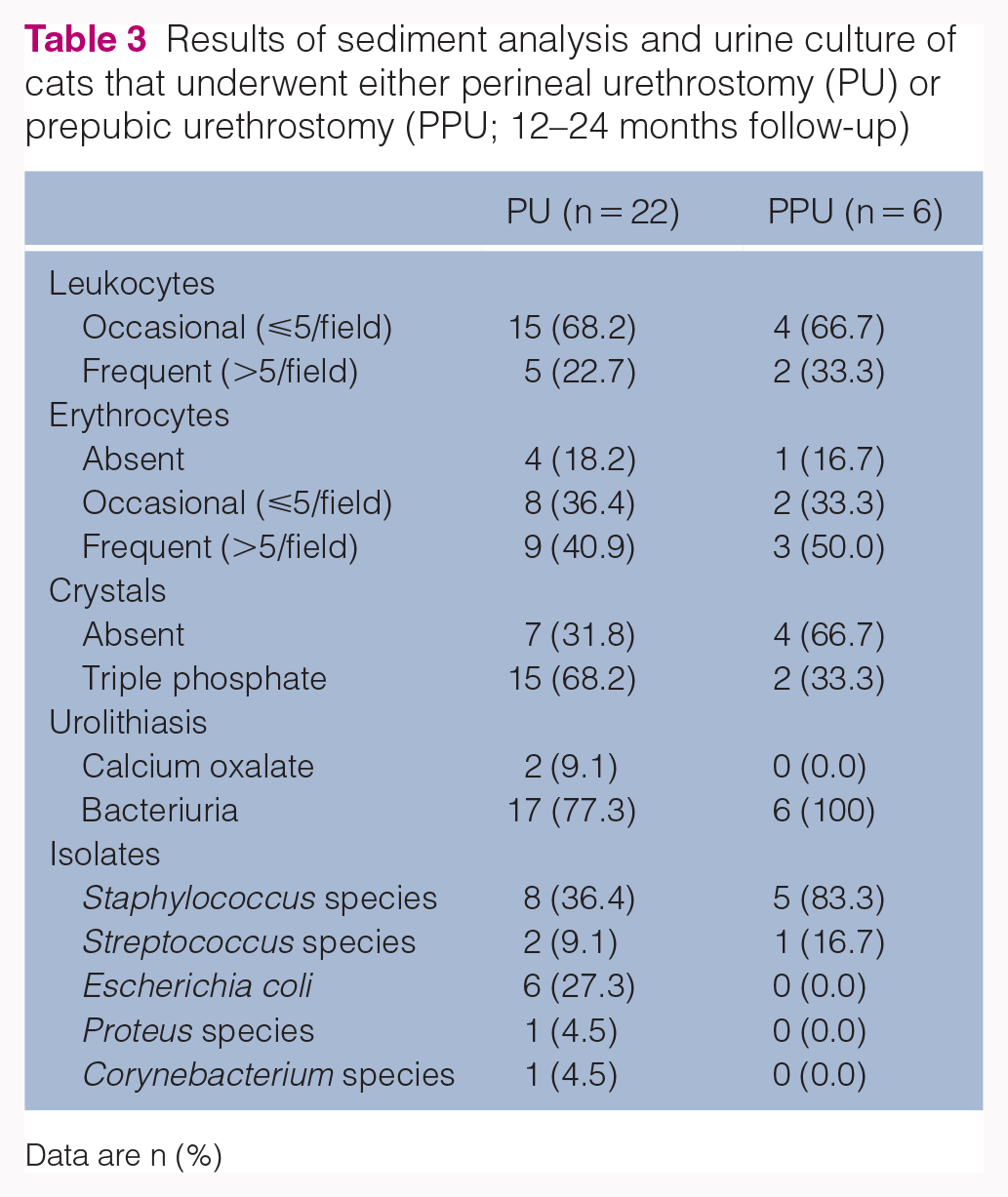
Data are n (%)
CKD staging
Eight cats were reassessed for CKD, owing to increased creatinine and/or SDMA values. Samples were taken 2 weeks after the initial evaluation. Three cats reassessed did not, in fact, have CKD. No significant differences in CKD levels and staging were observed between the two cohorts. In the PU group, one cat (4.5%) was classified as stage 1 and three cats (13.6%) were classified as stage 2 CKD, according to IRIS guidelines (Table 4). Only one cat (16.7%) with PPU presented with SDMA elevation with no other laboratory abnormalities or clinical signs of CKD and was classified as stage 1 CKD.
Cats that underwent perineal urethrostomy (PU) or prepubic urethrostomy (PPU) with early signs of chronic kidney disease (CKD) 12–24 months after urethrostomy

Values outside the reference interval are presented in bold
SDMA = symmetric dimethylarginine; UPC = urine protein:creatinine ratio; USG = urine specific gravity
Discussion
The aim of this study was to evaluate and compare the clinical outcomes of cats 12–24 months after PU and PPU. Our main findings were that: (1) urethrostomy does not always resolve the clinical signs of FLUTD; (2) PU is associated with less frequent complications, such as dermatitis, FLUTD and UTI clinical signs, than PPU; and (3) pet owners are more satisfied after PU than after PPU.
In the present study, there was only one case of an indication for urethrostomy in a female cat. This was due to adhesion of the uterine stump to the pelvic urethra in response to an intense suture reaction, 20 days subsequent to an elective ovariohysterectomy. Another case of urethral stenosis in a female cat has been reported in the literature, which was associated with an inflammatory response due to a trauma. 11 Male cats have a higher predisposition to urethral obstruction owing to their urethra being longer and narrower than that of female cats. 12
In this study, obesity (BCS >4) was observed in 59.1% of PU and 66.7% of PPU cases. This suggests that obesity is a factor predisposing to obstruction, as reported previously.1,12 The higher frequency of obstructive FLUTD in neutered cats was most probably due to the tendency to gain weight after neutering and not due to the neutering itself: one study did not find significant differences in anatomy and urethral diameter between intact and neutered cats. 13
The number of obstructive FLUTD episodes and multiple urethral catheterizations was frequent in most preoperative histories of patients that underwent PU and PPU. Yet, Seitz et al demonstrated that indwelling urethral catheterization remains the most indicated treatment. 14 However, multiple urethral de-obstructions increase the risks of urethral and penile stenosis or traumas. This is a major reason for urethrostomy. 15 Another common surgical indication for performing PU and PPU is postoperative urethral ostium stenosis, a serious complication of urethrostomy. 16 It has been reported that the risk of stoma stricture is higher after PU than after PPU. 10 This may be due to the diameter of the perineal urethra, which is four times narrower than in the prepubic region. The initial surgical indication for these animals is recurrent FLUTD clinical signs. Transient surgical complications such as hematuria, edema and hematoma are also common after surgery and have been reported previously.1,10 As in other studies,15,16 urethrostomy did not solve the FLUTD clinical signs in all cats operated on. However, the procedure has the advantage of decreasing the likelihood of re-obstruction.
Subcutaneous extravasation of urine is usually observed in cases of malposition of urethral mucosa or by dehiscence of sutures, 10 which was verified in one case of PPU. This condition was resolved with prolonged catheterization using a closed urinary drainage system for 15 days. The PPU technique may have a greater risk of incurring this complication owing to the tension the urethra is subjected to when sutured at the ventral region. 10
This study also evaluated the long-term complications of urethrostomy, including chronic peristomal dermatitis. This appeared to be more common in the PPU than the PU cohort. This may be explained because of the new location of the urethral ostium in the skin. Upon micturition, urine leakage into surrounding tissue may occur.
Urinary incontinence was observed in one case of PPU. This has previously been reported as a common complication of PPU, owing to the higher chance of vascular and neurologic damage.4,10 Recurrent UTIs were also reported significantly more often postoperatively in PPU cats compared with PU cats. However, bacteriuria was observed in 77.3% of PU and in 100% of PPU cats. Thus, as reported previously, 16 PU patients were more frequently asymptomatic. This highlights the importance of follow-up for cats that have undergone urethrostomy, since it may increase susceptibility to UTIs.16,17 This may be a consequence of the loss of the natural barrier that follows a penectomy. As a result, the urethral stoma is in greater proximity to the bladder. Presumably, this facilitates the ascent of infection. 18
The overall QoL of the cats that underwent the PU technique was reported as excellent by most owners, corroborating the findings of other studies.15,16 This improvement of animal welfare is fundamental to supporting the surgical decision in cases where there is recurrence of urethral obstruction. The PPU technique was also associated with a good level of satisfaction, even with the presence of complications related to peristomal dermatitis. In only one case was there an unsatisfactory opinion on the outcome of the procedure, which was a consequence of the patient’s urinary incontinence. These results differ from those reported by Baines et al, 10 who stated that 6/16 animals submitted to PPU were subsequently euthanized as a result of postoperative complications.
The IRIS guidelines state that fasting serum creatinine concentration is the first criterion for CKD diagnosis.8,18 Fasting serum creatinine concentration is a late marker of renal homeostasis and increases when approximately 75% of renal function is lost. 19 It should be noted that the muscle mass score may also affect the fasting serum creatinine concentration, but it was not assessed in this study. According to the IRIS guidelines, the diagnosis of CKD based on a single measurement of serum creatinine concentration is not recommended. However, serial collection of blood samples is often not practical in the clinical routine. Hence, in the present study, serum creatinine values were analyzed along with SDMA. SDMA is a new renal biomarker that allows for earlier diagnosis of renal disease than the traditional creatinine test. 20 SDMA levels reveal CKD in cats, on average, 17 months before the serum creatinine concentration surpasses the RI. 20
The concomitant increase of SDMA and serum creatinine was verified in three animals with PU. However, in one case of PU and one of PPU, an increase in SDMA was found without an increase in serum creatinine. However, these cats had concomitant increases in UPC ratios. An increase in creatinine in one cat of the PU cohort, that had a normal level of SDMA, was normalized after 3 weeks.
To support the diagnosis of CKD, UPC ratio and USG were also assessed. The gold standard method for analysis of proteinuria is the collection of all urine produced in 24 h. However, it has already been shown that the UPC ratio obtained with a single daily sample is reliably correlated with collection over 24 h. 21 Proteinuria was observed in four cats in the PU group and in one cat in the PPU group. Post-renal proteinuria was ruled out in all of these cases, because sediments did not present significant alterations. 18 This reinforces the diagnosis of renal proteinuria. Renal proteinuria may occur as a result of glomerular loss, glomerulonephritis or hypertension, or a deficiency in tubular absorption. The last pathology is the most frequent in cats. 21 However, an important limitation to the determination of proteinuria in this study is that systemic hypertension and histologic evaluation could not be assessed.
In this study, the USG remained unaltered in some azotemic cats, as has been reported previously. 22 This may be because of the dietary intervention implemented in these animals or due to the cats’ hydration state, which have both been shown to influence USG, especially in the early stages of CKD.22–24
Conclusions
The main indications for urethrostomy are multiple catheterizations and urethral traumas, which may be avoided with careful clinical management. Cats that underwent urethrostomy showed bacteriuria, recurrent UTI and increased levels of SDMA. This highlights the importance of follow-up for the prevention and/or early treatment of urinary disorders. PU is associated with higher owner satisfaction and less symptomatic UTI and peristomal dermatitis than PPU. While PPU is important as a salvage procedure, it should be limited to cases in which standard techniques for PU cannot be performed.
Footnotes
Author note
Informed consent was obtained from the owners prior to the interview and for the use of data and pictures.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals (owned or unowned), and followed established internationally recognized high standards (‘best practice’) of individual veterinary clinical patient care. Ethical approval from a committee was therefore not necessarily required.
Informed consent
Informed, written consent was obtained from the owner or legal custodian of all animals described in this work for the procedures undertaken. For any animals or humans individually identifiable within this publication, informed consent for their use in the publication (verbal or written) was obtained from the people involved.