
Abstract
Case series summary
Described are four cats diagnosed with ophthalmomyiasis externa caused by Cuterebra larvae. Medical records were retrospectively reviewed to identify cats with ophthalmomyiasis externa between 2005 and 2020 at Cornell University Hospital for Animals. Signalment, history, clinical and diagnostic findings, treatment and outcome were recorded. All cats were young (< 3 years of age), had outdoor access and were initially examined during the summer months. All cases had unilateral disease with the right eye affected. Two cases had nictitating membrane lesions and two had orbital disease. Concurrent superficial corneal ulceration was present in three cats. Two cats suffered from pyrexia, suspected secondary to inflammation from the larval infestation. Successful larval removal was performed in all cats, which resulted in improvement of discomfort and clinical signs. A corneal ulcer persisted in one cat, which was lost to follow-up prior to ulcer resolution. Parasite identification confirmed Cuterebra species infestation in all cases.
Relevance and novel information
To the authors’ knowledge, this is the first report of feline ophthalmomyiasis externa caused by Cuterebra species. Parasite removal was successful in restoring comfort and resolving clinical signs in all cats with adequate follow-up information.
Introduction
Myiasis refers to dipteran fly larval infestation of tissues, while ophthalmomyiasis describes infestations of the eye. The expression ‘bot fly’ is commonly utilized to describe dipteran fly species that parasitize mammals such as the genera Cuterebra, Hypoderma, Oestrus and Gasterophilus. These parasitic infestations are found in many wild and domestic animal species. A small number of ophthalmomyiasis cases with infestation of intraocular and extraocular structures have been reported in dogs and cats.1–9 If the fly larvae are identified within the globe or within the orbit or adnexa, it is referred to as ophthalmomyiasis interna (OI) or ophthalmomyiasis externa (OE), respectively.
Cases of OE owing to Cuterebra species. have been reported in three dogs.1,2,10 However, only a single feline OE case report exists where reared adult males from eggs and larvae resting on the conjunctiva were identified morphologically as Lucilia sericata and Calliphora vicina, respectively. 9 Aside from one canine case with symblepharon requiring surgical correction to improve vision, manual removal of larvae was effective, resulting in comfortable and visual globes in all canine and feline cases of OE.1,2,9,10
Although Cuterebra is just one of the many parasitic genera in the dipteran order of flies, it is the genus most commonly reported in those cases of ophthalmomyiasis in dogs and cats where the larva was taxonomically identified.1–9 To the authors’ knowledge, no prior studies have documented OE caused by Cuterebra species. in cats. In addition, OE has not been reported in cats in the Americas. Medical records of cats evaluated by the ophthalmology service at Cornell University Hospital for Animals (CUHA) between 1 August 2005 and 1 October 2020 with a diagnosis of OE were identified. The purpose of this retrospective case series is to describe the historical, clinical and diagnostic features and therapeutic outcome of four cats with OE caused by Cuterebra larvae.
Case series description
Case 1
A 3-year-old intact female domestic mediumhair cat, weighing 3.9 kg, was presented at the end of July for evaluation of acute right periocular soft tissue swelling. Although a primarily indoor cat, the animal had access to a porch with a racoon infestation. The cat was dewormed as a kitten but had no other medical history and had never received a monthly preventive deworming treatment. The cat’s vaccination status was unknown.
Ophthalmic examination of both eyes (OU) was performed. Results of neuro-ophthalmic tests (palpebral reflex, menace response, dazzle reflex and pupillary light reflex) were normal OU. The right cornea retained fluorescein stain; the left cornea did not. There was moderate blepharospasm, marked chemosis and conjunctival hyperemia of the right eye (OD). Slit-lamp biomicroscopy OD revealed moderate third eyelid (TEL) elevation with visible larva spiracles (insect respiratory openings) immediately beneath the palpebral conjunctival surface of the TEL (Figure 1a). Proparacaine was applied topically prior to manipulating the TEL OD and before tonometry OU. The intraocular pressures (IOPs) obtained with rebound tonometry were 20 mmHG OU. Gentle retraction of the TEL using Colibri forceps allowed for complete assessment of the corneal surface and anterior ocular structures. A geographic, superficial corneal ulcer involved approximately 1/3 of the axial and ventronasal corneal surface and the anterior segment was unremarkable OD. Binocular indirect ophthalmoscopy was performed OD; the lens, retina and optic nerve head were normal. Complete ocular examination (slit-lamp biomicroscopy and indirect ophthalmoscopy following dilation with tropicamide ophthalmic solution) of the left eye (OS) was normal.
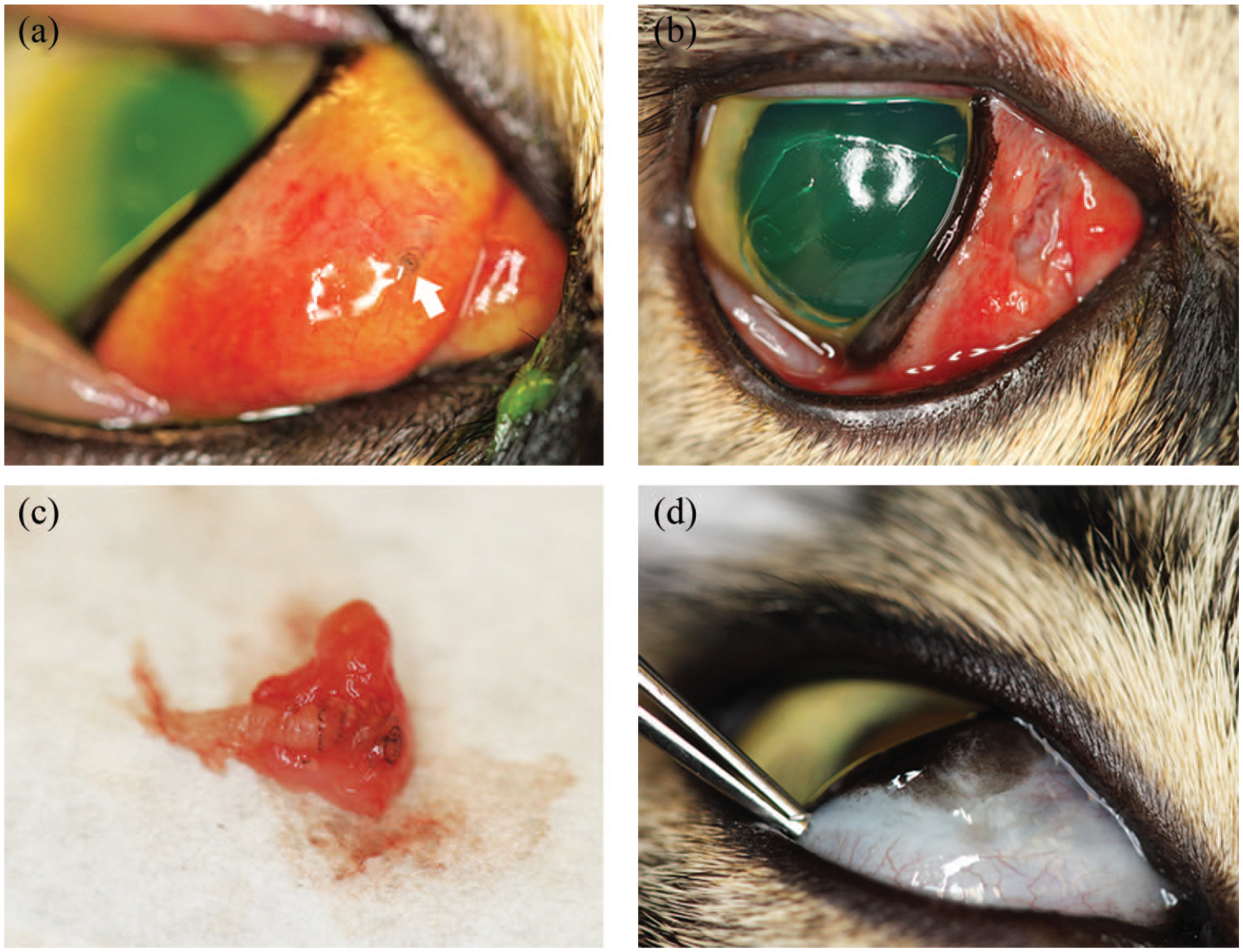
Clinical course of case 1 with ophthalmomyiasis externa: (a) clinical photograph at the initial ophthalmic assessment shows marked chemosis and conjunctival hyperemia, and moderate third eyelid (TEL) elevation with visible larva spiracles just beneath the conjunctival surface of the palpebral face of the TEL (arrow). An ~4 × 2 mm area of TEL conjunctiva and the parasite were removed using sharp dissection. The geographic superficial corneal ulcer is visible in (b). (c) The Cuterebra larva embedded within TEL tissues. The instar stage could not be subsequently determined. (d) Clinical photograph at the 3-week recheck reveals minimal scarring on the palpebral surface of the third eyelid. The corneal ulcer had healed at this visit
Physical examination was unremarkable aside from the ophthalmic findings. Following intravenous catheter placement, the cat was sedated with dexmedetomidine (10 μg/kg) and butorphanol (0.2 mg/kg) IV and placed in sternal recumbency. OS was lubricated and OD was lavaged with eyewash throughout the brief procedure. The right eye was routinely prepped and draped. Then, the eyelids were retracted using a Barraquer eyelid speculum. The TEL was exteriorized using Colibri forceps to better visualize its palpebral surface. An elliptical incision was made through the palpebral conjunctiva and around the embedded parasite using Westcott scissors. The parasite and approximately 4 × 2 mm of surrounding tissue was removed en bloc with blunt and sharp dissection using Westcott scissors. Care was taken to avoid severing the larva. The area was thoroughly searched for remaining larval tissue, but none was identified. The conjunctival surgery site was left open to heal by second intention (Figure 1b). The sedation was reversed with intramuscular atipamezole and the cat recovered uneventfully. Erythromycin ophthalmic ointment was applied OD following the procedure. The animal was sent home on amoxicillin-clavulanic acid (16 mg/kg PO q12h for 2 weeks), robenacoxib (6 mg PO q24h for 3 days) and erythromycin ophthalmic ointment (q6h OD until recheck).
The larva was submitted to the Cornell University Animal Health Diagnostic Center Parasitology Laboratory and was identified as a Cuterebra larva (Figure 1c). The posterior aspect of the larva was not intact, and the spiracles were not clearly visible; therefore, the instar (developmental stage) could not be confirmed.
Three weeks after initial presentation the owners reported the cat was doing very well at home. On ophthalmic examination, the superficial corneal ulcer had healed and there was minimal scarring on the palpebral surface of the TEL (Figure 1d). No other abnormalities were found on ophthalmic examination.
Case 2
A 5-week-old intact feral female domestic longhair cat , weighing 0.48 kg, was presented in late September with a suspected chronic globe rupture. The cat also had an approximately 2-week history of an open wound rostrotemporal to the base of the right ear and a punctate wound a few millimeters lateral to the lateral canthus OD. On physical examination there was a large, motile larva protruding anteriorly through and filling the entire palpebral fissure (Figure 2a). The right ear base wound was believed to be the breathing pore due to spiracle identification deep in the orifice. No other concerning abnormalities were found on physical examination.
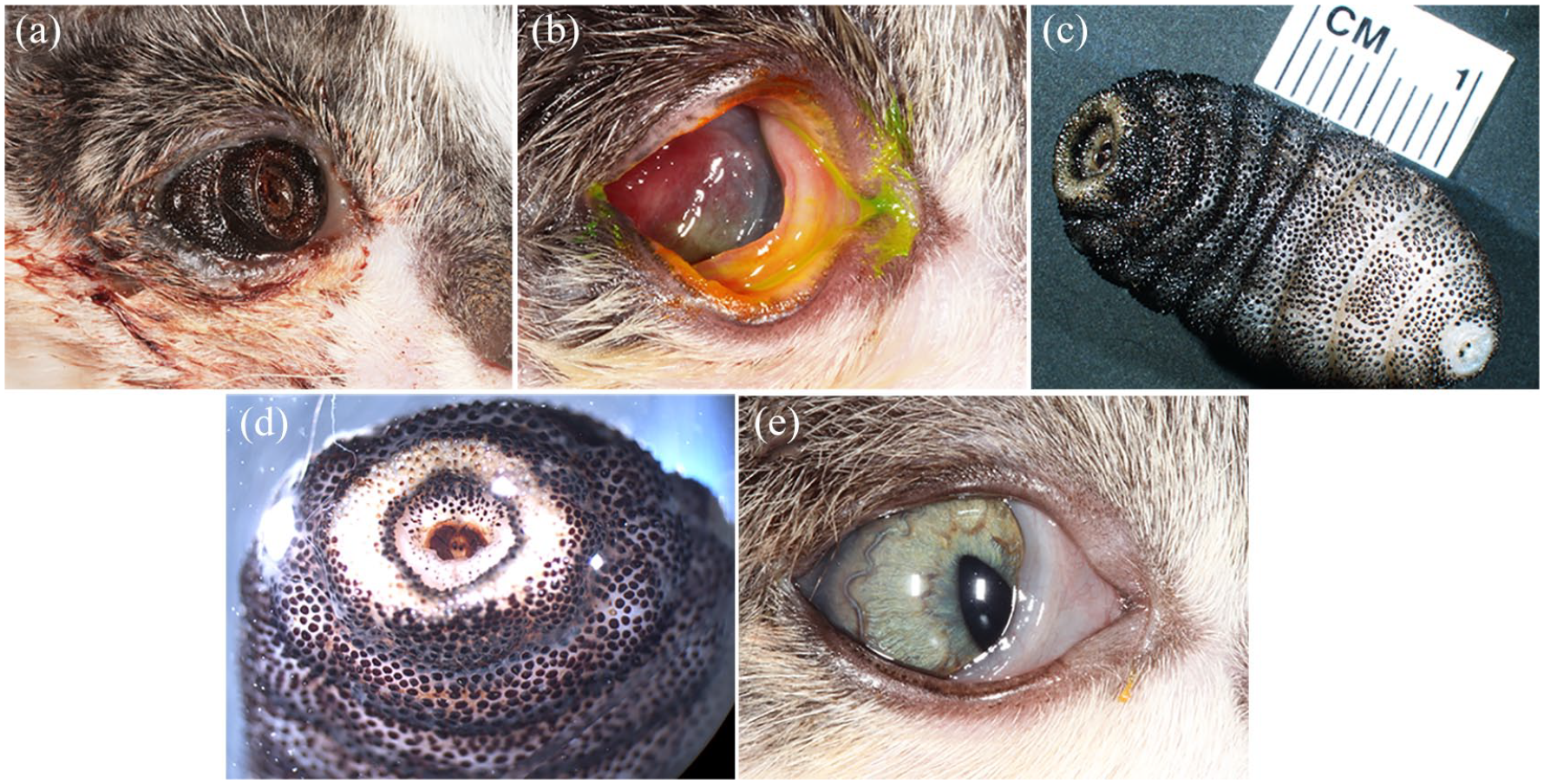
Clinical course of case 2 with ophthalmomyiasis externa: (a) clinical photograph at the initial ophthalmic assessment shows a larva filling the right palpebral fissure. (b) Following gentle, manual removal of the larva, the right globe was enophthalmic and ventronasally displaced. Owing to the globe displacement, conjunctival inflammation and corneal opacity, a complete ophthalmic examination could not be performed. (c) A third-stage larva of a Cuterebra species was recovered that was almost 3 cm in length (scale bar: 1 cm). (d) A magnified view of the larva spiracles can be seen in this posterior photograph of the mature bot. (e). Clinical photograph at the 2-week recheck revealed mild enophthalmos and third eyelid elevation, but the globe had returned to a more normal position and keratoconjunctivitis was largely resolved
The cat was part of a stray outdoor litter of five that lived under the porch of the new owners’ house. The owners appreciated abnormalities OD about 2 weeks prior to presentation but were only able to attain the kitten from its mother 4 days prior to clinical assessment. A few days before presentation, a referring veterinarian started the animal on amoxicillin–clavulanic acid (15 mg/kg PO q12h), meloxicam (0.05 mg/kg PO q24h) and erythromycin ophthalmic ointment (q12h OD). The wound on the side of the animal’s face was also treated topically with chlorhexidine scrub and neomycin sulfate, isoflupredone acetate and tetracaine hydrochloride dermal ointment twice daily. The kitten was treated with an unknown deworming medication prior to presentation.
Ophthalmic examination OD was limited due to the presence of a large, suspected Cuterebra larva and its surrounding inflammatory response that filled the right anterior orbit and protruded through the palpebral fissure, which prevented lid closure and examination of the right globe. B-mode ultrasonography was not diagnostic for periocular lesions. High frequency ultrasonography was performed to evaluate the extent of parasitism and confirm the presence of a globe. Although the larva prevented complete ocular assessment, an intact globe was appreciated. The neuro-ophthalmic examination was normal OS and there was a consensual pupillary light reflex from OD to OS. The left cornea did not retain fluorescein. Rebound tonometry estimated the IOP as 8 mmHg OS. Complete ocular examination OS was unremarkable.
As the parasite was already exposed through the palpebral fissure, proparacaine was administered topically OD, and the cat was gently restrained while larval removal was completed using Bishop-Harmon forceps. A large, intact, highly mobile larva was extracted from the right orbit and subsequently transferred to formalin. The larva was identified by parasitologist coauthors of this manuscript in the Department of Microbiology and Immunology based on morphologic features as a third instar Cuterebra species larva (Figure 2c–d).
No additional larvae were seen in the right orbit. A large empty warble (ie, a subcutaneous pseudocyst in which a larva of various bot flies resides 11 ) extended from the anterior aspect of the right orbit to the posteriotemporal aspect of the orbit where the ~2 mm circular warble pore was identified. A punctate full-thickness skin wound was also noted a few millimeters lateral to the right lateral canthus. Only moderately inflamed conjunctival tissue and a mildly thickened TEL could be clearly identified OD. Gentle retraction of the TEL using a cotton-tipped applicator allowed for partial visualization of the right globe, which was posteriorly and ventronasally displaced (Figure 2b). A formed globe with an edematous and ulcerated cornea could be appreciated deep in the orbit. Performance of the remaining ophthalmic examination was not possible due to poor visibility of the right globe. The owner did not consent to wound exploration and debridement, so the orbit was thoroughly lavaged with 0.5% dilute betadine solution. Topical therapy with neomycin and polymyxin B sulfates and gramicidin ophthalmic solution (q6h OD) was initiated. The owners were instructed to continue the previously prescribed amoxicillin–clavulanic acid and to discontinue the other medications prescribed by their local veterinarian.
At the cat’s 2-week recheck, the owners believed the animal to be comfortable and visual at home. Since the last recheck, the cat was eating well and was apparently healthy. The cat had finished the course of amoxicillin–clavulanic acid prior to recheck. On ophthalmic examination, the wounds near the base of the cat’s right ear and next to the ipsilateral lateral canthus had healed. There was mild enophthalmos and TEL elevation, but the globe position had significantly improved (Figure 2e). The IOPs were 12 mmHg OD and 13 mmHG OS. Neuro-ophthalmic examination was normal OU. The Schirmer tear test results were 7 mm/min OD and 8 mm/min OS. Neither cornea retained fluorescein. On slit lamp biomicroscopy, the temporal peripheral right cornea had mild superficial fibrosis and vascularization. The anterior chamber was clear, and the lens was normal OU. On fundoscopy, the retina and optic nerve were unremarkable OU. Owing to the examination findings, the topical ophthalmic antibiotic was discontinued, and the cat was started on a sorbitol and carbomer gel eye lubricant (q8h OD) until recheck.
Five weeks after initial presentation, the owners reported that the cat was doing very well at home. The cat’s ophthalmic examination findings remained static from the last visit.
Case 3
A 4-month-old intact female domestic shorthair cat, weighing 1.6 kg, was presented in early August for evaluation and treatment of acute serosanguineous ocular discharge OD. The serosanguineous ocular discharge was noted by the cat’s owner the day prior to presentation and was thought to have resulted from a backyard chicken pecking the kitten’s eye, although the event had not been witnessed. Additionally, the owner believed the kitten had been losing weight prior to presentation. The cat was part of an unvaccinated, outdoor litter of five with no previous history of veterinary care or deworming.
Physical examination revealed a fever of 105.3°F, a distended, soft, non-painful abdomen and moderate blepharospasm OD. A complete ophthalmic examination was performed OU. Neuro-ophthalmic responses and reflexes were intact OU. Neither cornea retained fluorescein. Proparacaine was applied topically prior to manipulating the TEL OD and before tonometry OU. The IOPs, estimated with applanation tonometry, were 16 mmHg OD and 13 mmHg OS. Slit-lamp biomicroscopy OD revealed moderate blepharospasm with TEL elevation. There was no evidence of periocular or ocular injury, although moderate eyelid swelling was noted inferonasally OD. Approximately 50% of the ocular surface was covered by a protruding and thickened TEL. Moderate diffuse conjunctival hyperemia and chemosis was also present OD. At the inferonasal anterior aspect of the TEL, suspected bot spiracles were seen protruding from a punctate ulcerated conjunctiva with evidence of previous hemorrhage (Figure 3a). Gentle retraction of the TEL using Colibri forceps allowed for evaluation of the nasal anterior ocular structures and revealed a normal anterior segment in the right eye. Binocular indirect ophthalmoscopy was performed OD; the lens, retina and optic nerve head were normal. Results of a complete ocular examination OS were normal.

Clinical course of case 3 with ophthalmomyiasis externa: (a) clinical photograph at the initial ophthalmic assessment shows third eyelid (TEL) elevation with moderate diffuse conjunctival hyperemia and chemosis. A superficial corneal ulcer was not present. The spiracles of the larva cannot be seen in this photograph but were in the vicinity of the arrow. (b) Manual removal of the larva using Debakey forceps left a ~1–2 mm diameter orifice in the inferonasal third eyelid (arrow). (c) A second instar Cuterebra larva was recovered (scale bar: 1 mm). (d) At the 2-week recheck, the warble pore was surrounded by a dense bed of fibrotic tissue with extension of the exuberant tissue (arrow) full thickness through the TEL. This resulted in mechanical irritation to the corneal surface and a secondary superficial corneal ulcer. (e) At the 4-week recheck, symblepharon of the palpebral face of the TEL and palpebral conjunctiva of the inferior lid was present (arrow)
The cat was easily handled with gentle restraint. The ulcerated conjunctiva was covered with a generous amount of petrolatum ophthalmic ointment for 10 mins in an attempt to stimulate the parasite to emerge partially out of the opening. A larva moved to the periocular surface through the pore and was removed using Debakey forceps. The small intact larva was placed in formalin for later identification. The open wound was closely examined for any remaining larva and evidence of non-viable tissue or overt bacterial infection (Figure 3b). No concerning abnormalities were found on orbital and periorbital B-mode ultrasonography. An Elizabethan collar was placed immediately after examination. Owing to financial constraints, the owner did not consent to bloodwork (complete blood count, serum biochemistry, and feline immunodeficiency and feline leukemia virus tests), wound exploration or debridement under general anesthesia. Topical ofloxacin ophthalmic solution (q6h OD) and oral clindamycin (23.4 mg/kg PO q24h) were prescribed. Selamectin (15 mg) was applied to the haired skin between the scapulae, and nitenpyram (11.4 mg) and praziquantel/pyrantel pamoate (18.2 mg and 72.6 mg, respectively) were given orally prior to discharge from the hospital. The larva was submitted to the Cornell University Animal Health Diagnostic Center Parasitology Laboratory and was identified by morphologic features as a second instar Cuterebra larva (Figure 3c).
The cat returned 2, 4 and 5 weeks after initial presentation. Although visual and apparently comfortable, the cat had impaired TEL movement as a result of symblepharon formation and persistent corneal ulceration. The corneal ulcer was believed to be related to mechanical irritation from exuberant tissue extending to the posterior surface of the TEL and deepened at all following rechecks (Figure 3d,e). At the last recheck for that cat, the corneal stroma surrounding the ulcer appeared to have cellular infiltrate so corneal cytology was performed, which revealed few non-degenerate neutrophils and eosinophils. No infectious agents were identified on cytology, and culture was not performed as the clients declined further diagnostic tests.
Owing to concern for immune-mediated eosinophilic keratitis, possibly initiated by the previous parasitic infection, the cat’s therapy was adjusted to include an immuno-modulatory medication (ie, cyclosporine 2% solution q12h OD), while all other treatments were discontinued and replaced with oxytetracycline ophthalmic ointment (q6h OD). The cat was lost to further follow-up.
Case 4
A 1-year, 3-month-old, castrated male domestic shorthair cat, weighing 4.1 kg, was presented in early August for inappetence, lethargy and coughing and wheezing sounds noted for a week. The owners also noted neck extension during swallowing and open-mouth breathing. The cat was initially an indoor-only cat but had gained outdoor access approximately 1 month before developing these clinical signs.
Physical examination findings were unremarkable aside from a fever of 105.9°F. The cat was sedated with midazolam (0.2 mg/kg IV) and given hydromorphone (0.5 mg/kg IV). Results of a complete blood count and serum biochemistry were unremarkable. Thoracic and abdominal radiographs were normal aside from mild splenic enlargement believed to be secondary to sedation. The animal was sent home on lactated Ringer’s solution to be administered subcutaneously (60 ml q6h) and amoxicillin–clavulanic acid (15.2 mg/kg PO q12h for 3 weeks).
Ten days after initial presentation, the animal presented again owing to persistent difficulty while swallowing. At that visit, the owner also reported that the cat had an elevated TEL OD and had been pawing at OD for 1 week. On physical examination, the right periorbital soft tissues were swollen and erythematous. A ~5 mm scab was present rostral to the right ear and the cat appeared to experience pain during right periorbital palpation and retropulsion. At that point, the Ophthalmology Service was consulted, and mild exophthalmos was appreciated (Figure 4a). There was also marked reduction during retropulsion OD. The rest of the ophthalmic examination findings were unremarkable. Oral examination revealed soft tissue swelling in the right pterygopalatine fossa. The right submandibular lymph node was larger than the left, but no other lymphadenopathy was appreciated.

Clinical course of case 4 with ophthalmomyiasis externa: (a) clinical photograph at the initial ophthalmic assessment shows mild exophthalmos and third eyelid elevation of the right eye. A skin wound at the base of the right ear is not visible in this image. A third-instar larva of Cuterebra species was surgically removed from the subcutaneous lesion extending from the adjacent orbit (b)
A presumptive diagnosis of a right retrobulbar abscess or cellulitis was made. Orbital ultrasound findings supported a soft tissue mass/abscess posterior to the right globe. The animal was sedated with diazepam (0.5 mg/kg IV) and ketamine (10 mg/kg IV). Then, a mouth speculum was placed, and a stab incision was made in the right pterygopalatine fossa. Using blunt dissection, the retrobulbar area was bluntly explored, but no purulent material was expressed. Samples were collected from the incision in the oral cavity for cytologic assessment and aerobic and anaerobic bacterial cultures. Pterygopalatine fossa cytology was non-diagnostic. The large scab rostral to the ear was removed to clean the area. The wound was believed to be the breathing pore due to spiracle identification deep in the orifice within the retrobulbar space. The botfly was manually removed and was identified as a third instar Cuterebra larva by the parasitologist co-authors of this manuscript (Figure 4b). Wound cytology revealed a moderate number of degenerate polymorphonuclear cells and eosinophils.
The owner was instructed to continue the oral antibiotic as previously prescribed until the culture results returned and was sent home with a tapering course of oral prednisolone (1.2 mg/kg q12h for 5 days, then q24h for 5 days, then every other day for five doses). Ivermectin (1300 mg subcutaneously weekly for three doses) was also sent home to eliminate any remaining larvae. Few Pasteurella species were cultured on the retrobulbar swab, but antibiotic susceptibility was not available. A couple of weeks after discharge, the owners were called and reported complete resolution of the clinical signs.
Discussion
The peak Cuterebra species infection period in the northern USA is observed in the late spring to summer months.12–15 Cuterebra eggs will hatch in response to a sudden increase in temperature. 14 During the transition into the warm season, the region in which the cats in this case series resided typically experiences temperature elevation from freezing to an average daily high temperature range between the upper 16 to 32°C, greatly increasing the potential for larval hatching. As expected, therefore, all infections in this series were detected from July to September.
Treatment of cuterebriasis causing morbidity includes manual removal of larvae.1,2,16–19 This is especially true in atypical hosts, as typical hosts rarely develop clinical signs associated with infestation. 20 Favored methods for larval removal in OE cases include manual removal following application of local anesthetic and putative larval suffocation with petroleum jelly applied over the respiratory orifice. The latter is suggested to cause the larva to partially extrude itself from the warble to avoid asphyxiation. 21 Asphyxiation may not be an actual result after applying lubrication over the warble pore site, since some OI cases have apparently live intraocular larvae despite being surrounded by fluid. However, a combination of both techniques was utilized in case 3 due to poor visibility of the early-stage larva in a limited working space. The larva in case 1 was securely embedded within the TEL soft tissues as the warble pore was not yet developed, so surgical excision with narrow tissue margins was employed to ensure complete removal of the larva. Since the larvae in cases 2 and 4 were easily visualized and accessible, manual removal by gently grasping the larvae was successful.
Removal of the entire larva in one piece is considered essential as fragmented larvae may cause anaphylaxis or severe hypersensitivity reactions.22–24 The orifices are left to heal by second intention. Administration of diphenhydramine and dexamethasone before or after larval removal has been recommended to help in the case of larval rupture during the removal process.16,17,25 Since, in the present series, all larvae were believed to be removed intact in all cases, no injectable antihistamines or corticosteroids were administered. However, during parasite identification in case 1 the posterior aspect of the instar was noted not to be intact. This cat recovered without complication.
The avermectins may be effective against dipteran larvae. 26 Despite ivermectin being shown to have a large safety margin in cats, inappropriate use can cause serious toxicosis resulting in blindness, coma, and death.27,28 Given the possibility of a severe inflammatory reaction from a dying larva following systemic larvicidal therapy such as ivermectin, the use of such therapy is not advised if it can be avoided. 20 One exception is with central nervous system cuterebriasis, where the benefits of ivermectin use can outweigh the risks of withholding treatment. 25 Ivermectin is occasionally used in an extra-label manner to treat some parasites as in case 4 in this series treated in 2005. 29 Although ultrasonography was used to confirm absence of further parasitic infestation in the orbit, ivermectin administration was continued at home in that cat. Therefore, a tapering course of oral corticosteroids was also prescribed to reduce the risk of a potential hypersensitivity reaction from any additional larval death. Because ivermectin can have serious adverse effects in humans, the possible risks associated with its use and handling were communicated to the owners. Although no complications from ivermectin therapy were reported in that cat, medical practices concerning ivermectin have since changed and the medication was not utilized in the remaining cases in this report.
Fevers at the time of presentation in two cats in the present series (cases 3 and 4) may have represented a response to secondary bacterial infection or a hypersensitivity reaction to the parasite in an atypical host. The lack of diagnostic testing in case 3 makes this impossible to determine; however, in case 4, further systemic assessment did not identify other possible causes for fever. As severe systemic signs resulting solely from Cuterebra species infestations have been documented in small animals, clinicians should be aware of potential systemic manifestations of this parasite. 20 Empirical oral administration of broad-spectrum antibiotics was employed in all cases of the current series due to fever or presence of an open wound. All eyes with corneal ulceration received empirical antimicrobial therapy selected based on what was considered standard of care at the time.30,31 Individual veterinary ophthalmologist antibiotic choices are further supported by the most common bacterial isolates and antimicrobial susceptibility patterns for cats with bacterial keratitis. 32 In addition to antibiotic therapy, nitenpyram was administered in case 3, since this medication is effective for treating other causes of primary myiasis. 33
The eosinophilic corneal infiltrate observed on cytology months after Cuterebra species removal in case 3 was unexpected. An accumulation of eosinophils often occurs in hypersensitivity disorders, neoplasia and parasitic infestation. 34 Since the corneal cellular infiltrate was not noted until 5 weeks following larval removal and there was progressive stromal loss, other causes for the eosinophils on corneal cytology were considered. Corneal tissue infiltration with eosinophils is particularly linked with feline eosinophilic keratoconjunctivitis (FEK) in cats. 35 An aberrant immune-mediated condition or result of a concurrent infection with feline herpesvirus (FHV-1) are commonly described etiopathogeneses for FEK.36–38 In that case, the authors considered initial larval infestation inciting FEK as a possibility. An initial topical corticosteroid course followed by a longer course of cyclosporine is considered the treatment of choice for FEK by some. 39 In the cat we describe (case 3), antibacterial drugs were administered topically for weeks but the corneal lesion failed to resolve. Herpetic disease was considered unlikely as the sole reason for non-healing, since herpetic ulcers are typically confined to the epithelial layer. 40 Chronic mechanical trauma from the diseased conjunctival tissue on the bulbar surface of the TEL was believed to be the underlying cause for corneal ulcer persistence and stromal loss.
Prevention of myiasis would be preferable to treatment, considering the potential risks to vision and quality of life. There needs to be establishment of a safe and effective preventative strategy to inhibit these infestations by eliminating larvae before their development in the host tissues. Further research into deworming and larvicidal medications to prevent and treat Cuterebra species infestations is warranted.
Conclusions
To the authors’ knowledge, these are the first reported cases of Cuterebra larval infestation in the extraocular tissues of cats, and the first report of feline OE in the Americas. Comparable to earlier OE,1,2,9 manual removal was successful in improving animal comfort and clinical signs. In the present series, only one cat (case 3) developed notable complications following larval removal; that cat had chronic corneal ulceration and symblepharon formation, similar to one canine OE case. 10 This case series confirms that second-intention healing accompanied by appropriate antibiotic therapy is appropriate for resolution of warbles.1,41,42 Although manual removal was successful in some cases, debridement of non-viable tissue may also be warranted to allow for uncomplicated healing and to provide the best functional and visual outcome.
Footnotes
Conflicts of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.