
Abstract
Practical relevance:
Feline carpal injuries are usually caused by falls from a height that result in hyperextension injury or antebrachiocarpal luxation or subluxation. Isolated ligamentous damage or fracture of the carpus is unusual; it is more common to have a combination of both in the cat. These injuries can be debilitating since cats climb and jump from great heights, and have a greater range of antebrachial pronation and supination than dogs.
Anatomy:
There are differences in the anatomy of the feline and canine carpus. In particular, cats only have a single short radial collateral ligament, also known as the medial collateral ligament. This means that, in the cat, antebrachiocarpal subluxation is possible with rupture of the dorsal joint capsule and short radial collateral ligament alone.
Clinical challenges:
Many feline carpal injuries can be treated without performing pancarpal arthrodesis. However, determining which ligaments and joint levels are affected requires careful examination and often stress radiography. When pancarpal arthrodesis is performed in the cat, it has been reported to reduce the height of jumping and to increase reluctance to climb. This is speculated to be due to reduced pronation and supination movement of the carpus.
Evidence base:
The current evidence base for management of feline carpal injuries is grade III or IV, with most of the studies being retrospective case series involving cadaveric dissection or direct extrapolation from published information about the dog. There are few guidelines regarding the optimal treatment options for carpal injuries in the cat.
Anatomy
The feline carpus is a multi-compartmental unit that consists of three joint levels and several smaller intercarpal joints. 1 The joint levels include the antebrachiocarpal, middle carpal and carpometacarpal joints.
The antebrachiocarpal joint comprises the distal end of the radius and ulna, which articulate with the radial carpal and ulnar carpal bones, respectively. The accessory carpal bone forms part of the proximal carpal row; it articulates with the ulna and the palmar aspect of the ulnar carpal bone. 1 The flexor carpi ulnaris muscle inserts on the apical portion of the accessory carpal bone. 2
The middle carpal joint is formed by the articulation of the numbered carpal bones (I–IV) with the radial and ulnar carpal bones. Distal to the numbered carpal bones is the carpometacarpal joint. The numbered carpal bones at this level articulate with the metacarpal bones (Figure 1).

Three-dimensional CT reconstruction of a feline carpus, dorsal view. Carpal bone 1 is not shown. RCB = radial carpal bone; UCB = ulnar carpal bone; ACB = accessory carpal bone; CII–IV = carpal bones; MCII–V = metacarpal bones
The passive stabilisers of the feline carpus include the joint capsule, palmar fibrocartilage and ligaments. There are few reports on normal feline carpal ligament anatomy, with most anatomical texts referring to ligament origins and insertions in the dog.1,2 A summary of origins and insertions of feline carpal ligaments is included in Table 1.
Ligament origins and insertions of the feline carpus

Adapted from Basa et al 3
Previous authors have demonstrated that the anatomy of the feline short radial collateral ligament differs from that of the dog. 4 In particular, the short radial collateral ligament of the cat consists of a single broad ligament that has its origin at the dorsoproximal aspect of the distal radius and inserts on the palmarodistal aspect of the radial carpal bone (Figure 2). 4 In the dog, this ligament consists of superficial and deep portions that are separated by the tendon of the abductor pollicus longus muscle. 5 The biomechanical function of these ligaments has not been investigated.

Anatomical dissection of the medial aspect of the carpus. The asterisk corresponds to the tendon of the abductor pollicis longus, and deep to this is the short radial collateral ligament. This ligament courses obliquely from the dorsomedial surface of the radius to the palmar surface of the radial carpal bone (yellow line shows approximate course)
Normal joint range of motion
In cats, the normal standing angle of the carpus relative to the antebrachium is 160–180°, while in dogs this angle is slightly less at 140–180°. 1 The greatest range of joint motion in cats and dogs occurs at the antebrachiocarpal joint (85–90%), followed by the middle carpal joint (10–15%); there is little to no movement at the carpometacarpal joint. 1 Cats also tend to have a greater degree of carpal valgus displacement than dogs, which is apparent on manipulation of the paw.
The carpus is traditionally considered to be a ginglymus (hinge) joint, with physiological carpal hyperextension in the cat reported to be 15°. 6 It is known that cats have a greater range of supination and pronation (115°) than dogs (50°).7,8 The features of the feline carpus that give rise to this include a flexible interosseous (radius/ulna) membrane, differences in the collateral ligaments of the elbow and the presence of a large ulnar styloid process. 8
There are no anatomical descriptions of the interosseous membrane in the cat. However, as in people, this structure is thought to contribute to rotational stability of the antebrachium. 9 The feline elbow also has a stronger olecranon ligament, which is twice the width and a third of the length of its counterpart in the dog. 7 This ligament extends from the lateral side of the olecranon to the medial side of the humeral condyle and is speculated to be an evolutionary adaptation contributing to increased supination. 8
Cause and type of carpal injuries
Feline carpal injuries are commonly caused by ‘high-rise’ syndrome or motor vehicle accidents. The reported incidence of carpal injuries in one epidemiological study of feline high-rise syndrome was 0.29%. 10 The antebra-chiocarpal joint is most commonly injured, followed by the carpometacarpal and middle carpal joints. 11 The reported frequency of feline carpal injuries associated with high-rise syndrome varies; in one report on 119 cats, no carpal injuries were sustained, while in a report on 107 cats in Israel, 4.7% were diagnosed with carpal bone fracture.10,12
The current literature on feline carpal injuries is summarised in Table 2. In the largest case series of feline carpal injuries to date, 40/73 cats had injuries to another limb. 6 The antebrachiocarpal joint was more likely to be affected by a fall from the fourth floor or higher, whereas carpometacarpal joint injuries occurred with falls from a height up to the third floor. This difference in affected carpal rows is likely to be due to landing dynamics – cats falling from a greater height tend to fall evenly on all four paws while, with falls from lower heights, the cat tends to land on outstretched forelimbs first. In the same case series study, 25% of the injuries were attributed to carpal hyperextension. 6
Cases of feline carpal injury reported in the literature (n = 109)
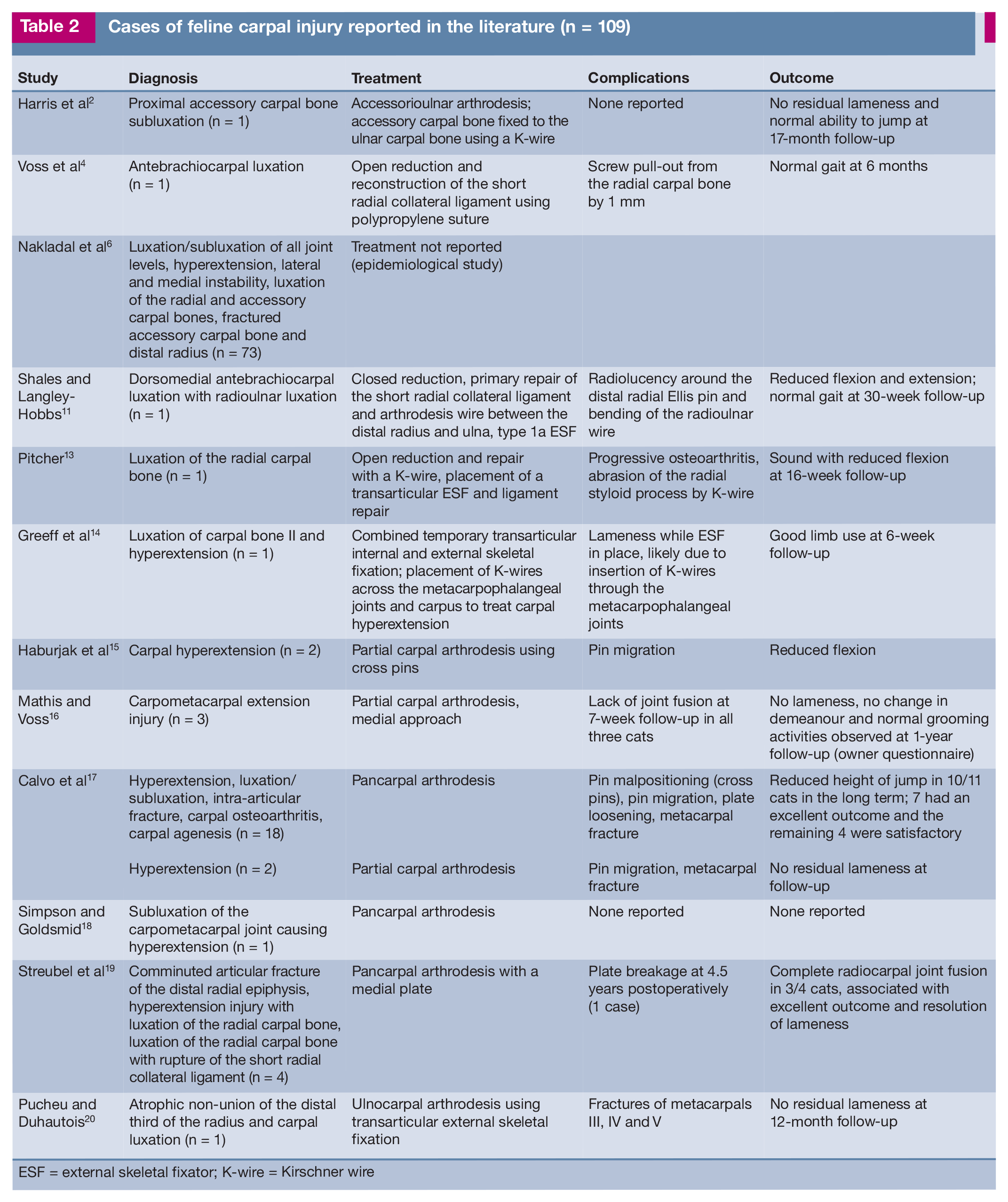
ESF = external skeletal fixator; K-wire = Kirschner wire
Carpal hyperextension is associated with damage to the palmar fibrocartilage, flexor retinaculum, palmar ligaments or a combination of these structures. 11 In the dog, it is the most common carpal injury, with the distribution of injuries being 31% at the antebrachiocarpal joint, 22% at the middle carpal and 40% at the carpometacarpal joint in one case series. 21
Physical examination
Cats with traumatic carpal injuries will typically be presented with mild to complete non-weightbearing unilateral forelimb lameness. In the case of hyperextension injuries, there is often a more palmigrade stance compared with the contralateral limb, and a palpable joint effusion (Figure 3). With a clear history of trauma, the presence of crepitus may be suggestive of carpal bone fracture. In the case of bilateral hyperextension, and in the absence of known trauma, it is prudent to perform arthrocentesis to rule out inflammatory joint disease.

(a–c) Stance of a cat with carpal hyperextension injury. In images (b) and (c) the cat has a palmigrade stance associated with the left carpus. Images courtesy of Dr Rui Sul, University of Sydney Veterinary Teaching Hospital
Assessment of ligamentous instability may need to be performed with the patient sedated to facilitate a complete orthopaedic examination. Subtle instabilities can be missed in the conscious cat, especially if the carpus is painful. Dorsopalmar stress is applied to the antebrachiocarpal, middle carpal and carpometacarpal joints (Figure 4). The presence of ‘drawer’ movement suggests damage to the dorsal joint capsule; in some cases, the dorsal radiocarpal ligament may also be damaged at the level of the antebrachiocarpal joint. 4 Since there is variability between individual cats in the degree of carpal extension normally seen, the contralateral carpus is used as a point of reference. 4

(a–c) Physical examination of a cat with a carpal hyperextension injury. Images show (a) flexion stress, (b) stress in extension and (c) varus stress. The cat was given light sedation prior to examination. Images courtesy of Dr Rui Sul, University of Sydney Veterinary Teaching Hospital
Valgus and varus stress is applied to assess the integrity of the short radial and short ulnar collateral ligaments, respectively. In cadaveric feline limbs, transection of the short radial collateral ligament in combination with rupture of the dorsomedial joint capsule resulted in complete antebrachiocarpal luxation. 4 Therefore, in cats, injury to this ligament must be considered as part of the diagnostic workup for subluxation or luxation of the antebrachiocarpal joint; by contrast, in dogs, antebrachiocarpal (sub)luxation requires multiligamentous injury (short radial collateral, short ulnar collateral, radiocarpal and ulnocarpal ligaments) and damage to the joint capsule. 11 It is speculated that injury to the short ulnar collateral ligament is relatively uncommon in the cat because normal physiological valgus posture of the distal forelimb places greater tensile load on the medial aspect of the carpus.4
Diagnosis
Currently, the diagnosis of feline carpal injuries relies upon manual palpation and radiography. Plain radiography with dorsopalmar and mediolateral views can assist in the detection of carpal bone fracture or luxation; however, if there is suspected ligamentous damage and instability this is often used in conjunction with stress radiography.
Stress radiography
Stress radiography includes varus and valgus stress views as well as use of flexion and extension stress techniques. An abnormal valgus or varus stress view suggests damage to the short radial collateral and short ulnar collateral ligaments, respectively, while hyperextension may be due to damage to the palmar fibrocartilage. 4
Interpretation of stress radiographs is more difficult in the cat than the dog due to the small size of the carpal bones. Both carpi should be radiographed with similar degrees of stress applied (preferably by the treating clinician) so that differences in joint space symmetry can be assessed. Where there are minor differences in joint symmetry, the authors recommend relying on manual palpation and concurrent findings such as the presence of joint effusion.
Computed tomography
CT allows more accurate detection of carpal bone fracture or luxation (Figure 5), due to the small size of the carpal bones and their superimposition on radiographs. CT has previously been used to differentiate radial carpal bone fracture in dogs where there was suspected incomplete fusion of ossification centres, and to describe normal topography of the carpal canal.3,22,23
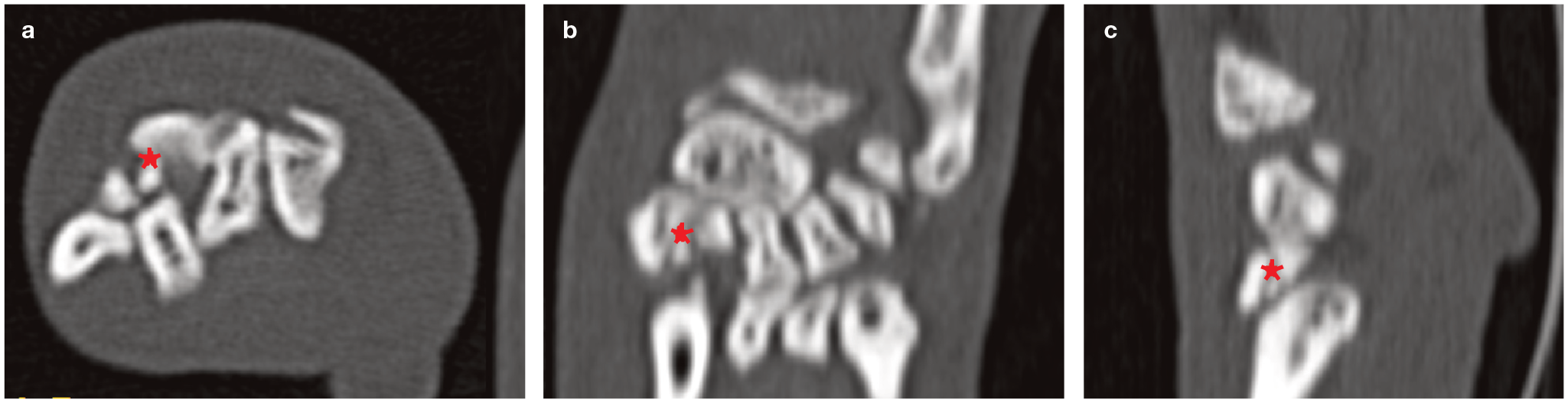
(a–c) Multiplanar reconstruction from a feline carpal CT study confirming the presence of multiple fractures of the distal row of carpal bones. The fractures were not apparent on radiographs due to superimposition of the carpal bones. The asterisk in each of the images demonstrates fracture of carpal bone II. (a) Transverse image just proximal to the metacarpus; (b) dorsal plane image sectioned mid-carpus; (c) sagittal image mid-antebrachium
Magnetic resonance imaging
Experimental studies in the dog and cat using low- and high-field MRI, respectively, described the normal appearance of the carpal ligaments (Figure 6).3,24 This imaging modality is used in the diagnosis of equine intercarpal ligament injuries and cartilage lesion defects. 25 It may have future application in diagnosing feline carpal ligament injuries.
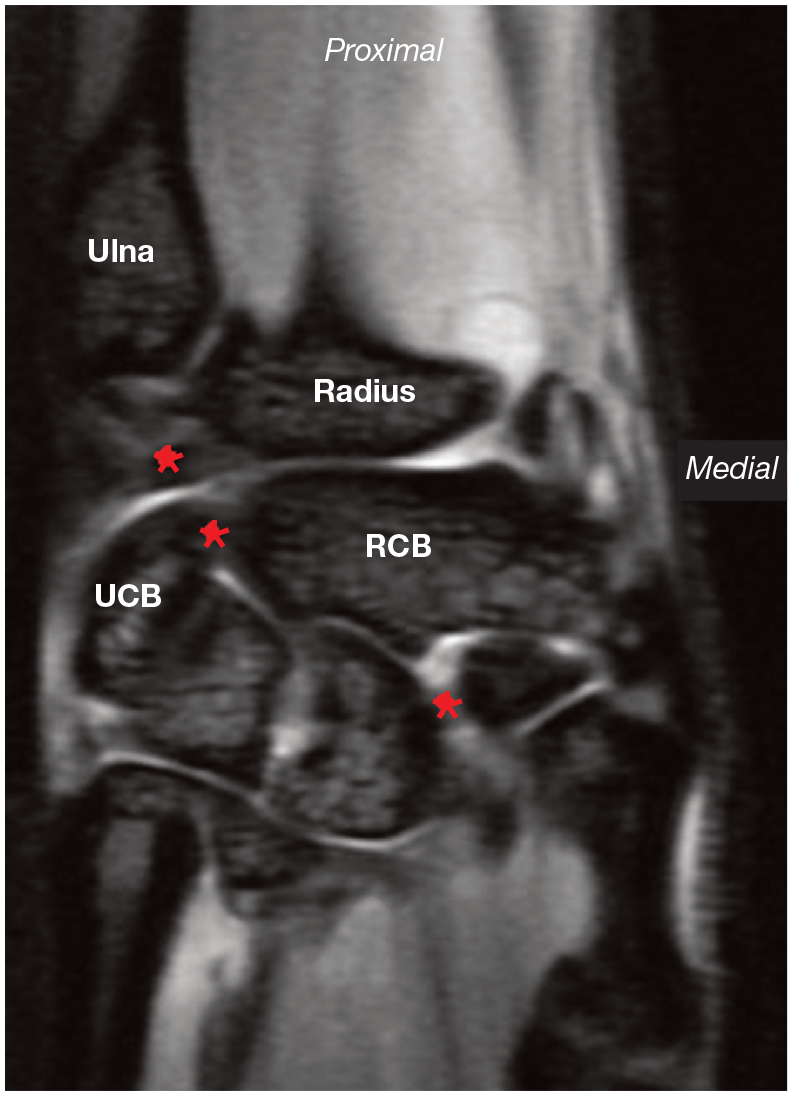
Dorsal plane 3T MRI image of the feline carpus (T1-weighted image). The asterisks correspond to the carpal ligaments, seen as transverse hypointense bands. The most proximal asterisk is the radioulnar ligament, and the other two correspond to the smaller intercarpal ligaments. UCB = ulnar carpal bone; RCB = radial carpal bone
Surgical approaches to the carpus
The most commonly performed approaches to the carpus are dorsal, medial, palmaromedial or palmarolateral. 26 In cats, unlike the dog, the tendon of the extensor carpi radialis branches to become the extensor carpi radialis longus inserting on the dorsal surface of the second metacarpus, and the extensor carpi radialis brevis inserting on the dorsal surface of the third metacarpus; this is important to note when making the dorsal approach. 27

Dorsal approach to the carpus (cadaver specimen). An incision has been made between the tendon of the extensor carpi radialis and the tendon of the common digital extensor. The extensor carpi radialis is retracted on the left side of the image, and the common digital extensor on the right side. The joint capsules of the antebrachiocarpal and middle carpal joints have been incised. RCB = radial carpal bone; UCB = ulnar carpal bone

Palmaromedial approach to the carpus. The asterisk indicates the palmar aspect of the radial carpal bone. The overlying flexor retinaculum and joint capsule have been incised and retracted

Palmarolateral approach to the carpus. The asterisk indicates the accessory carpal bone. FCU = flexor carpi ulnaris; AML = accessoriometacarpal ligament
Closure
Where there is enough remaining joint capsule, this can be closed using absorbable suture in a simple continuous or simple interrupted pattern. Deep and superficial fascial layers are closed prior to skin closure. 28
Specific feline carpal injuries
The following sections describe a range of carpal injuries and their treatment approaches, a summary of which is provided in Table 3.
Summary of carpal injuries, surgical approaches and recommendations for treatment

K-wire = Kirschner wire
Fracture of the distal radial and ulnar styloid processes
Fractures of the distal radial and ulnar styloid processes result in instability of the antebrachiocarpal joint due to disruption of the insertion points for the short radial collateral and short ulnar collateral ligaments, respectively.27,30 Open reduction and internal fixation are, therefore, indicated. A palmaromedial (radial styloid process) or palmarolateral (ulnar styoid process) approach provide the best exposure. 27 These fractures are amenable to fixation with Kirschner (K)-wires and a tension band wire, or a lag screw.
Treatment for fracture of the radial styloid process can be achieved using two parallel K-wires inserted through the radial styloid process and driven in an oblique proximolateral direction through the lateral cortex of the radius. 29 Orthopaedic wire (0.8–1 mm) is then placed through a hole drilled in the radius 1 cm proximal to the fracture and around the ends of the K-wires, and secured in a figure-of-eight pattern to create a tension band.26,31 Owing to the small size of the fragments, further fracture is a risk. Therefore, the authors recommend applying slow and even tension during wire tightening. Where there is a larger fragment, a single lag screw (no greater than a 2.4 mm cortical screw) and K-wire, placed in the same direction as the paired K-wires, could be used.26,31
A similar method of fixation is used for fractures of the distal ulnar styloid process, except that only a single K-wire and tension band is used, due to the smaller size of the medullary canal.26,29,31 Alternatively, the K-wire can be driven obliquely from the ulnar styloid process to the distal radius to prevent pin migration, but would need to be removed following fracture healing due to restricted pronation and supination.26,31
External coaptation with a modified Robert Jones bandage and caudal splint should be used for 4 weeks postoperatively, to prevent pin migration and implant failure.
Carpal joint luxation and subluxation
Antebrachiocarpal joint
Disruption of the short radial collateral ligament can either occur in isolation, or in conjunction with complete antebrachiocarpal subluxation or luxation caused by simultaneous rupture of the dorsomedial joint capsule. Antebrachiocarpal luxation can occur either dorsally or in a palmar direction. In the cat, it tends to be in a palmar direction, likely due to the oblique course of the short radial collateral ligament (the angle between the longitudinal axis of the radius and the medial collateral ligament is approximately 100°).4,29 Complete luxation of the antebrachiocarpal joint is not as commonly associated with hyperextension as it is in dogs; however, the integrity of the short ulnar collateral ligament and palmar ligaments and fibrocartilage should also be assessed (see below). Arthrodesis should be considered in cases of antebrachiocarpal joint subluxation or luxation with concurrent hyperextension injury.
Diagnosis of an isolated short radial collateral ligament injury can be made using stress radiography. In the cat, valgus stress does not create significant medial opening of the joint spaces, despite the presence of an injured short radial collateral ligament. Varus stressed radiographs are often more useful because the radial carpal bone displaces in a mediopalmar direction (Figure 10).4,29 In the presence of antebrachiocarpal luxation, there is often a positive drawer sign, with palmar displacement of the manus relative to the antebrachium. Inward rotation of the paw with flexion of the carpus will often induce palmar luxation of the carpus following closed reduction. 4
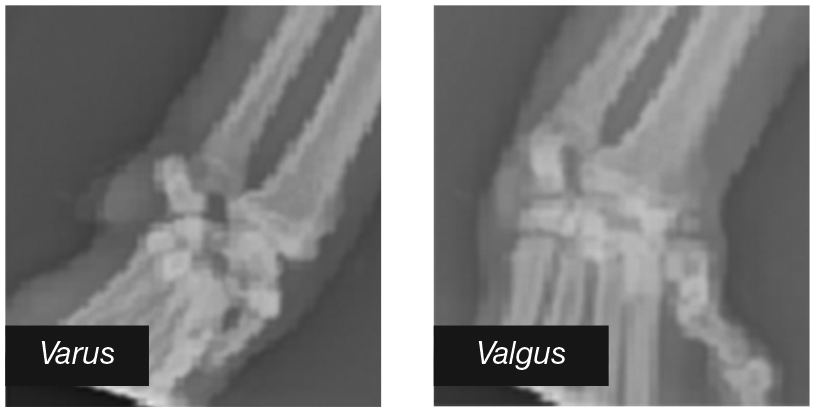
Varus and valgus stressed radiographs from a cat with antebrachiocarpal joint subluxation. On the varus stress radiograph there is displacement of the radial carpal bone in a palmaromedial direction, and overriding of the middle carpal and antebrachiocarpal joints with poor definition of the carpal bones
The treatment for antebrachiocarpal joint luxation initially requires repair or reconstruction of the short radial collateral ligament. If the ligament ends are intact, primary repair should be performed. In a report by Shales and Langley-Hobbs, horizontal mattress sutures with 3-0 polypropylene were used. 11 Where primary repair is not possible, ligament reconstruction can be performed. Voss et al have described the use of bone screws as suture anchors and 2-0 polypropylene suture. 4 A dorsomedial approach is made to the carpus and a 1.5 mm screw is inserted proximally in the radial metaphysis in a dorsomedial to palmarolateral direction. The second 1.5 mm screw is inserted palmar to the tendon of the extensor pollicis longus, placed centrally within the radial carpal bone and directed slightly dorsally. The ligament prosthesis is secured around the screws in a figure-of-eight fashion, taking care to avoid over-tightening, as this could restrict carpal joint motion and result in premature failure of the prosthesis.
If there is a tear in the joint capsule, the preference of the authors is to place simple interrupted absorbable sutures for closure. In the presence of radioulnar ligament instability following ligament reconstruction, a temporary screw or pin can be inserted lateromedially through the ulnar styloid process into the distal radius to allow the radioulnar ligament to heal (a 0.9 mm trocar-tipped K-wire has previously been used for this purpose).11,29 This should be removed after 4–6 weeks due to the restriction of supination and risk of wire breakage. 11
Ligament healing is typically slow, so the repair should be supported with either external coaptation, including a splint, or external skeletal fixation. A craniomedial type 1a external skeletal fixator can be used, and in previous reports has been maintained for 5 weeks prior to removal.11,13
Middle carpal and carpometacarpal joints
Luxation of the middle carpal and carpometacarpal joints is usually associated with hyperextension injury, and rarely diagnosed in isolation. Where there is middle carpal joint subluxation, there may be a gap between the palmar process of the ulnar carpal bone and metacarpal V, or widening in the joint space between the radial carpal bone and carpal bone II, indicating damage to the intercarpal ligaments. 4 With carpometacarpal joint luxation or subluxation, the base of the metacarpal bones may appear to overlap the carpal bones. 29
The technique for surgical reconstruction of the intercarpal ligament between the radial carpal bone and carpal bone II in the dog has been described by DeCamp et al. 30 However, the current authors’ impression is that this would be difficult in the cat owing to the small size of the numbered carpal bones, leading to a high risk of iatrogenic fracture. Where there is no disruption of the palmar ligaments, closed reduction with external coaptation for 6 weeks could be attempted.
Carpal bone fracture and luxation
Radial carpal bone
To the authors’ knowledge, isolated fracture of the radial carpal bone has not been reported in the cat. In the dog, there are case series that describe the injury being associated with repetitive strain or inherent weakness in the bone. The latter is postulated to be associated with incomplete ossification of the radial carpal bone. 23 There is a single report, by Pitcher, 13 of radial carpal bone luxation in the cat, in which there was displacement in a palmaroproximal direction.
The reported treatment for feline radial carpal bone luxation is open reduction and fixation of the radial and ulnar carpal bones with a K-wire or lag screw, primary repair or reconstruction of the short radial collateral ligament, and repair of the joint capsule, with or without transarticular external skeletal fixation.13,32 In order to achieve reduction of the radial carpal bone, Pitcher described flexion with distraction of the antebrachiocarpal joint, and rotation of the radial carpal bone 90° along the dorsopalmar axis followed by the mediolateral axis. 13 A dorsal (± combined pal-maromedial) approach can be used to access the radial carpal bone and insert either a lag screw (1.3 or 1.5 mm cortical screw) or K-wire (1 mm diameter or less) slightly obliquely in a dorsolateral direction until the ulnar carpal bone is engaged. During implant insertion, bone holding forceps should be used on the abaxial surfaces of the radial and ulnar carpal bones to prevent lateral displacement of the ulnar carpal bone. Repair of the short radial collateral ligament should be completed as described earlier.
Complications following internal fixation of the radial and ulnar carpal bones include residual instability of the radial carpal bone and irritation caused by the stabilising K-wire. 29
The reported treatments for radial carpal bone fracture in the dog include insertion of a lag screw from the palmaromedial aspect of the radial carpal bone for a simple fracture; in the case of a dorsal slab fracture, two lag screws are placed in the dorsopalmar direction, albeit isolated radial carpal bone fracture has not been described in this species. 30 The small size of the radial carpal bone may preclude the use of these techniques in the cat. 30
Postoperatively, the repair should be supported with external skeletal fixation or a cast for 4–6 weeks. 30 In the case described by Pitcher, there was a good outcome following placement of a K-wire and transarticular external skeletal fixation; however, osteo-arthritis developed in the long term. 13
Accessory carpal bone
Accessory carpal bone injury is rare in cats. There are two single reports to date: one was a cat with accessory carpal bone luxation 4 and the second a cat with concurrent dorsomedial antebrachiocarpal luxation. 11 In dogs, there are five recognised types of accessory carpal bone fracture, but the same classification system does not appear to be relevant in the cat. 33 Montavon et al refer to having managed accessory carpal bone fractures in two cats (one was distal basilar and the second, comminuted); 29 however, the outcome for these cases was not described.
In the case of accessory carpal bone fracture in the cat, treatment involves external coaptation with the carpus immobilised in 20° flexion for 4–6 weeks. 29 If this is not successful and the lameness persists, then fragment removal or arthrodesis can be considered. Harris et al reported a cat with accessory carpal bone subluxation due to damage to the accessorioulnocarpal ligament. 2 In this case, widening of the accessorioulnar joint space was evident on the radiographs. The reported treatment was accessorioulnar arthrodesis, with the accessory carpal bone being fixed to the ulnar carpal bone with a 0.6 mm K-wire following removal of articular cartilage and placement of an autogenous cancellous bone graft. A palmarolateral approach is described for this technique, with insertion of the K-wire from the apical surface of the accessory carpal bone. 2 Postoperative stabilisation involved splinting of the carpus in a semi-flexed position for 4 weeks. The reported outcome for this case was good, with the cat having no lameness at follow-up at 17 months. 2
Ulnar carpal bone and numbered carpal bones
These injuries are rare in the cat and usually occur in conjunction with hyperextension or antebrachiocarpal luxation (see Figure 11 for radiographic appearance of ulnar carpal bone luxation). The authors are not aware of any reports of ulnar or numbered carpal bone fracture in the cat.

Dorsopalmar (a) and mediolateral (b) radiographs of a cat with ulnar carpal bone luxation and palmar carpometacarpal subluxation. On the dorsopalmar view there is increased joint space between the ulnar carpal bone and radial carpal bone, and the ulnar carpal bone and radius, suggestive of ulnar carpal bone luxation. The arrow on the dorsopalmar view is pointing to the sesamoid within the tendon of the abductor pollicis longus muscle, which is commonly mistaken for a fracture of the radial styloid
In the case of ulnar carpal bone luxation, the authors recommend open reduction and fixation to the radial carpal bone with a K-wire (as described above for radial carpal bone luxation). Where there is concurrent injury to the palmar ligaments, pancarpal arthrodesis (± K-wire fixation) is more appropriate. The short ulnar collateral ligament should also be inspected and treated with a primary repair or ligament reconstruction if required.
The small size of the numbered carpal bones limits the capacity for implant placement, and the authors recommend following what is currently described for the dog by DeCamp et al. 30 The bones of the larger proximal carpal row are shown in Figure 12. Small non-displaced fragments may reattach after 4 weeks of splinting the carpus. 30

Photographic image of anatomical specimens, illustrating the relative size of the carpal bones of the proximal carpal row. Note that the accessory carpal bone is slightly obliquely positioned compared with the ‘skyline’ views of the other bones
Damage to the palmar ligaments and fibrocartilage (hyperextension injury)
The middle carpal and carpometacarpal joints are more commonly affected by hyperextension injury than the antebrachiocarpal joint. Patients with hyperextension injury are typically presented with a palmigrade stance and carpal extension of at least 20–30° (normal extension is 15° in the cat).14,30 Where there is injury of the palmar ligaments at the level of the carpometacarpal joint, there will be dorsal deviation of the metacarpal bones relative to the distal carpal bones on flexed stressed radiographs.
Although external coaptation of the carpus in flexion has been described as a treatment option for these injuries, the clinical results are often disappointing owing to a continued palmigrade stance.3,33 Greeff et al reported management of carpal hyperextension and dorsal luxation of the second carpal bone with a temporary modified type IIb external skeletal fixator with insertion of K-wires across the metacarpophalangeal joints. 14 This was achieved using two 2 mm centrally threaded full pins and a negatively threaded half pin in the radius, with 1.1 mm K-wires inserted in a normograde direction and directed proximally in the distal epiphyses of metacarpal bones II, III and IV, extending to the proximal extent of the radial carpal bone. These pins and wires were then incorporated into a Kirschner–Ehmer construct that was removed after 6 weeks. This cat was not lame at 1-year follow-up. This option may be suitable in cases without concurrent carpal bone fracture or collateral ligament instability.
Where this is no obvious involvement of the antebrachiocarpal joint, partial carpal arthrodesis can be performed and is thought to be advantageous due to preservation of range of motion at the antebrachiocarpal joint. 29 In dogs, the reported disadvantage of partial carpal arthrodesis is residual hyper-extension and osteoarthritis of the ante-brachiocarpal joint, resulting in ongoing lameness. As yet, there are no long-term studies to assess these complications in the cat. 14 Unlike the dog, dorsally applied bone plates are not recommended in the cat due to the potential for implant interference with carpal joint flexion. 29 The reported techniques for partial carpal arthrodesis in the cat include cross pinning and medial plating.15,16
Cross pinning was described in two cats by Haburjak et al. 15 A dorsal approach was used first to access the middle and carpometacarpal joints to allow for removal of articular cartilage and placement of autogenous cancellous bone graft. Two K-wires one-third the proximal diameter of metacarpal II were chosen; the first wire engaged the proximal aspect of metacarpal II and was directed dorsolaterally to engage the ulnar carpal bone. The second wire was inserted from the proximomedial aspect of the radial carpal bone in a palmaro-lateral direction to exit in the proximal third of metacarpal V. In one of the cats, there was pin migration at short-term follow-up; however, there was no longer term follow-up in these cases. The most common surgical error was failure to engage the radial and ulnar carpal bones with the wires. The current authors do not recommend using this technique because of the lack of interfragmentary compression and likely failure to achieve bone fusion.
The plates available for performing a partial carpal arthrodesis in the cat include a 1.5 mm Veterinary Cuttable Plate (Synthes), Stryker 1.7 mm titanium hook plate (with the hook removed) and Synthes 1.3 mm finger-plate. 16 In other small implant systems the screw hole spacing is too wide to engage the appropriate number of carpal bones (ideally a minimum of two screws in the carpal bones).
Mathis and Voss described the use of medially applied mini-plates in three cats. 16 The first screw was inserted into the radial carpal bone, with the second screw being placed in the base of the metacarpal bones. Burring of articular cartilage was reportedly difficult using the medial approach in these cases, with the fifth carpometacarpal joint being inaccessible. This resulted in a tendency for only the medial aspect of the carpometacarpal joint to fuse. At 1-year follow-up, clients in this study reported that their cats showed decreased ability to jump and decreased climbing, which the current authors speculate may be due to incomplete fusion of the joint rather than true arthrodesis. Figure 13 shows postoperative radiographs from a cat in which partial carpal arthrodesis was performed using a medially applied plate.

Dorspalmar (a) and mediolateral (b) radiographs following a partial carpal arthrodesis in a cat using a 1.5 mm cuttable plate. Images courtesy of the University of Sydney Veterinary Teaching Hospital
Pancarpal arthrodesis
When to consider
The published indications for pancarpal arthrodesis include carpal hyperextension, end-stage osteoarthritis, intra-articular fractures, severe shearing injuries and some peripheral nerve injuries. 30 Pancarpal arthrodesis may be considered when there is carpal hyperextension combined with multiple carpal bone fractures or instability of the antebrachiocarpal joint, and in cats showing continued lameness despite primary ligament repair and joint stabilisation.
Surgical technique
Bone graft harvest should be considered and included as part of the surgical preparation prior to arthrodesis surgery. The authors’ preference for bone graft collection is to have the patient positioned in dorsal recumbency with a hanging leg preparation, and the proximal humerus included in the surgical field. A 2 cm sharp incision is made craniolateral to the greater tubercle of the humerus until the underlying bone is palpated, and Gelpi retractors are inserted. The brachiocephalicus muscle and acromial part of the deltoideus muscle are separated with this approach. 28 A 1.5–2 mm drill bit can be used to create a monocortical hole and cancellous bone is collected using a curette. In older cats where bone graft collection may be low yield, the iliac crest of the ipsi-lateral side can additionally be prepared. Bone graft substitutes such as demineralised bone matrix are also commercially available.
A dorsal or medial approach can be used for pancarpal arthrodesis, as described above, depending on the site of plate application. Once the approach is made, the joint capsule of all transverse joints of the carpus should be incised using a size 15 blade and the articular cartilage removed using a high-speed pneumatic burr, with an assistant providing gentle lavage and flexion of the carpus. Care is needed with the burr not to destroy small carpal bones, and, for this reason, using a curette may be advisable.
The reported techniques for pancarpal arthrodesis in the cat include dorsal or medial plating.17–19 The recommended implant systems for plating feline carpi include the Hybrid Pancarpal Arthrodesis Plate 1.5/2.0 mm (Veterinary Instrumentation), Veterinary Cuttable Plates 1.5/2.0 mm (Synthes), dynamic compression plates 1.5/2.0 mm (Synthes), Castless Plate 1.5/2.0 mm (Orthomed, UK), the Compact 2.0 maxillofacial LOCK system (Synthes) and the Fixin six-hole V2102 plate (Figure 15).


Pancarpal arthrodesis in a cat using a dorsal approach. This intraoperative image shows preparation of joint spaces for removal of articular cartilage. RCB = radial carpal bone; CII = carpal bone II
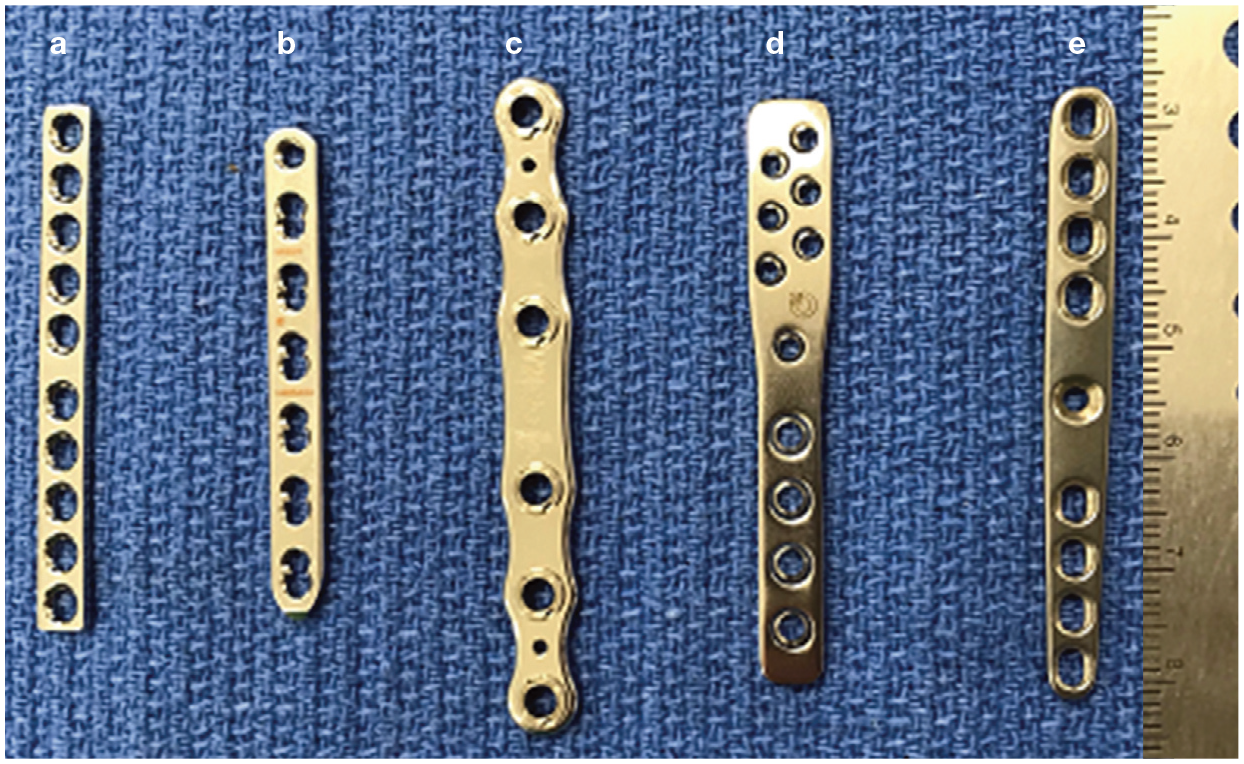
Some of the commercially available plates that can be used to perform a pancarpal arthrodesis. (a) 1.5/2.0 mm 10-hole Synthes dynamic compression plate; (b) 1.5/2.0 mm seven-hole Synthes locking compression plate; (c) Fixin six-hole V2102 plate; (d) Castless Plate 1.5/2.0 mm (Orthomed, UK); (e) Hybrid Pancarpal Arthrodesis Plate 1.5/2.0 mm (Veterinary Instrumentation)
Dorsal plating
When performing dorsal plating, the plate is not applied on the tension side of the bone, which may explain the augmentation of the repair with casting, transarticular external skeletal fixation or crossed pins in the study by Calvo et al. 17 Simpson and Goldsmid were the first to describe a case of feline pancarpal arthrodesis using a dorsally applied eight-hole 1.5 mm mini-plate. 18 They measured the width of the metacarpal bones in 15 cadavers and concluded that no greater than a 1.5 mm diameter screw should be placed in metacarpus III, to avoid iatrogenic fracture.
The plates that are commonly applied dorsally include the Hybrid Pancarpal Arthrodesis Plate 1.5/2.0 mm and, more recently, the Castless Plate 1.5/2.0 mm. The benefit of these plates is that the screw hole sizes are larger for the radial metaphysis (2.0 mm: proximally) than they are for the radial carpal and metacarpal bones (1.5 mm: distally). The Castless Plate was developed to allow for screw placement in metacarpals III and IV, though there are currently no studies to show that it is biomechanically superior to the Hybrid Pancarpal Arthrodesis Plate. In the only study to describe the use of a Castless Plate in cats, all three cats had reported complications including bone resorption under the plate (one cat) and paw swelling (two cats). 34
The authors’ preference with respect to a dorsal pancarpal arthrodesis is to use a Hybrid 1.5/2.0 mm plate due to the ease of approach and application (Figure 16). Preoperative planning is described in Figure 17.

Postoperative dorsopalmar (a) and mediolateral (b) radiographs of a feline carpus following pancarpal arthrodesis using a 1.5/2.0 mm Hybrid Pancarpal Arthrodesis Plate

Preoperative planning for a dorsal pancarpal arthrodesis. (a) A screw is inserted in the radial carpal bone, and the screw length is measured. The red marker corresponds to the location of the radial carpal bone. (b) The diameter of metacarpal III is measured (red line) to ensure that an appropriate screw size is selected. (c) The plate is pre-contoured prior to surgery. The red line corresponds to the angle at which the plate is contoured. (d) Metacarpal III (red line) is measured to ensure that the plate will span at least 50% of its length
Medial plating
The purported benefits of medial plating are an increased area moment of inertia of the plate and the fact that the screws can engage multiple metacarpal bones.16,19 The technique has been described in three cats by Streubel et al using a Compact 2.0 mm locking plate. 19 Although two cats had complete radiocarpal joint fusion at follow-up, in one cat there was incomplete fusion of the radiocarpal joint and plate breakage at 4.5-year follow-up. This was thought to be due to lack of compression at the radiocarpal joint caused by the use of locking screws and a resulting gap within the joint space.
Ulnocarpal arthrodesis
Ulnocarpal arthrodesis has been described in a single case report to treat atrophic non-union of the distal third of the radius and concurrent carpal bone luxation. At long-term follow-up there was resolution of lameness. 20 The authors of that report used closed reduction with a bilateral uniplanar external skeletal fixator to achieve arthrodesis. 20 In this particular case there was osteolysis of the distal 20% of the radius that prevented incorporation of the distal radius within the arthrodesis.
Postoperative care
Follow-up radiographs should be obtained every 6 weeks until osseous fusion is complete (ie, when the full width of all joint spaces is bridged by bone in both mediolateral and dorsopalmar projections). 36 While it has not been studied in the cat, a previous study in eight dogs described healing following dorsal pancarpal arthrodesis and the use of autogenous cancellous bone graft. 37 Delayed or failed fusion of the arthrodesis may be due to failure to completely remove all articular cartilage. 37 The use of external coaptation with a modified Robert Jones bandage and palmar splint is recommended for 4 weeks, and application of a modified Robert Jones bandage without support for an additional 4 weeks.
Complications and long-term outcome
The reported complications following pancarpal arthrodesis in both the dog and cat include failure of bone fusion (Figure 18), metacarpal bone fracture, pin loosening, infection and multiple screw loosening. Calvo et al assessed long-term functional outcome in 20 cats treated with pancarpal arthrodesis. 17 According to an owner questionnaire (11 cats), a large proportion of those cats showed a reduced height of jump (10/11) and a general unwillingness to jump and climb. 17 There was a 35% complication rate; however, the only major complication requiring further surgery noted in this study was multiple screw loosening that led to plate and screw removal.

Dorsopalmar radiographs of a feline carpus. (a) Image taken immediately postoperatively following placement of a 2.7 mm dynamic compression plate for pancarpal arthrodesis with no bone graft. Note that this plate size is larger than would be recommended for pancarpal arthrodesis. (b) The same carpus 6 months postoperatively following plate removal due to the formation of a draining sinus over the plate. There is failure of arthrodesis due to inadequate fixation and infection
It has also been speculated that pancarpal arthrodesis reduces supination and pronation of the feline antebrachium, although the extent to which this occurs is unknown. 16
Key Points
Some carpal injuries in cats are amenable to treatment with open reduction, primary ligamentous repair and external support using either a cast or external skeletal fixation.
The authors believe that ligamentous injury is common enough to warrant routine use of stress radiography where there is a known traumatic carpal injury, and that primary repair with rigid fixation will provide a more favourable outcome than using pancarpal arthrodesis as a first-line treatment.
Pancarpal arthrodesis should remain a salvage procedure, reserved for select cases and those with ongoing pain and lameness.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.