
Abstract
Objectives
The aim of this study was to define the clinical characteristics of cats referred for evaluation of subclinical cardiac murmurs, and, secondarily, to identify predictors of echocardiographic identification of cardiac disease.
Methods
One hundred and sixty-three apparently healthy cats with subclinical murmurs were retrospectively enrolled. Medical records of cats older than 1 year of age referred for the evaluation of subclinical murmurs were reviewed. Cats were considered healthy if clinical signs of systemic disease or cardiac disease were not reported and cats were not receiving cardiac medications. Logistic regression was used to identify clinical variables that predict echocardiographic identification of cardiac disease.
Results
One hundred and eight cats (66.3%) had echocardiographic evidence of cardiac disease with hypertrophic cardiomyopathy being the most common (80.5%). Left atrial enlargement was uncommon; in 90% of cats with echocardiographically identified cardiac disease, the left atrial aortic ratio from two-dimensional echocardiography was <1.51. Cats with cardiac disease were more likely to be male (P = 0.016), weigh more (P <0.01) and have a murmur of intensity ⩾3/6 (P = 0.019) than cats without cardiac disease. Murmur intensity ⩾grade 3/6 (P = 0.01) and male sex (P = 0.01) were independent predictors of echocardiographic evidence of cardiac disease in multivariable analysis.
Conclusions and relevance
The majority of cats referred for evaluation of subclinical cardiac murmurs have cardiac disease. Based on left atrial dimensions, cardiac disease is generally mild. Male sex and a loud cardiac murmur are associated with the identification of cardiac disease.
Introduction
Heart murmurs are often identified during the examination of apparently healthy cats; the reported prevalence of subclinical murmurs is between 15.5% and 34%.1,2 However, the finding of a cardiac murmur is inconsistently related to the presence of cardiac disease. Cardiac disease is absent in as many as 50% of cats that have cardiac murmurs.1,2 In some feline patients that are free of primary cardiac disease, dynamic right ventricular outflow tract obstruction is apparently responsible for murmurs, but murmurs also develop in the absence of echocardiographically identified flow disturbances.1–4 When cardiac disease is associated with the presence of a murmur, hypertrophic cardiomyopathy (HCM) is most commonly identified.1,2,4 The diagnostic accuracy of B-type natriuretic peptide has been evaluated in feline patients with clinically occult cardiac disease, and when the result of a quantitative BNP assay is within the reference interval, the probability that severe cardiac disease is present is likely to be low. 5 However, echocardiography is required to determine conclusively the cause and the clinical importance of feline murmurs.
Most feline patients that have incidentally detected cardiac murmurs in which cardiac disease is echocardiographically evident have HCM. While the clinical course of feline HCM is often benign, some patients have a poor outcome related to the development of congestive heart failure, the occurrence of arterial thromboembolism or sudden unexpected death. 6 Echocardiographic left atrial enlargement (LAE) has consistently been associated with poor outcome in feline cardiomyopathies.7–10 The prevalence of heart disease in feline patients referred for evaluation of subclinical murmurs has been estimated, but the severity of disease in this population has been incompletely defined. 4
Through retrospective evaluation of case records, we sought to define the clinical characteristics of feline patients referred for evaluation of subclinical cardiac murmurs, with attention to the prevalence of atrial enlargement. Secondarily, the study was designed to identify patient characteristics that might predict echocardiographic detection of cardiac disease.
Materials and methods
We searched the archive of Virginia Maryland College of Veterinary Medicine for medical records of apparently healthy cats, referred between 1 September 2006 and 31 August 2016, for evaluation of cardiac murmurs. Medical record data of apparently healthy cats with murmurs were included in analyses if patient age was >1 year, and if both physical and echocardiographic findings, including an assessment of left atrial size, were recorded and available for review. Cats were considered to be ‘apparently healthy’ if a review of the patient history failed to disclose clinical signs of disease, evidence of chronic diseases such as hyperthyroidism, diabetes, previously identified systemic hypertension or renal insufficiency was absent and patients were not receiving cardiac medications. Cats with previous diagnoses of congenital or acquired cardiac disease were excluded.
Signalment and patient history were recorded, and all cats underwent physical examination, which included thoracic auscultation. Auscultatory characteristics, including murmur intensity, the murmur’s point of maximum intensity, and presence or absence of gallop sounds were recorded in the medical record. In some cases, the intensity of murmurs was variable; the greatest recorded intensity was subject to analysis.
Echocardiography was performed using commercially available ultrasound instruments (Vivid 7 [GE-Medical and Artida: Toshiba Medical Systems]), while patients were manually restrained in right, and then left, lateral recumbency. To facilitate echocardiographic examination, sedative agents (butorphanol and/or acepromazine) were administered to some patients. Standard echocardiographic methods were used to obtain M-mode, two-dimensional and Doppler echocardiographic images. M-mode echocardiographic examination of the left ventricle was guided by two-dimensional echocardiographic short-axis images. The following ventricular dimensions were obtained from M-mode images: end-diastolic thickness of the interventricular septum; end-diastolic thickness of the left ventricular posterior wall; end-systolic thickness of the interventricular septum; end-systolic thickness of the left ventricular posterior wall; end-diastolic left ventricular chamber dimension; and end-systolic left ventricular chamber dimension. Left ventricular fractional shortening was derived. In most cases, measurements of interventricular septal thickness and left ventricular posterior wall thickness also were obtained from the two-dimensional right parasternal long-axis view. Left atrial dimensions and aortic diameters were obtained from a two-dimensional right parasternal short-axis view at the level of the heart base. M-mode images of the aorta and left atrium were guided by right parasternal short-axis images. The left atrial dimension indexed to aortic diameter (obtained from M-mode [LA:AoM] or two-dimensional echocardiography [LA:Ao2D]) was calculated.11,12 Color Doppler mapping was used to identify flow disturbances. Transvalvular velocities were recorded from spectra obtained by pulsed- or continuous-wave Doppler interrogation.
Left ventricular hypertrophy (LVH) was defined, from stored M-mode and two-dimensional images, by an end-diastolic wall thickness ⩾6 mm in any region of the interventricular septum or of the left ventricular free wall. 13 LAE was defined by LA/AoM >1.54 or LA:Ao2D >1.39. 11 Dynamic right ventricular outflow tract obstruction was defined by the presence of a systolic jet that originated proximal to the pulmonary valve with a spectral Doppler echocardiographic characteristics that indicated late systolic acceleration. Similarly, dynamic left ventricular tract obstruction was defined by late systolic acceleration. An electrocardiogram was recorded during echocardiography if the patient tolerated placement of electrodes.
Numerical data that were subject to analysis were abstracted from the medical record. Images were reviewed only to verify extreme observations that might represent data entry errors or to clarify apparent discrepancies between textual descriptions and numerical data. Additional diagnostic investigations, including thoracic radiography, determination of systemic arterial blood pressure and evaluation of thyroid function, were at the discretion of the attending clinician.
Statistical analysis
Statistical analysis was performed using commercially available computer software (JMP Pro 14; SAS Institute). Continuous variables were compared using the Student’s t-test or Mann–Whitney U-test, as appropriate, based on data distribution. Associations between categorical variables were evaluated using Fisher’s exact test. A multivariable logistic regression model was developed to identify characteristics evident prior to referral that might independently predict echocardiographic identification of structural cardiac disease. The response variable was presence/absence of cardiac disease. Candidate variables, specifically sex, age and detection of a cardiac murmur with intensity of grade 3/6 or greater, were selected based on published literature, biologic plausibility and inspection of scatterplots and 2 × 2 tables. Body weight was not included because its effect is confounded by sex; male cats weighed more than female cats. A backward stepwise procedure for variable selection was used. Normally distributed data are presented as mean ± SD, while data that were not normally distributed are presented as median (range) or, to emphasize specific features of the data, median (interquartile range [IQR]). Categorical variables are presented as counts and percentages. The distribution of the data or residuals was graphically evaluated to ensure that the assumptions of all statistical tests were met. Alpha was set to a value of 0.05.
Results
Between 1 September 2006 and 31 October 2016, 684 cats were referred to the Cardiology Service of the Virginia Maryland College of Veterinary Medicine, and 163 cats met the inclusion criteria. Of these 163 cats, most, 143 (87.7%), were mixed breed, classified as domestic shorthair or domestic longhair, but a few purebred lines were represented. There were four Maine Coon cats, four Siamese cats and other breeds were represented by three or fewer individuals.
Of the 163 cats, 102 (62.6%) were male and 61 were female. Body weight was significantly greater in male cats than in female cats (median 5.3 kg [range 2.8–9.3 kg] vs 4.2 kg [range 1.5–6.9 kg]; P <0.01). Mean heart rate recorded during physical examination was 192 ± 25 beats per min. For 157 (96.3%) patients, the maximum recorded heart murmur intensity was graded 2–4/6 (Figure 1). The modal value of murmur intensity was grade 3/6, with 87 (53.4%) patients having a murmur of this intensity. Murmur intensity varied during the examination in 42 (25.8%) cats. In 95% of the patients, the point of maximal intensity of the murmur was described as some variation of sternal border (n = 11), left parasternal (n = 102) or right parasternal (n = 43). All murmurs, except for two, were systolic; the two exceptions were ‘to-and-fro’ murmurs associated with congenital heart disease. A gallop sound was recorded in 21 (12.9%) cats and in eight of these (4.9%) the gallop was intermittent.

Distribution of maximal recorded murmur intensity from 163 apparently healthy cats referred for echocardiographic evaluation of cardiac murmurs
Twenty-five (15.3%) cats were sedated, with butorphanol and/or acepromazine, prior to echocardiographic examination.
Cardiac disease was echocardiographically identified in 108 (66.3%) of the 163 cats. Of these 108 cats, 87 (80.5%) had HCM, nine (8.3%) had left ventricular hypertrophy (LVH) attributed to hyperthyroidism or systemic hypertension, eight (7.4%) had congenital heart disease and four (3.7%) had mitral regurgitation (MR) of undetermined cause. Of the cats with congenital heart disease, three had a ventricular septal defect, two had valvular aortic stenosis and the remaining three had subaortic stenosis, mitral valve dysplasia and tricuspid valve dysplasia, respectively. Cats with MR of undetermined cause were reported to have MR but not reported to have LVH or systolic anterior motion of the mitral valve. Cats with a HCM phenotype, classified either as HCM or LVH (HCM-P), constituted 88.9% of those with cardiac disease, and 58.9% of the entire study sample. 14
In the 96 cats that had HCM-P, 82 (85.4%) murmurs were associated with the findings of dynamic left ventricular outflow tract obstruction, dynamic right ventricular outflow tract obstruction, or concurrent left and right ventricular outflow tract obstruction (Figure 2). For the remaining 14 (14.6%), the putative cause of the murmur was not echocardiographically identified or was not recorded in the medical record. Of 55 cats in which echocardiography did not disclose cardiac disease, the following flow disturbances were identified: dynamic left ventricular outflow tract obstruction, dynamic right ventricular outflow tract obstruction, or concurrent left and right ventricular outflow tract obstruction in 30 (54.5%). In the remainder, the murmurs were believed to be innocent.
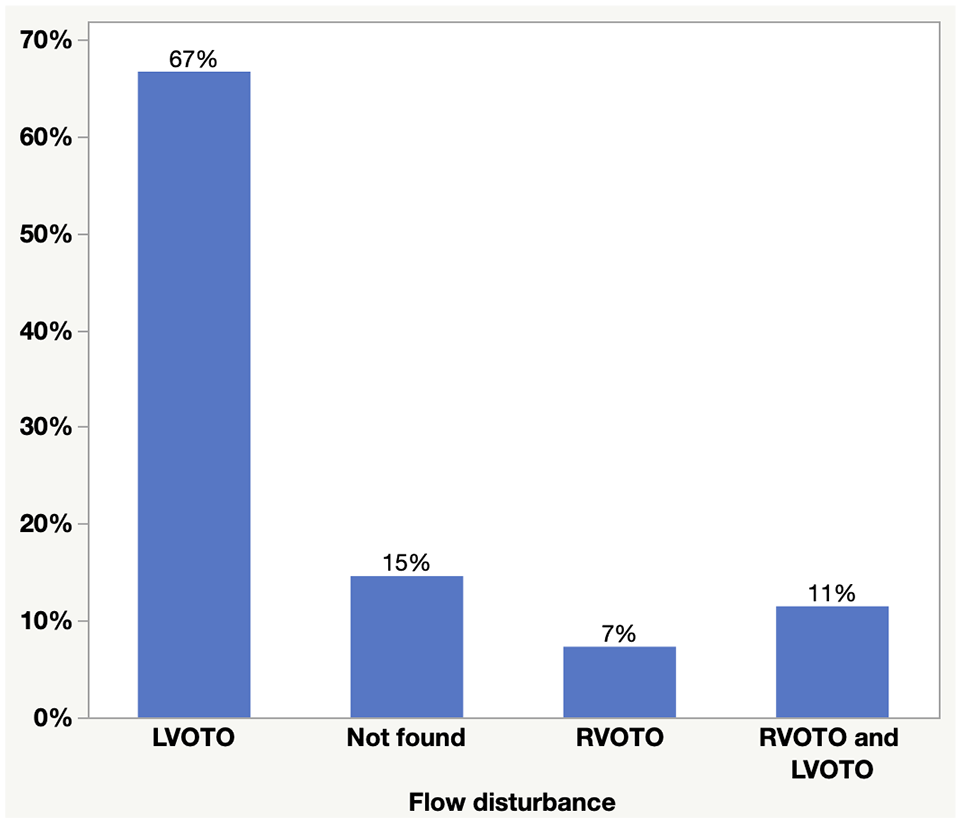
Distribution of flow disturbances inferred from Doppler echocardiographic findings in 96 cats with left ventricular hypertrophy phenotype that had been referred for evaluation of subclinical cardiac murmurs.
LAE was identified in 41/163 (25.1%) patients, two of which had congenital heart disease. Three cases that were classified free of cardiac disease based on the textual description provided by the attending clinician had LA:Ao2D that were >1.4 but <1.5, and one classified as free of disease had an LA:AoM that was 1.55. The median LA:AoM in the 108 cats in which cardiac disease was echocardiographically identified was 1.4 (IQR 1.28–1.55), while the median for LA:Ao2D was 1.3 (IQR 1.2–1.43). When LAE was identified, it generally was mild. The 90th percentiles of LA:AoM and LA:Ao2D were, respectively, 1.63 (n = 111) and 1.51 (n = 148) (Figure 3).

Box plots of ratios of left atrial dimension and aortic diameter obtained from M-mode (LA:AoM; n = 71) and two-dimensional echocardiography (LA:Ao2D; n = 100) of 108 cats with subclinical cardiac murmurs in which cardiac disease was echocardiographically identified. Both LA:AoM and LA:Ao2D were available for most cases, but, for a few, only one of the ratios was recorded. Each box represents the interquartile range (IQR) and is divided by a line that represents the median value. ‘Whiskers’ represent the value that is most distant from the median but within 1.5 times the IQR from the first or second quartiles. Dots represent single observations greater than or less than the value defined by the ‘whiskers’
The clinical characteristics of cats with and without echocardiographically identified cardiac disease are presented in Table 1. Statistically significant differences between ages of cats that did or did not have cardiac were not identified. Those with cardiac disease were more likely to be male, heavier and more apt to have murmurs graded ⩾3/6 than those without. Neither identification of a gallop sound nor a murmur of consistent intensity were significantly associated with the presence of structural cardiac disease. Statistically significant differences were not identified when the age (P = 0.73) and body weights (P = 0.47) of patients with cardiac disease and LAE were compared with those of patients with cardiac disease that lacked LAE. Male sex (P = 0.83), murmurs of ⩾3/6 intensity (P = 0.42) and detection of a gallop sound (P = 0.06) were not associated with LAE in patients with cardiac disease.
Characteristics of 163 cats with subclinical cardiac murmurs in which cardiac disease was, or was not, echocardiographically identified

Data are presented as n (%), median (range) or mean ± SD, as appropriate, based on the type of variable and distribution. Variables for which there were missing observations are identified through presentation of specific values for n. P values are from comparisons of cats with cardiac disease to cats without
n = 102
n = 51
n = 91
n = 49
bpm = beats per min
Candidate explanatory variables for a logistic regression in which the response variable was presence/absence of echocardiographically identified cardiac disease were age, sex and murmur intensity of ⩾grade 3/6. Multivariable logistic regression identified murmur intensity ⩾grade 3/6 (odds ratio [OR] 2.6, 95% confidence interval [CI] 1.209–5.579; P = 0.01) and male sex (OR 2.46, 95% CI 1.24–4.87; P = 0.01) as independent predictors of the presence of cardiac disease. The odds of a diagnosis of cardiac disease can be expressed in terms of probabilities (Table 2).
Probabilities of echocardiographic diagnosis of cardiac disease in 163 cats with subclinical cardiac murmurs, of which 108 were determined to have cardiac disease

Estimated probability is from a logistic model in which there were significant effects of the identification of a murmur with intensity ⩾grade 3/6 (P = 0.01) and of male sex (P = 0.01)
M = male; F = female
Discussion
We reviewed the medical records of apparently healthy cats that were referred for evaluation of cardiac murmurs. Most of these cats had echocardiographic evidence of cardiac disease, and the majority of patients in which cardiac disease was identified had HCM-P. LAE is uncommon in feline patients with incidentally detected cardiac murmurs, and, when identified, LAE generally was mild. Cats with LAE did not differ from cats without LAE with regard to sex, body weight, age or murmur intensity. Of cats referred for evaluation of subclinical cardiac murmurs, male sex and murmurs of intensity ⩾grade 3/6 independently predict the echocardiographic identification of cardiac disease.
The proportion of cats that had echocardiographically identified HCM-P, 58.9%, is similar to that in the investigation that most closely matches our own with respect to study population but greater than might be predicted based on studies of relatively unselected samples of cats. In a prospective evaluation of referred cats with subclinical murmurs, 17/32 had echocardiographically identified cardiac disease. 4 However, in community-based echocardiographic surveys, 5/16 (31.3%) and 94/318 (29.6%) apparently healthy cats with murmurs had HCM-P.1,2 These disparities might be explained by the characteristics of the referral population. The patients that we report were older and, in general, had louder murmurs than those described in ‘CATSCAN’, the most extensive echocardiographic evaluation of apparently healthy cats. 2 HCM is not exclusively a geriatric disease, and retrospective evaluations of referred cases reveal a mean or median age at diagnosis that generally is close to 6 years.7,8,15 However, in apparently healthy cats, the proportions of older cats that have murmurs and have HCM is greater than the proportions observed in younger cats.2,6 The study that yielded those data was not longitudinal, so the age-dependent incidence of HCM is not known; however, it is likely that cats of any age can be affected, but lengthy survival of cats with subclinical disease together with geriatric development of disease account for the high proportions of older, affected cats in cross-sectional studies. Regardless, the median age of the cats that we studied was 7 years, similar to that reported by Nakamura et al, 4 while the median age of cats enrolled in CATSCAN was within the range of 1–3 years and 70% were younger than 5 years of age. 2 The cats that we studied generally had louder murmurs than those in CATSCAN. In that study, of the 318 cats that had murmurs, the modal grade was 2/6 and 67.3% had grade 1/6 or grade 2/6 murmurs. 2 In contrast, the modal intensity in our population was grade 3/6. While intensity of murmurs in patients with feline cardiomyopathy is inconsistently related to severity of disease, it is possible – perhaps likely – that patients with louder murmurs are more apt to be referred. 16 The proportion of cats that had murmurs for which intensity varied (26%) was similar to one study of apparently healthy cats but considerably lower than that identified during CATSCAN, in which 91.2% of cats with murmurs were reported to have variable intensity.1,2,17 However, our data consist of medical records that describe a single hospital visit. In contrast, auscultation was performed multiple times by different operators during CATSCAN.
LAE was detected in a minority of our cases (25.2%), but this proportion is greater than previously published estimates of the prevalence of LAE. One of 17 (5.9%) referred cats with subclinical murmurs were reported to have LAE, and, in relatively unselected populations, the prevalence of LAE was 0 or 0.08%.1,2,4 In CATSCAN, the prevalence of LAE in cats with HCM was 3.5%. 2 Partly, the greater prevalence is explained by the use of 1.39 and 1.54 as upper limits of, respectively, the reference intervals (RIs) for LA:Ao2D and LA:AoM. These limits are relatively conservative but based on published literature. 11 Others, citing a textbook, or publications that relate to canine or human echocardiography, have used 1.5 as the upper limit of the RI for LA:Ao2D. Regardless, the question of what ratio distinguishes cats with normal left atrial dimensions from those with LAE is not one that can be answered by our data. However, it can be stated that for 90% of cats in which we echocardiographically identified cardiac disease, LA:Ao2D was less than 1.51. It is relevant that LA:Ao >1.5 is associated with poor clinical outcome in feline patients with HCM. 18
Interestingly, no association was found between LAE and the presence of a gallop sound. It is possible that gallop sounds noted in the medical record were transient sounds other than third or fourth heart sounds. This, and with regard to the occurrence of gallop sounds, a small sample size, might explain the lack of association between LAE and this auscultatory finding.
It previously has been shown that cats with subclinical HCM weigh more than cats that do not have HCM.2,19 Our data are consistent with this finding in that cats with echocardiographically identified cardiac disease were heavier than those without. However, male cats in our study weighed more than female cats. To our knowledge, others who have evaluated similar populations have not compared body weight across sex, but it presents a difficulty in the interpretation of our data. A predominance of males in cats with HCM and larger proportions of male cats relative to control groups has consistently been shown. It is unclear whether our results with regard to body weight reflect a sex predisposition, a tendency of heavier cats to develop cardiac disease, or both.
We identified male sex, and a murmur intensity ⩾grade 3/6, as independent predictors of echocardiographic identification of cardiac disease. The ORs suggest modest effect sizes. The odds of a cat with a murmur intensity ⩾grade 3/6, whether male or female, are 2.6 times that of a cat with a softer murmur. Independent of murmur intensity, the odds that a male cat will have echocardiographically evident cardiac disease are 2.5 times that of a female cat. Expressed in terms of probabilities, female cats with soft murmurs are less likely than not to have cardiac disease, while the probability that a male cat with a loud murmur has cardiac disease exceeds 75%. These findings are generally consistent with previously published data. 2 Disparities might reflect differences in population – all of our patients were referred, and all had murmurs – and perhaps numbers of cats that were examined.
The results of this investigation must be considered in the context of its limitations. Most obviously, the data were acquired retrospectively. Conclusions regarding diagnoses were based on those recorded in the medical record and, as is inevitably the case with retrospective studies, there were occasional instances of missing data. Although all examinations were performed by veterinary cardiologists or residents under supervision, the echocardiographic methods, including the assessment of left atrial size, were not prospectively determined and it is not possible to account for inter-operator variability and the variation in interpretations that might result. In addition, because the study was retrospective and not ‘blinded’, there might be a bias on the part of attending clinicians to identify, or not identify, cardiac disease based on features of the history and perceived attitudes of the client, and these factors were not evaluated in this study. We collectively considered patients with LVH to have a ‘HCM-P’; circulating thyroxine concentration and systemic arterial blood pressure were inconsistently evaluated, so it is not known with certainty what proportion of those with LVH had cardiac disease that was secondary to endocrine or hemodynamic factors.
There is also the possibility of referral bias. It might be that factors that we did not consider determine whether or not patients are referred, in which case, the characteristics of the sample that we evaluated might not be representative of the population of cats with subclinical cardiac murmurs. For example, cats that have louder murmurs might be more likely to be referred. If this were the case, it would bias the estimated prevalence of cardiac disease, although the associations between murmur intensity and presence of disease are valid within the precision of the estimates. Given the known variation in intensity of feline murmurs, and the inter-observer variation in murmur description, the auscultatory findings that were subject to analysis in our study might be inconsistent with the findings that actually prompted referral. This shortcoming is inherent in the retrospective study design, but might limit the extent to which our results can be generalized to first-opinion practice.
Despite these limitations, our findings shed light on clinically relevant questions and are generally concordant with what might have been predicted based on published literature.
Conclusions
Although a substantive proportion of feline patients that are referred for evaluation of subclinical cardiac disease are free of cardiac disease, the majority have echocardiographically evident cardiac disease, and most of them have LVH. Cardiac disease in this population is relatively mild based on prevalence of LAE. Male sex and a loud murmur might predict echocardiographic confirmation of cardiac disease in this population.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognized high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee was therefore not necessarily required.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) undertaken. No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.