
Abstract
Objectives
Urinary tract infections (UTIs) are reported to be relatively common in hyperthyroid cats, with prevalence rates ranging from 12% to 22%. Factors that are associated with UTIs include age, decreasing body weight and active urine sediments. The purpose of this study was to investigate the prevalence of positive urine cultures (PUCs) in hyperthyroid cats and associated risk factors for PUC.
Methods
In total, 197 hyperthyroid cats presenting for radioiodine therapy had urine cultures prospectively performed on cystocentesis samples. Data pertaining to clinical signs, drug history, age, weight, blood urea nitrogen, creatinine, serum thyroxine and urinalysis were also evaluated.
Results
The prevalence of PUCs in this population of hyperthyroid cats was 5.1% and all cats were subclinical. Microscopic bacteriuria was significantly associated with a PUC (60%) compared with a negative urine culture (1.6%) status. Age, weight, urine specific gravity <1.020, urine pH, hematuria, pyuria, thyroxine concentration, breed and sex were not associated with PUC status.
Conclusions and relevance
The prevalence of PUCs in this population of cats was lower than previous reports of cats with hyperthyroidism. Cats with a PUC were subclinical at the time of culture, regardless of urine sediment abnormalities. Further studies are necessary to determine the clinical significance of subclinical bacteriuria in hyperthyroid cats.
Introduction
Bacterial urinary tract infections (UTIs) are reported to be uncommon in cats. However, in retrospective studies, older age, female sex and concurrent diseases such as chronic kidney disease (CKD), diabetes mellitus and hyperthyroidism have been associated with a higher prevalence of UTIs in cats.1–5 Bacterial UTIs are subcategorized as clinical or subclinical bacteriuria. Bacterial cystitis is defined as a bacterial infection of the bladder resulting in inflammation with corresponding clinical signs of pollakiuria, dysuria, stranguria and/or macroscopic hematuria. 6 Subclinical bacteriuria, in contrast, is determined by the presence of bacteria based on a positive bacterial culture from a properly collected urine specimen in the absence of the aforementioned clinical signs. 6 In hyperthyroid cats, retrospective studies have found that the prevalence of UTIs ranges from 12% to 22%, with the majority having subclinical bacteriuria.2,5 One of these studies concluded that urine culture should be included as a part of routine work-up for all hyperthyroid cats. 2 However, the prevalence of subclinical bacteriuria in apparently healthy cats ⩾7 years of age is not dissimilar, at 10–13%. 4 There is a broad range of positive urine culture (PUC) prevalence in studies of cats without lower urinary tract signs when cats of all ages are evaluated (0.9–28.8%).1,7 Mechanisms for a predisposition of UTIs in hyperthyroid cats proposed by some authors include reduced urine specific gravity (USG) and increased cortisol secretion due to activation of the hypothalamic–pituitary–adrenal axis.5,8 Although neither of these has been directly associated with UTI in hyperthyroid cats, they could, along with increased age and comorbidities of renal disease, account for the previously reported high prevalence of UTIs in hyperthyroid cats. However, to our knowledge, a predisposition to UTIs in humans with hyperthyroidism has not been reported.
Recommendations to perform urine cultures routinely in hyperthyroid cats without signs of cystitis could unnecessarily add to client expense and lead to the inappropriate use of antimicrobial therapy. Treatment of cats with subclinical bacteriuria may not be warranted and, in fact, might be harmful. 6 It is our impression that the prevalence of bacteriuria and UTIs in hyperthyroid cats presenting for radioiodine therapy at our institution is lower than reported by Mayer-Roenne et al and Bailiff et al.2,5 Additionally, in agreement with the aforementioned studies, our observation is that few, if any, have had signs of cystitis, which makes us question the value of routinely performing urine culture in hyperthyroid cats.The primary aim of this study was to determine the prevalence of PUCs in a large number of cats with hyperthyroidism presenting for radioiodine therapy. The second aim of this study was to identify risk factors for a PUC in hyperthyroid cats.
Materials and methods
All cats evaluated for radioiodine treatment of hyperthyroidism, confirmed by increased serum total thyroxine (T4) and/or thyroid scintigraphy, at the Virginia-Maryland College of Veterinary Medicine from September 2008 to June 2016 were enrolled in the study with signed owner consent forms at presentation for radioactive iodine therapy. Evaluation of cats during this time frame was based on our hospital’s protocol for screening patients for radioiodine. This protocol includes collection of a complete history, physical examination, complete blood count, biochemical profile and urinalysis via cystocentesis. For the purposes of this study, bacterial culture and sensitivity was performed on all urine specimens obtained. Procedures that would not be performed routinely on cats presenting for radioiodine treatment were not performed for the purposes of this study.Cats were excluded, retrospectively, if they had been administered oral antibiotics or methimazole within 2 weeks or cefovecin within 3 weeks of presentation for radioiodine and if urine could not be collected for urinalysis by cystocentesis and concurrent quantitative aerobic urine culture. Data, including age, sex, breed, body weight, serum concentrations of blood urea nitrogen (BUN), creatinine, T4, urinalysis parameters, urine culture results, medication history, concurrent diseases and clinical signs of cystitis (macroscopic hematuria, stranguria, pollakiuria and periuria), were collected from the medical records retrospectively.
Urinalysis
Urine was collected for urinalysis and plating for quantitative aerobic culture performed within 30 mins of collection by the Virginia Tech Animal Laboratory Service. Urine collection was performed via cystocentesis blindly or with ultrasound guidance by a trained veterinary technician, doctor or senior veterinary student who was directly supervised. Pyuria was defined as >5 white blood cells/high power field (hpf) and hematuria as >20 red blood cells/hpf. Urine samples were plated on blood agar plates and MacConkey agar (MAC) plates. Blood agar plates were incubated for 24 h at 35°C with CO2 and MAC at 35°C for 24 h. Plates were checked for growth after 24 h. If no growth was detected within 24 h, plates were incubated for an additional 24 h before being categorized as negative. Colony counts were performed on all urine samples from which growth was obtained and microorganisms were identified. Colony counts ⩾1000 colony-forming units (cfu)/ml were recorded as a PUC. Cats with colony counts >0 but <1000 cfu/ml were excluded from the study following exclusion criteria of previous studies over concerns about contamination. 9
Statistical analysis
The primary outcome was occurrence of a PUC. Continuous risk factors were age, body weight, BUN, creatinine, serum T4 and urine pH. Categorical factors included breed, sex, USG <1.020, pyuria, hematuria and bacteriuria. Normal probability plots showed that age, body weight and pH followed a normal distribution, while creatinine, BUN and T4 were skewed. Accordingly, continuous risk factors were summarized as means ± SD for normally distributed data or as median (range) for skewed data. Categorical risk factors were summarized as contingency tables. Bivariable associations between PUC and risk factors were assessed using the two-sample t-test (age, body weight and pH), the Wilcoxon rank sum test (creatinine, BUN and T4) and Fisher’s exact test (all categorical variables). Multivariable analysis was not attempted because there were few (n = 10) positive cases found for the primary outcome. Statistical significance was set to P <0.05. P values were adjusted for multiple testing using the Benjamini–Hochberg false discovery rate method. All analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Results
A total of 261 hyperthyroid cats were initially enrolled. Sixty-four of these were excluded due to lack of urine culture (n = 19) or urinalysis (n = 1) having been performed, urine bacterial growth >0 but <1000 cfu/ml (n = 2), recent antimicrobial administration (n = 14), use of a free catch collection method (n = 13) or where the method was not specified (n = 15). Thus, a total of 197 hyperthyroid cats were included in the analysis.Urine collection was performed by cystocentesis. Urine culture was positive in 10 cats and negative in 187 cats, resulting in a PUC prevalence of 5.1% (95% confidence interval 2.0–8.2). Clinical signs of cystitis were not present in any cat at the time of evaluation. In the documentation of previous illness for all cats in this population, a tentative diagnosis of feline lower urinary tract disease was made in eight cats, with all being urine culture negative during this evaluation. A total of 145 cats were treated with methimazole prior to referral. Concurrent illness was documented in 32 cats, which included CKD (n = 5), tentative feline asthma (n = 4), tentative chronic enteropathy (n = 3), hypertension (n = 2), megacolon (n = 1), tentative hepatopathy (n = 2), osteoarthritis (n = 2), dermatitis (n = 2), chronic upper respiratory infection (n = 2), keratitis (n = 1), conjunctivitis (n = 1), atrioventricular block (n = 1), subcutaneous abscess (n = 1), small cell lymphoma (n = 1), primary pulmonary neoplasia (n = 1), partial extrahepatic bile duct obstruction (n = 1), immune-mediated hemolytic anemia (n = 1), inflammatory bowel disease (n = 1), feline immunodeficiency virus (n = 1), stomatitis (n = 1), small intestinal mass (n = 1) and oral ulceration (n = 1).
The mean ± SD age and weight of all cats was 13 ± 2.36 years and 4 ± 1.15 kg, respectively. Breeds included 182 (92.4%) domestic shorthair (DSH) or longhair (DLH) cats, nine Siamese (4.6%), one Himalayan (0.5%), one Russian Blue (0.5%), two mixed (1.0%), one Maine Coon (0.5%) and one Manx (0.5%). Ninety-nine (50.3%) were castrated males and 98 (49.7%) were spayed females. Age, weight, breed and sex were not significant risk factors for PUC (Table 1).
Selected variables in hyperthyroid cats with positive (PUC) and negative urine cultures (NUC)
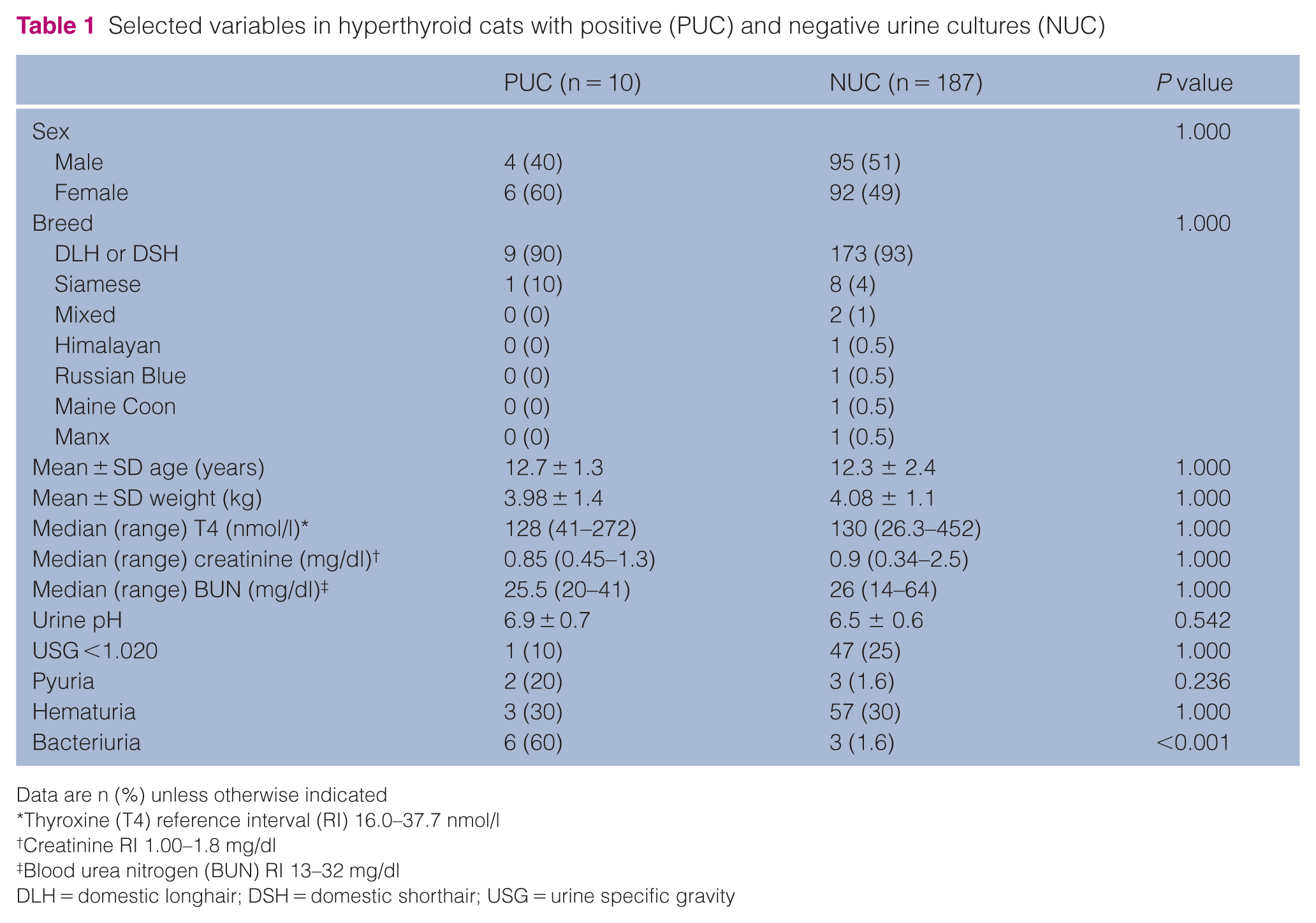
Data are n (%) unless otherwise indicated
Thyroxine (T4) reference interval (RI) 16.0–37.7 nmol/l
Creatinine RI 1.00–1.8 mg/dl
Blood urea nitrogen (BUN) RI 13–32 mg/dl
DLH = domestic longhair; DSH = domestic shorthair; USG = urine specific gravity
Serum concentrations of urea or creatinine were above their respective reference intervals in 1/10 (10%) and 37/187 (20%), and 0/10 (0%) and 6/187 (3.2%) cats with PUCs and negative urine cultures (NUCs), respectively. The proportions of cats with a USG concentration <1.020 with PUCs and NUCs were not significantly different (Table 1). Serum urea, creatinine and T4 concentrations were not associated with urine culture outcome (Table 1). The proportions of cats treated previously with methimazole with PUCs (n = 8/10; 80%) and NUCs (n = 137/187; 73%) were not significantly different (P = 1.00). The presence of microscopic bacteriuria was associated with PUC outcome (Table 1).
Four of the PUC isolates were Escherichia coli (3000 cfu/ml, >100,000 cfu/ml, >100,000 cfu/ml, >100,000 cfu/ml), two were Enterococcus species (>100,000 cfu/ml, >100,000 cfu/ml) and one isolate each was coagulase-negative Staphylococcus species (>100,000 cfu/ml), Corynebacterium species (3300 cfu/ml), Streptococcus species (2500 cfu/ml) and Pasteurella species (>100,000 cfu/ml). None of the individual cats with PUCs had multiple bacterial isolates.
Of the 10 cats with PUCs, five were prescribed antimicrobials and five were not. Two of the latter cats had a repeat urine culture 1 month later, and both were negative. The remaining eight cats did not have a subsequent urine culture performed, but six had a follow-up urinalysis performed 1–5 months later. Microscopic bacteriuria was present in 3/6 cats, two of which were, and one of which was not, treated with antimicrobials. All 10 cats with PUCs had follow-up serum BUN, creatinine and T4 concentrations measured at 1, 3 and 6 months, and one cat had an additional measurement at 8 months. Two cats developed azotemia after radioiodine treatment at 2 and 8 months, respectively. The former developed subclinical hypothyroidism concurrent with azotemia and had persistent microscopic bacteriuria despite antimicrobial treatment. The latter, which developed overt hypothyroidism concurrent with azotemia, had a PUC that was treated with antimicrobial therapy at the time of radioactive iodine therapy.
Discussion
In contrast to retrospective studies with a relatively high prevalence of UTI in hyperthyroid cats (12–22%), the present study documented a prevalence of only 5.1% in hyperthyroid cats presenting for radioiodine therapy. None of the cats had clinical signs of cystitis. Because urine culture was performed in all cats presented for treatment of hyperthyroidism in which urine was able to be obtained, the findings in the present study are likely to be a more robust estimate of the point prevalence of PUCs in hyperthyroid cats as cases were not selected based on the presence of clinical signs of cystitis. However, the vast majority of cats had previously been administered methimazole for some period of time, which one could argue may have had some unproven protective effect against UTI with the resultant control of the hyperthyroid state masking any predisposition to infection the disease might cause.The prevalence of subclinical bacteriuria in healthy cats varies depending on age (1% in cats with a median age of 4 years and 10–13% in cats aged >7 years) and study design.4,7 Estimates of the prevalence of subclinical bacteriuria in unselected populations of cats, including healthy and ill cats, range from 6.2% to 28.8%.1,9 The disparity between these studies illustrates that comparison between studies with different methods and populations is problematic. A limitation of our study is the lack of inclusion of a control population. Inclusion of a control group would have expanded the study to allow additional conclusions to be made. With a PUC prevalence of only 5.1%, hyperthyroidism as a substantial risk factor for subclinical bacteriuria or for UTI is questionable. Prospective studies would be necessary to elucidate the risk in this population of cats.
In this population of hyperthyroid cats with PUCs, the most common Gram-negative isolate identified was E coli and the most common Gram-positive isolate was Enterococcus species. This correlates with previously published studies of cats with lower urinary tract disease in the bacterial isolates identified. 1
The clinical relevance of subclinical bacteriuria in cats is unclear and was not addressed in the present study. In the only study we are aware of that evaluated urine cultures repeatedly, there was no evidence that subclinical bacteriuria was harmful, since survival was not affected despite persistence of infection in many cats. 4 Microscopic bacteriuria persisted in 3/6 cats in the present study, while NUCs were obtained from the two cats that had urine culture repeated after radioiodine treatment. Unfortunately, the present study did not have a consistent protocol in place for management or follow-up of cats with PUCs, and as this was a small population of cats, an overall conclusion cannot be made. In general, treatment of subclinical bacteriuria is not recommended in humans. While there is little information regarding the natural history of subclinical bacteriuria in cats, a recent consensus statement recommended against treatment. 6
Our study has several limitations. Sixteen percent of hyperthyroid cats presented for assessment for radioiodine treatment were found to have concurrent diseases. 10 All cats presenting for radioiodine treatment in this study had no current signs of cystitis. The majority of cats were previously treated with methimazole prior to referral for iodine therapy. It was not possible to ascertain if cats treated with methimazole became euthyroid at any point and, if so, the duration of control of hyperthyroidism. However, no cat had received methimazole within 2 weeks of evaluation for this study. Whether 2 weeks is long enough for any hypothetical therapeutic or protective effect of methimazole against bacteriuria to resolve is unknown. In our study, there is not a clear explanation for the difference in PUC prevalence in comparison to previous studies. For this population of hyperthyroid cats presenting for radioiodine therapy, it is uncertain if these patients were screened prior to referral to our hospital and could be another explanation for the low prevalence of subclinical bacteriuria seen.
Conclusions
The prevalence of PUC in hyperthyroid cats presenting for radioactive iodine is low. Cats with active urine sediments as indicated by bacteriuria are more likely to have PUCs. We consecutively enrolled cats in this study over 8 years, and did not use the presence or absence of signs of cystitis as criteria for enrolment. Yet, no cats had such signs. It remains unclear whether subclinical bacteriuria in hyperthyroid cats resolves after radioiodine treatment or persists. Future prospective studies of clinical outcomes are necessary to make evidence-based clinical recommendations for or against urine culture in hyperthyroid cats.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (owned or unowned), and followed established internationally recognized high standards (‘best practice’) of individual veterinary clinical patient care. Ethical approval from a committee was not necessarily required.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work for the procedure(s) undertaken. For any animals or humans individually identifiable within this publication, informed consent for their use in the publication (verbal or written) was obtained from the people involved.