
Abstract
The association between urolithiasis and growth of bacteria in the urine or urolith has not been recently evaluated in the past 15 years, and the effects of antimicrobial administration on urolith cultures have not been reported. As well, laboratory techniques for urolith cultures have not been critically evaluated. The objectives of the current study were to 1) report bacterial isolates from uroliths and their association with signalment, urolith composition, antimicrobial use, and urine cultures and 2) evaluate laboratory techniques for urolith cultures. For the first objective, a retrospective search of bacterial isolates cultured from uroliths submitted to the laboratory as well as the signalment, urine culture results, and antimicrobial use were recorded. For the second objective, 50 urolith pairs were cultured by washing each urolith either 1or 4 times and culturing the core. Five hundred twenty canine and 168 feline uroliths were reviewed. Struvite-containing uroliths had an increased prevalence of a positive culture compared to nonstruvite-containing uroliths (P < 0.0001, odds ratio [OR] = 5.4), as did uroliths from female dogs (P < 0.0001, OR = 2.9). No significant difference between culture results and previous antimicrobial administration was found (P = 0.41). Eighteen percent of cases with negative urine cultures had positive urolith cultures. There was no significant difference in core culture results whether the urolith was washed 1 or 4 times (P = 0.07). Urolith culture outcome was not always influenced by previous antimicrobial administration, and bacterial culture of a urolith may not yield the same results as those obtained from the urine. The modified protocol, which requires less time and expense for urolith cultures, may be an acceptable alternative.
Urolithiasis is a common lower urinary tract problem in cats and dogs.1,5 Specific types of uroliths have been associated with bacterial urinary tract infections (UTIs). 4 The association between mineral compositions and bacteria has not been recently evaluated in the past 15 years. Importantly, cultured isolates may change over time.9,11 Furthermore, previous studies did not specify if the patients were receiving antimicrobials at the time the urolith was cultured. Uroliths can also act as a nidus for infection and can be found in dogs with recurrent UTI. 13 It has been reported that bacteria isolated from the urine may differ from what is found in either the urolith or bladder mucosa; therefore, cultures of uroliths are warranted. 2 In human beings, positive urolith cultures are better predictors of potential urosepsis compared to urine collected from the bladder. 6
Methods describing laboratory techniques regarding urolith cultures have been reported.2,3 Oftentimes, a urolith is washed with sterile saline at least 3 or 4 times to remove any superficial bacteria that may have contaminated the stone. By convention, after the fourth wash, the wash and the core of the urolith are cultured for aerobic bacteria. Any pathogens grown from the core of the urolith are usually reported. Other methods have described washing the urolith with alcohol. 2 Laboratory protocols for urolith cultures have not been prospectively evaluated.
Therefore, the objective of the current study was to 1) retrospectively evaluate canine and feline urolith cultures and their association with mineral composition, signalment, urine cultures, and previous antimicrobial administration; and 2) prospectively evaluate 2 laboratory protocols for urolith cultures.
Materials and methods
Data collection
For the retrospective study, records from the Gerald V. Ling Urinary Stone Analysis Laboratory, School of Veterinary Medicine, University of California, Davis, between July 2008 and June 2010 were reviewed to find canine and feline uroliths that were analyzed for their mineral content and submitted for urolith culture. To determine the mineral composition of uroliths, each visibly distinct layer of the urolith was initially analyzed by use of the oil-immersion method of optical crystallography with polarizing light microscopy as previously described. 10 Urolith cultures were performed in the following manner. Each urolith was washed 4 times with 50 ml of sterile saline for 10 sec. The urolith was then cracked with sterile rongeurs, and the core was scraped into a sterile mortar. One milliliter of sterile saline was added to grind the sample, and a 0.1-ml aliquot of this sample was cultured for aerobic bacteria as previously described. 12 A 0.1-ml aliquot of the first and fourth wash was also cultured for aerobic bacteria.
Specimens submitted to the Stone Analysis Laboratory had been accompanied by information from the referring veterinarian that included the patient’s age, sex, as well as whether or not urine had been cultured. Urine cultures were not performed at the study laboratory, therefore a standard protocol cannot be reported. If the urine was submitted for culture by the primary care veterinarian, the result of that culture was reported on the submittal form, and the data was recorded. Furthermore, any previous antimicrobial administration at the time of stone removal was also recorded.
Laboratory protocol for urolith culture
For the prospective study, 50 similarly sized uroliths submitted in pairs from the same patient from June to December 2010 were analyzed. One urolith of the pair was washed once in 50 ml of sterile saline for 10 sec. The other urolith was washed 4 times in the exact same manner. Each urolith was then processed as described above. A 0.1-ml aliquot of the first and fourth wash, when available, was also cultured for aerobic bacteria to evaluate the need for this step in the urolith culture protocols.
Statistical analyses
Multiple logistic regressions were performed on the retrospective data to determine the association of signalment and culture results on urolith type. Results are presented as odds ratios (ORs) and 95% confidence intervals (CIs). McNemar test was used to evaluate the prospective paired data; P < 0.05 was considered significant.
Results
Urolith cultures
During the retrospective study period, 1,584 calcium oxalate (CaOx)-, 1,406 struvite-, and 346 urate-containing uroliths were analyzed. Of these uroliths, 688 were cultured at the request of the referring veterinarian. As only 64 of the urate-containing uroliths were cultured, only cultures from CaOx- and struvite-containing uroliths were included in the data analysis. Therefore, records from 520 canine (271 male and 249 female) and 168 feline (94 male and 74 female) uroliths were reviewed.
One hundred fifty-six out of the 688 (23%) urolith cultures were positive on aerobic culture. Of these, 144 (92%) were from dogs and 12 (8%) were submitted from cats. Struvite-containing uroliths were more likely than CaOx-containing uroliths to be associated with positive cultures (107/240, 44.5% vs. 37/280, 13.2%, respectively; OR = 5.4, 95% CI: 3.5–8.4), and females were almost 3 times as likely to have a positive culture (OR = 2.9, 95% CI: 4.19–4.3). Dogs less than 7 years of age had a lower prevalence of positive urolith culture (OR = 0.4, 95% CI: 0.3–0.6).
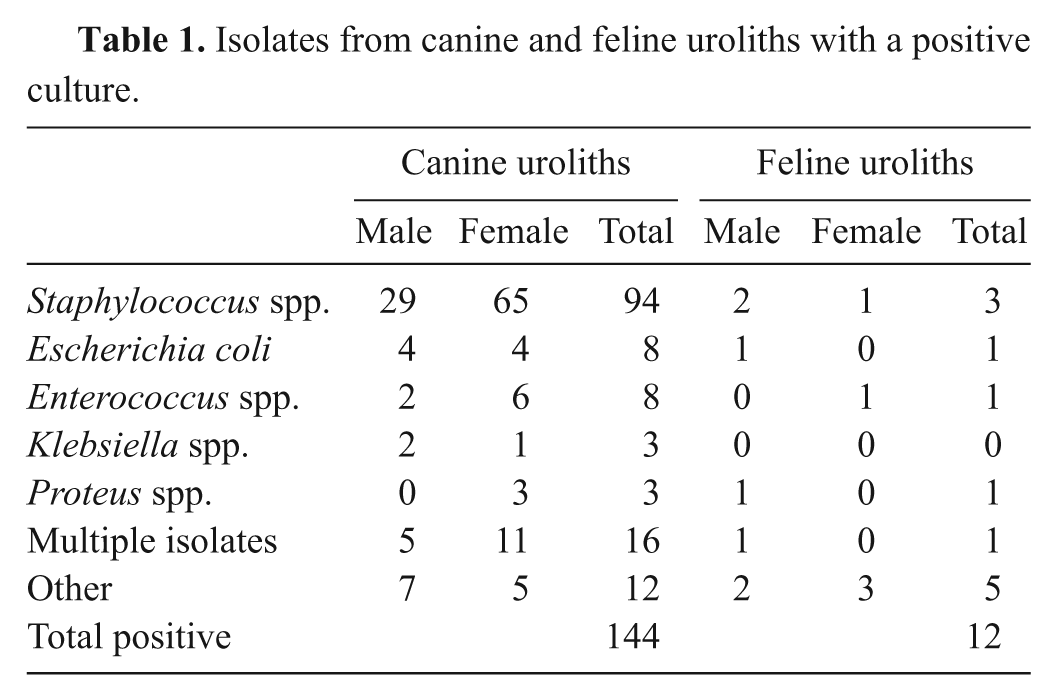
The most common pathogens isolated from canine and feline uroliths are found in Table 1. Of the 144 canine samples, 94 (65%) had growth of a Staphylococcus species. Struvite-containing uroliths had more than 9 times the prevalence for growth of Staphylococcus spp. (OR = 9.5, 95% CI: 5.2–18.6, P < 0.0001); conversely, CaOx-containing uroliths were negatively associated with Staphylococcus cultures (OR = 0.12, 95% CI: 0.05–0.25, P < 0.0001).
Isolates from canine and feline uroliths with a positive culture.
Urine cultures at time of urolith submission
Of the 520 uroliths submitted from dogs, 196 (38%) also had urine submitted for bacterial culture. The most common urinary pathogens reported are shown in Table 2. Eighty-six of the 196 (44%) urine cultures were positive for bacteria; 45 of these (52%) had growth of Staphylococcus spp. Twelve of the positive urine cultures (14%) had ≥2 bacterial isolates. Struvite-containing uroliths were 9 times more likely to have multiple bacteria present (OR = 9.0, 95% CI: 2.0–55.5, P < 0.001).
Isolates from urine cultures with respect to urolith composition in dogs.*
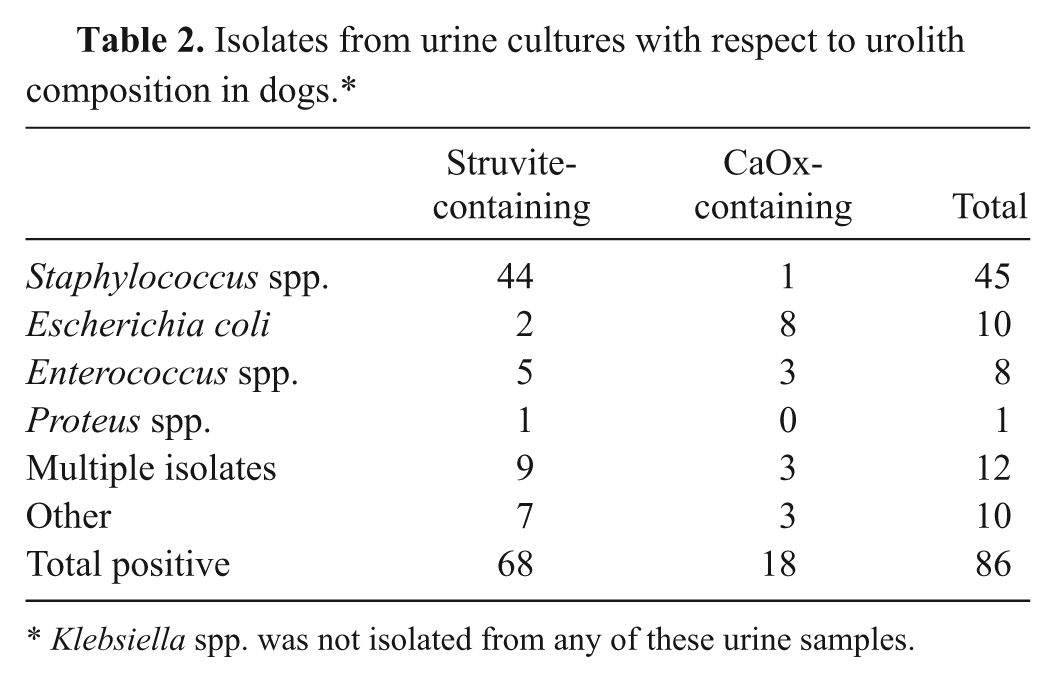
Klebsiella spp. was not isolated from any of these urine samples.
When comparing canine urine and urolith cultures from the same dog, only 30 (34%) of the urolith cultures had growth of the same pathogen that was reported in the urine. Eighteen percent of canine samples that had negative urine cultures had positive growth from the urolith; while 12% (10) had growth of a different organism compared to that isolated in the urine. Forty-six (54%) of the samples did not have growth reported for the urolith, despite a positive urine culture result.
Previous antimicrobial administration
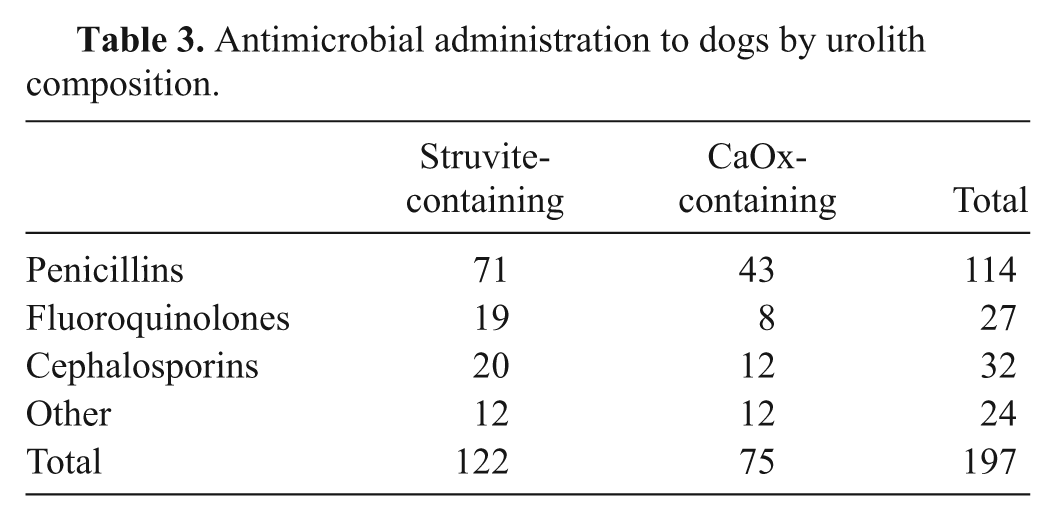
Of the 520 canine uroliths submitted for culture, information regarding use of antimicrobials was reported for 320 (62%). One hundred ninety-seven (38%) dogs were receiving antimicrobials at the time of urolith removal, whereas in 123 (24%) of the cases, antimicrobials were not administered. The most common antimicrobial classes reported by the referring veterinarians were penicillins, fluoroquinolones, and cephalosporins. The antimicrobials administered to dogs with struvite-containing versus CaOx-containing uroliths are shown in Table 3. Forty-nine of 144 (34.0%) of patients that received antimicrobials had positive cultures, and 148 out of 376 (39.4%) of patients that received antimicrobials had negative cultures; these differences were not significant (P = 0.41). Of the 168 uroliths submitted from cats, information regarding antimicrobial administration was reported for 81 (48%). Forty-nine (29%) were receiving antimicrobials, whereas 32 (19%) had not been given antimicrobials. There were too few numbers of feline patients given antimicrobials to be of statistical significance.
Antimicrobial administration to dogs by urolith composition.
Urolith culture protocols
When prospectively evaluating culture results from the 2 urolith wash protocols, 7 out of 50 (14%) had a positive urolith core culture when the first wash was negative for bacterial growth, but there were no instances where either the first or fourth wash was positive and the urolith core was negative (P < 0.001). No statistically significant difference was found for core culture result outcome if the urolith was washed 1 or 4 times (P = 0.071). When differences were present, it was generally a slight difference in the number of colony forming units of the organism reported. Information regarding antimicrobial use was available for 24 of these 50 cases; 16 out of 24 (67%) received antimicrobials. Only 1 case that had different core culture results when evaluating the 2 protocols had received an antimicrobial.
Discussion
In the current study, strong associations among Staphylococcus spp. infections, female dogs, and struvite-containing uroliths have been shown. These findings are similar to a previous publication, 4 and the relationship between infection caused by Staphylococcus spp. and struvite urolithiasis in dogs has been reported. 7 Struvite-containing uroliths usually form in dogs secondary to a UTI, with urease-producing bacteria, such as many species of staphylococci including Staphylococcus pseudintermedius. This occurs because such pathogens have the ability to hydrolyze urea into ammonia, bicarbonate, and carbonate. The resulting increase in urine pH results in urinary supersaturation of the ions necessary to form magnesium ammonium phosphate uroliths. 8 Staphylococcus spp. were the most common organisms isolated in the current study, although the urease-producing abilities of these organisms were not tested for all isolates. A similar finding has been previously reported, 3 but comparisons with another study are difficult to make due to a small sample size. 2
Unlike previous studies, the impact of antimicrobial use was investigated in the current study. Almost 40% of dogs were receiving antimicrobials just prior to urolith removal, and penicillins were the most common antimicrobial administered. Information on the dosages and durations of drug use was not available in the retrospective study. However, when evaluating the 320 dogs where antimicrobial use was reported, no significant difference was noted regarding urolith culture outcome in dogs. Therefore, a urolith culture can be considered for many cases, despite antimicrobial administration. Antimicrobials may not always penetrate the urolith, and positive results can be obtained. However, a negative urolith culture from a dog that was receiving antimicrobials should be interpreted cautiously as more porous uroliths may allow antimicrobial penetration.
In the current study, it was shown that urolith cultures can be clinically relevant even if the urine culture is negative for bacterial growth. A total of 18% of the urine samples that were negative for bacterial growth were positive for bacterial growth when the urolith was cultured in the current study. In a previous study, which prospectively evaluated 27 dogs that had urine, bladder mucosa, and urolith cultures performed, 11% and 7% of the cases had an organism cultured from the urolith or bladder mucosa, respectively, despite a negative urine culture. 3 In that study, antimicrobials were stopped 48 hr prior to the respective cultures. However, it was unclear how long antimicrobials may have been given prior to the study period. In another study, 2 out of 21 (9.5%) of cases evaluated had positive growth for bacteria when the urolith was cultured, despite a negative urine culture. 2 In the current study, urine culture results were not always in agreement with urolith culture results, and different pathogens were also isolated; therefore, analyzing the urolith for bacteria, even when the urine culture is positive, may yield new data. Furthermore, if the urine culture is positive and the urolith culture is negative, treatment for the infection is likely still warranted. Information regarding bacteria present within the uroliths may impact management strategies to prevent urolith recurrence, particularly with struvite urolithiasis. Further studies would be needed to determine if the pathogen identified in the urolith is often found in other sites of the urinary tract, such as the bladder mucosa or renal pelvis. This may be of most concern in dogs with recurrent UTI.
When prospectively evaluating the 2 laboratory protocols for urolith cultures, a statistically significant difference was not found regarding urolith core cultures if the stone was washed 1 or 4 times with sterile saline. Furthermore, reporting the culture results from the saline washes did not provide any additional information and these cultures can be omitted from the protocol. The modified protocol, which requires less time and expense for urolith cultures, may be an acceptable alternative. Performing 1 wash would eliminate extraneous work as well as save expenses of technician time and supplies. The current study only evaluated 50 pairs of uroliths, and it is possible that if more uroliths were analyzed, a difference may be noted. Furthermore, it is not possible to be completely certain that each urolith in the pair would contain the same bacterial numbers. Information regarding antimicrobial use was available for 24 of these cases; 16 (67%) received antimicrobials. It would be expected that any of the antimicrobials present would have had a similar effect on all uroliths present in the bladder at the time the uroliths were removed. Other studies have reported placing uroliths in alcohol prior to washing with sterile saline. 3 This protocol was not evaluated in the current study due to concerns that alcohol may penetrate a porous urolith and result in a false-negative culture.
In conclusion, additional information is provided from urolith cultures that may help tailor management protocols for patients with recurrent uroliths or UTI. Performing urolith cultures in dogs that have received antimicrobial therapy can yield positive results. Furthermore, additional information may be provided by a urolith culture as to what is found in the urine. Finally, a modified protocol for performing urolith cultures may be acceptable. Evaluation of a larger number of uroliths is required to support or refute these preliminary findings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.