
Abstract
Objectives
The aim of our study was to compare the standard fabellotibial suture with Mini TightRope fixation for the treatment of a cranial cruciate ligament (CCL) rupture using a feline custom-made limb press.
Methods
Cadaveric hindlimbs of 10 cats were inserted in the limb press at predefined joint angles and loads of 10% and 30% body weight (BW) were applied. Mediolateral radiographs were taken and three-dimensional coordinates were recorded using a microscribe digitiser, with intact and transected CCLs and after either fabellotibial suture or Mini TightRope fixation were performed. Different distances and angles from radiographs or microscribe coordinates were analysed.
Results
Radiographic distances from the femoral condyle to the cranial edge of the tibia (X1–X2) were higher in CCL-deficient stifles than in intact stifles at 10% and 30% BW loads. All fabellotibial sutures and Mini TightRope fixations neutralised excessive cranial tibial thrust. A significant difference in the distance between the patella and tibial tuberosity (D2) was observed between CCL-deficient limbs and Mini TightRope-fixed limbs at 10% BW load (P <0.04). A significant difference in the distance between the tibial tuberosity and lateral collateral ligament of the femur (D3) was observed between the intact and transected CCLs on the left legs at 10% BW load (P <0.003) and on both legs at 30% BW load (P <0.002). Furthermore, we observed significant differences between CCL-deficient left legs and Mini TightRope-treated legs at 10% BW load (P <0.003). With regard to fabellotibial suture-treated legs, we observed significant differences between transected limbs and fixed limbs at 30% BW load (P <0.004). W1 (craniocaudal angle) and W2 (mediolateral angle) showed significant differences between intact and transected CCLs and between transected and fixed limbs at 30% BW load (P <0.004).
Conclusions and relevance
Fixation of CCL-deficient stifles with lateral fabellotibial suture, as well as Mini TightRope tightened with a 20 N load, produces good biomechanical stability, as detected via radiographic assessment.
Introduction
Cranial cruciate ligament rupture (CCLR) occurs less frequently in cats than in dogs. In cats CCLR occurs most commonly because of trauma, 1 but it can occur in overweight cats without a previous history of trauma. 2
CCLR leads to stifle instability, joint swelling, pain and lameness. Until recently, CCLR was treated conservatively in many cases, but nowadays the treatment of choice is a surgical intervention owing to a quicker return to function.1,2
In a 1990 study, 25 dogs were diagnosed with partial cruciate ligament rupture. The dogs were mainly presented with lameness in the hindlimbs and 52% of the patients had a cranial drawer sign. All of the dogs underwent exploratory surgery and were treated either with fabellotibial suture or fibular head transposition. 3
Currently, lateral extracapsular suture stabilisation and tibial plateau levelling osteotomy are the two most commonly used surgical techniques for the stabilisation of CCLR in dogs. 4 A biomechanical study involving cats reported that the stability shown by fabellotibial sutures, as well as femorotibial sutures positioned at quasi-isometric points in a craniocaudal plane, is similar to that of stifle joints with an intact cranial cruciate ligament (CCL). 5
An alternative technique for CCL repair in dogs is TightRope fixation (Arthrex) and its efficiency has been tested by biomechanical and clinical studies.6,7 The TightRope should reduce internal rotation without leading to external rotation, and is placed at more isometric points than techniques used previously.6–8 The Mini TightRope is a smaller sized suture and is commonly used during human hand surgery.9,10 To our knowledge, none of the previous biomechanical or clinical studies evaluated the Mini TightRope for the stabilisation of CCLR in cats.
As a prerequisite to clinical studies, biomechanical studies aim to evaluate the stability of novel stabilisation techniques.11–13 Kneifel et al 14 compared a standard fabellotibial suture with an under-and-over technique using a limb-press model for cats, modified from a canine model.11,14,15 They used radiography for the evaluation of craniocaudal movements pre- and postoperatively, and demonstrated the utility of the limb-press model for cats. They also demonstrated that an extracapsular nylon suture is superior to an intra-articular technique in neutralising excessive cranial tibial thrust. However, Kneifel et al 14 evaluated only two-dimensional craniocaudal movements with lateral radiographs and not rotational (mediolateral) stability.
In the present study, we compared the standard fabellotibial suture and Mini TightRope fixation using a modified limb-press model for cats. 14 Because the Mini TightRope (or TightRope) is a suture that should be placed more isometrically with less external rotation than a standard fabellotibial suture, we used a three-dimensional measurement method (microscribe digitiser) in our study. We hypothesised that: (1) both surgical techniques would neutralise excessive cranial tibial thrust; and (2) after repair, the Mini TightRope technique would show less external rotation than the fabellotibial suture.
Materials and methods
Cadaveric specimens
Cadaver preparation was performed as described previously (Figure 1 and file 1 in the supplementary material). 15 We obtained the informed consent of the owner/legal custodian for the inclusion of their animals in our study.

Limb press with the specimen in position. Stifle and hock were angulated at 120° of flexion. A radiographic detector plate was mounted at the back of the model
Custom-made limb-press model
The limb press was custom made, as described previously, with slight modifications (Figure 2 and file 2 in the supplementary material). 14

Radiograph of a right stifle with an intact cranial cruciate ligament (ICCL), loaded at 10% body weight (BW), including measurements of the distance between two predefined points ×1 and ×2
Group 1: intact CCL
Each limb (n = 20) was inserted into the limb press at predefined joint angles (stifle joint 120° ± 5°; hock joint 120° ± 5°; hip joint 60°), and fixation screws in the top plate were fixed to keep the limb in the correct position. To achieve the predefined mean patellar tendon load, turnbuckles were tightened and then load was applied until 10% and 30% body weight (BW) were measured on the force plate. For the evaluation of radiographs, a radiographic magnification marker (Biometrix) was positioned at the level of the specimen parallel to the radiographic plate.
Radiographs were taken using a mobile x-ray machine (Toshiba model D 183BS; Gierth X-Ray) and developed digitally (dicomPACS viewer, version 5.2.11). The stifle angle was defined using the tibial functional axis and the femoral diaphyseal axis (caudal part of the metal pipe holding the femur). The angle of the tarsal joint was evaluated using the functional axis of the tibia and a parallel line to the longitudinal axis of metatarsal bones three and four (see Figure 2).14,16
Subsequently, a microscribe digitiser (MicroScribe MX; Solution Technologies) was used to record the three-dimensional coordinates of three predefined test points on the femur (P1–P3), two test points on the tibia and fibula (P4–P5), and three reference points on the limb press (R1–R3) (Figure 3 and file 3 in the supplementary material). We located our test points on specific anatomical landmarks to achieve reproducibility and marked them with waterproof markers.
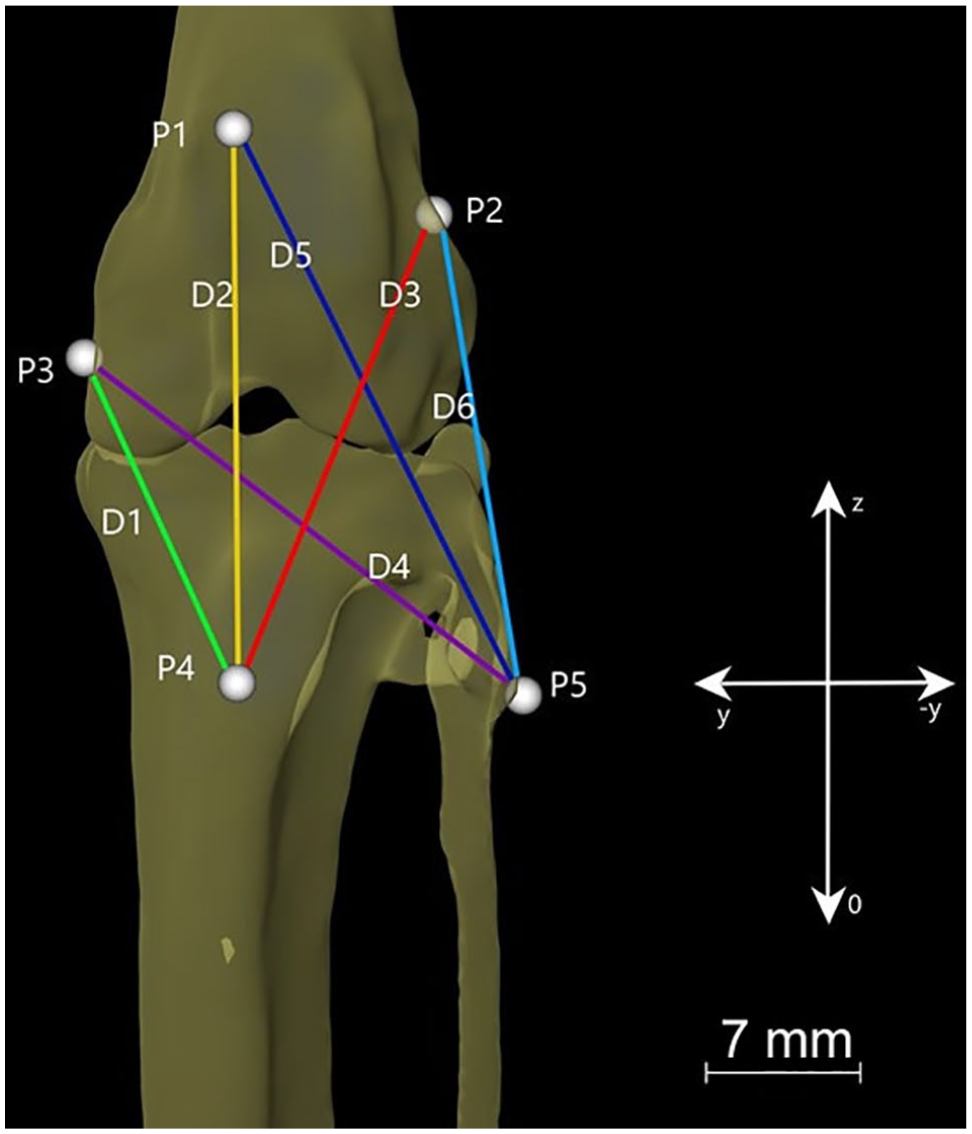
Distances (D1–D6) and test points (P1–P5) in a three-dimensional bone model of the feline stifle
Group 2: transected CCL
Limbs from group 1 (n = 20) were removed from the limb press, CCLs were transected via parapatellar arthrotomy with a #11 blade and the joint capsule was closed with 2-0 polypropylene sutures (PROLENE; Ethicon). After CCL transection (CCLT), limbs were remounted into the limb press and radiographs and microscribe detection was repeated with 10% and 30% BW loads.
Group 3: ‘repair’
After testing, limbs from group 2 (n = 20) were assigned to two subgroups (3a and 3b, n = 10 in each).
In group 3a, Mini TightRope fixation was performed with the Mini TightRope Kit (Arthrex) according to the manufacturer’s guidelines, as described by Cook et al. 8 First, a bone tunnel was drilled from a point 2 mm cranial and distal to the lateral fabella–femoral condyle junction and within the caudal portion of the lateral femoral condyle to the distal diaphysis of the femur on the medial side at the level of the proximal pole of the patella. The second bone tunnel was drilled from a point caudal and distal to the tubercle of Gerdy in a craniodistally directed angle such that the wire traversed the proximal aspect of the tibia and exited the proximal metaphysis of the tibia on the medial side. The fibre tape was passed through the holes, starting proximomedially. On the distal hole, the suture was fixed with the metal loop in position and pulled tight on the lateral aspect of the stifle; all twists were removed so that the strands were flat and firmly against the lateral joint capsule. The knot was tightened on the button on the proximomedial end with 20 N load at a 100° angle position of the stifle. 8
In group 3b, the fabellotibial suture was performed using the CCL Kit Fiberwire #2 (Arthrex). A curved needle was passed around the lateral fabella. A bone tunnel was drilled in the proximal part of the tibial tuberosity, and the suture was led through the bone tunnel. 17 With the straight needle, the patellar tendon was undermined and the knot between the two fibre wire endings was tightened with a 20 N load on the medial side at a 100° angle position of the stifle. A force gauge was used to maintain the 20 N load while tying the knots.
Repaired limbs were inserted in the limb press and radiography and microscribe coordinate detection were performed again with 10% and 30% BW loads.
Measurements
Radiographic assessment
To evaluate translational movements, we measured the distances between two predefined points, X1 and X2 (X1, cranial edge of the tibial plateau; X2, centre of a circle [radius = 6 mm] that was superimposed over the femoral condyles), by radiography (Figure 2). The distances were measured under each condition (intact, Ds; transected, Dt) and after one of the two procedures was performed (De, fabellotibial suture; Dmini, Mini TightRope) with 10% and 30% BW loads.
Microscribe digitising
Microscribe digitising arms (Solution Technologies) were used to record coordinates of P1–P5 and R1–R3 (file 3 in the supplementary material). After coordinate transformation, distances and vector angles between the test points were calculated to approach translation and rotation of the tibia.
Transformation of microscribe point coordinates
Point measurements (P1–P5) were performed for 10 specimens via the microscribe digitising arm as described above. Subsequently, R1–R3 (file 3 in the supplementary material) were used to align each microscribe data set according to a standard coordinate system fixed on the limb press, which represents the three anatomical planes of the limb. For registration, the transformation matrix was calculated for each microscribe data set, which was implemented in a custom-built MATLAB script (MathWorks), using a singular value decomposition approach. Registration of microscribe data allowed measurement of projected distances and angles with reference to the axial, coronal and sagittal planes.
CT scan and visualisation of bone displacements during limb-press experiments
Details of CT scans and visualisation are given in file 4 in the supplementary material.
Distances and angles
Three-dimensional distances (D1–D6; Figure 3) between two predefined test points (coordinates) were calculated using Microsoft Excel (for formulae and calculations, see file 5 in the supplementary material).
Measurement of three-dimensional movements in a craniocaudal plane
The distance between the patella and tibial tuberosity (D2) was calculated to measure cranioproximal or craniocaudal movements of the tibia. Furthermore, an angle was calculated to confirm our measurements of cranial or cranioproximal movements of the tibia. For angle calculations, vectors were drawn between the patella and tibial tuberosity and between the patella and the cranial origin of the coordinate system. In this angle, we only used the x and z coordinates of the test points (Figure 4).

Craniocaudal angle W1 in a mediolateral plane
Measurement of three-dimensional movements in a mediolateral plane
The distance between the tibial tuberosity and medial collateral ligament (D1) and the distance between the tibial tuberosity and lateral collateral ligament (D3) were calculated to provide information about the three-dimensional mediolateral movement of the tibia. Furthermore, to measure mediolateral movements, we calculated an angle by drawing vectors between the patella and tibial tuberosity and between the patella and an auxiliary point (–1000 for the left limb; +1000 for the right limb) by using y and z coordinates of the test points (Figure 5).
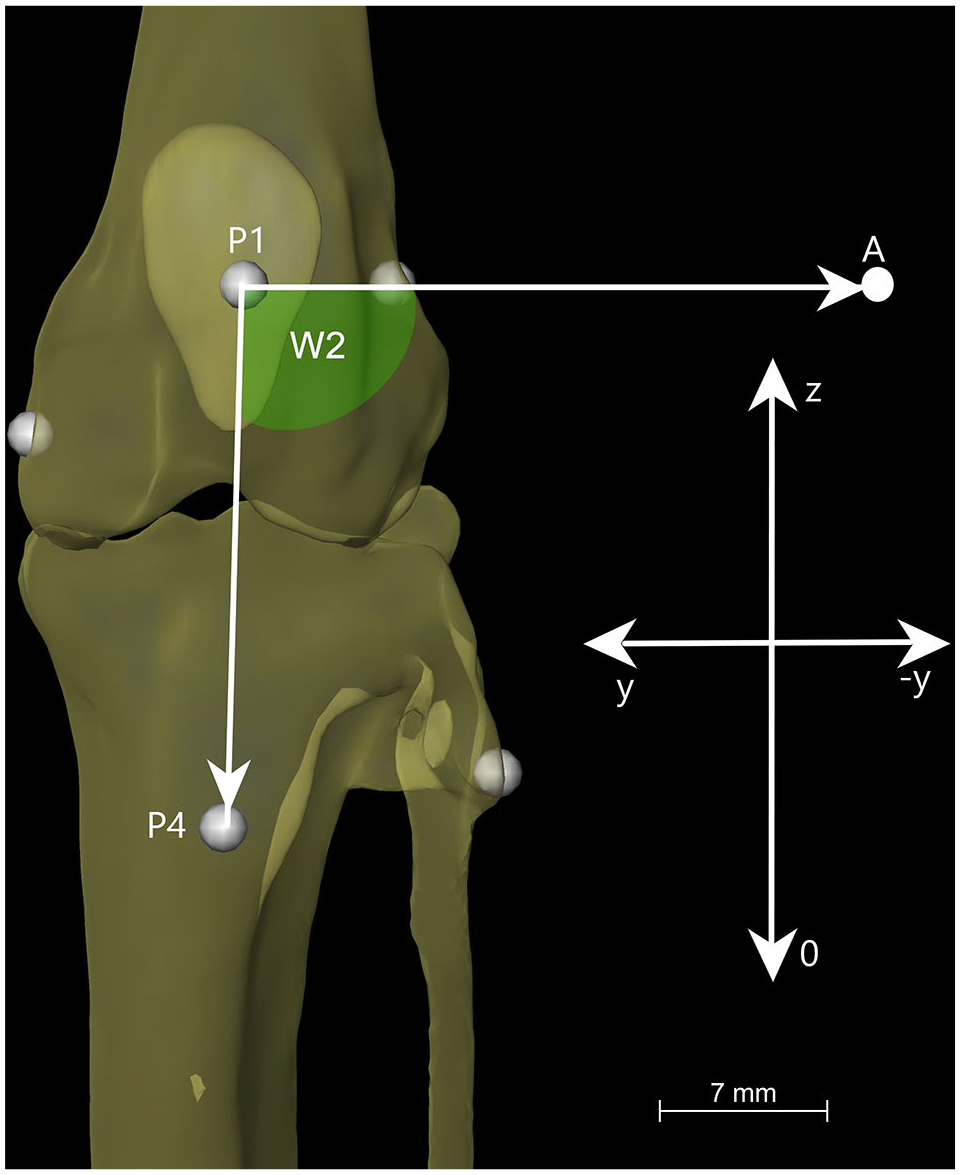
Mediolateral angle W2 in a craniocaudal plane
Statistical analysis
We used a representative sample of 10 cats and the significance power ranged from 0.6 to 0.9. A general linear model (GLM) was used for the repeated measurement of the effect of the two surgical techniques to evaluate the calculated between-load differences. To analyse the impact of each technique on these differences for each load, one-sample t-tests were performed. Pearson’s correlations of BW with the differences between De–Ds and Dmini–Ds, respectively, and Dt–Ds were calculated. Normality of distribution was determined using the Kolmogorov–Smirnov test. A P value <0.05 was considered significant. 15
Within-subject effects were evaluated to compare the techniques under different conditions (10% BW, 30% BW, intact, transected and repaired CCLs).
Results
In this study, five female and five male cats were included (mean ± SD age 8 ± 4.64 years [range 2–16 years]; mean ± SD weight 4.51 ± 1.08 kg [range 3.12–6.5 kg]). Most of the cats were domestic shorthairs (80%); one British Shorthair and one Oriental Shorthair cat were also included.
Measurement of two-dimensional movements in a craniocaudal plane
At 10% BW load, the mean ± SD distances (D = X1–X2; see Figure 2) measured in groups 1, 2, 3a and 3b were 11.65 ± 1.46 mm, 13.25 ± 2.61 mm, 11.60 ± 1.71 and 11.70 ± 1.57 mm, respectively. The corresponding values at 30% BW load were 12.20 ± 1.61 mm, 17.45 ± 2.06 mm, 13.2 ± 2.70 mm and 12.80 ± 2.20, respectively (Table 1).
Descriptive statistics for all measured craniocaudal distances
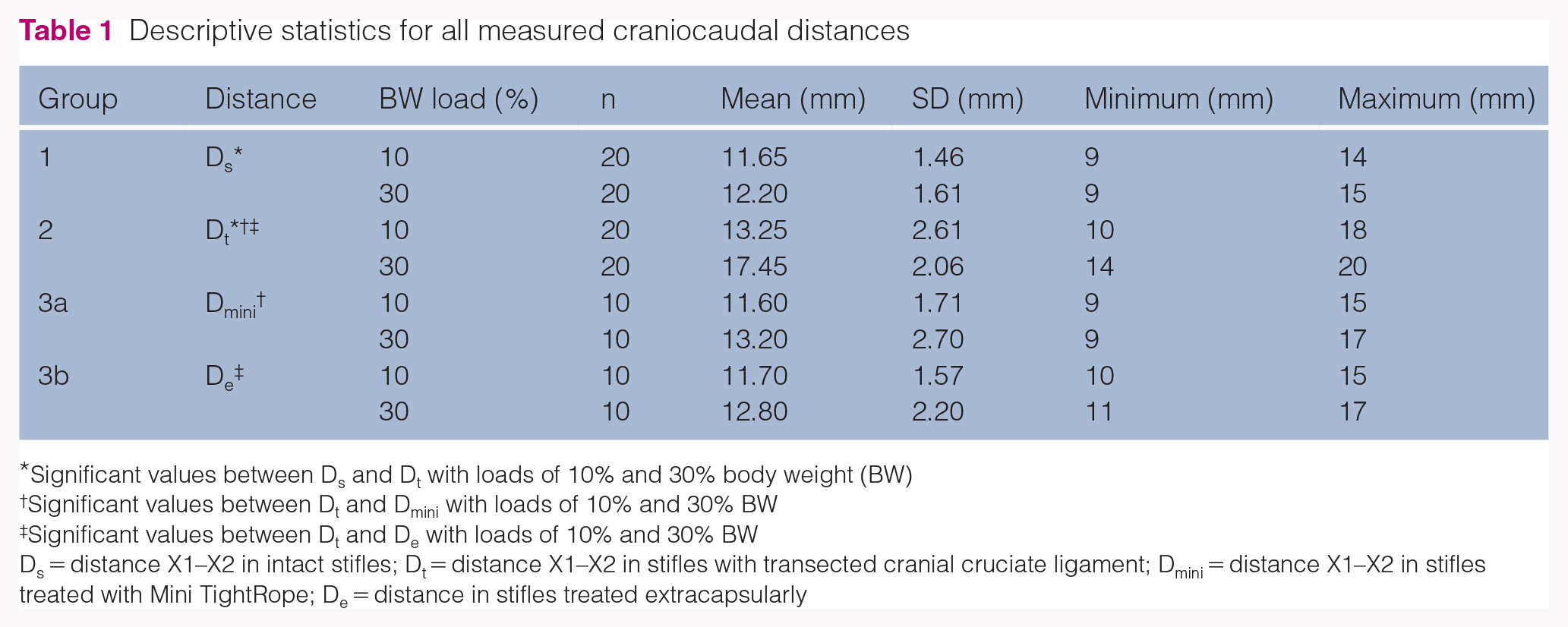
Significant values between Ds and Dt with loads of 10% and 30% body weight (BW)
Significant values between Dt and Dmini with loads of 10% and 30% BW
Significant values between Dt and De with loads of 10% and 30% BW
Ds = distance X1–X2 in intact stifles; Dt = distance X1–X2 in stifles with transected cranial cruciate ligament; Dmini = distance X1–X2 in stifles treated with Mini TightRope; De = distance in stifles treated extracapsularly
A GLM showed significant effects of condition (intact, transected or fixed with one of the two techniques) (f = 86.078, P <0.05) and load (f = 101.482, P <0.05) and a significant interaction between condition and load (f = 44.767, P <0.05). Test of within-subject effects showed a significant effect (P <0.05) of load, condition and load and condition combined on the distance. However, there was no significant difference between the techniques.
Measurement of three-dimensional movements in a craniocaudal plane
The changes in microscribe D2 are shown in Table 2.
Comparison of means for D2 (distance between the patella and tibial tuberosity) with loads of 10% and 30% body weight (BW)

Significant values between groups 2 and 3a at a load of 10% BW
Group 1 = intact cranial cruciate ligament (CCL); group 2 = transected CCL; group 3a = Mini TightRope; group 3b = fabellotibial suture
The following changes were observed in the craniocaudal angle (W1): at 10% BW load, W1 calculated with our point vectors in groups 1, 2, 3a and 3b was 104.60° ± 3.46°, 100.15° ± 7.83°, 103.94° ± 7.06° and 104.18° ± 3.49°, respectively; and at 10% BW load, the corresponding values were 103.14° ± 3.38°, 87.42° ± 4.46°, 97.30° ± 9.68° and 99.48° ± 5.23°, respectively (Table 3).
Comparison of means for W1 (craniocaudal angle) with loads of 10% and 30% body weight (BW)

Significant values between groups 1 and 2 on the right legs with a load of 10% BW
Significant values between groups 2 and 3a and 3b with a load of 10% BW
Significant values between groups 1 and 3a with a load of 10% BW
Significant values between groups 1 and 2 with a load of 30% BW
Significant values between groups 2 and 3a and 3b with a load of 30% BW
Group 1 = intact cranial cruciate ligament (CCL); group 2 = transected CCL; group 3a = Mini TightRope; group 3b = fabellotibial suture
With regard to W1, a test of within-subject effects showed a significant effect of load (f = 139.350; P <0.05), condition (f = 43.051; P <0.05) and load and condition combined (f = 34.228; P <0.05) (Table 3).
Measurement of three-dimensional movements in a mediolateral plane
The changes in microscribe D1 are shown in Table 4.
Comparison of means for D1 (distance between tibial tuberosity and medial collateral ligament) with the loads of 10% and 30% body weight (BW)

There were no statistically significant differences in the values between any of the test groups for D1
Group 1 = intact cranial cruciate ligament (CCL); group 2 = transected CCL; group 3a = Mini TightRope; group 3b = fabellotibial suture
The test of within-subject effects showed a significant effect (f = 9.532; P <0.05) of load on D1. There was no significant effect of condition on D1.
Significant effects of load (f = 24.105; P <0.05), condition (f = 27.718; P <0.05) and load and condition combined (f = 3.275; P <0.05) were observed on D3 (Table 5).
Comparison of means for D3 (distance between tibial tuberosity and lateral collateral ligament) with the loads of 10% and 30% body weight (BW)
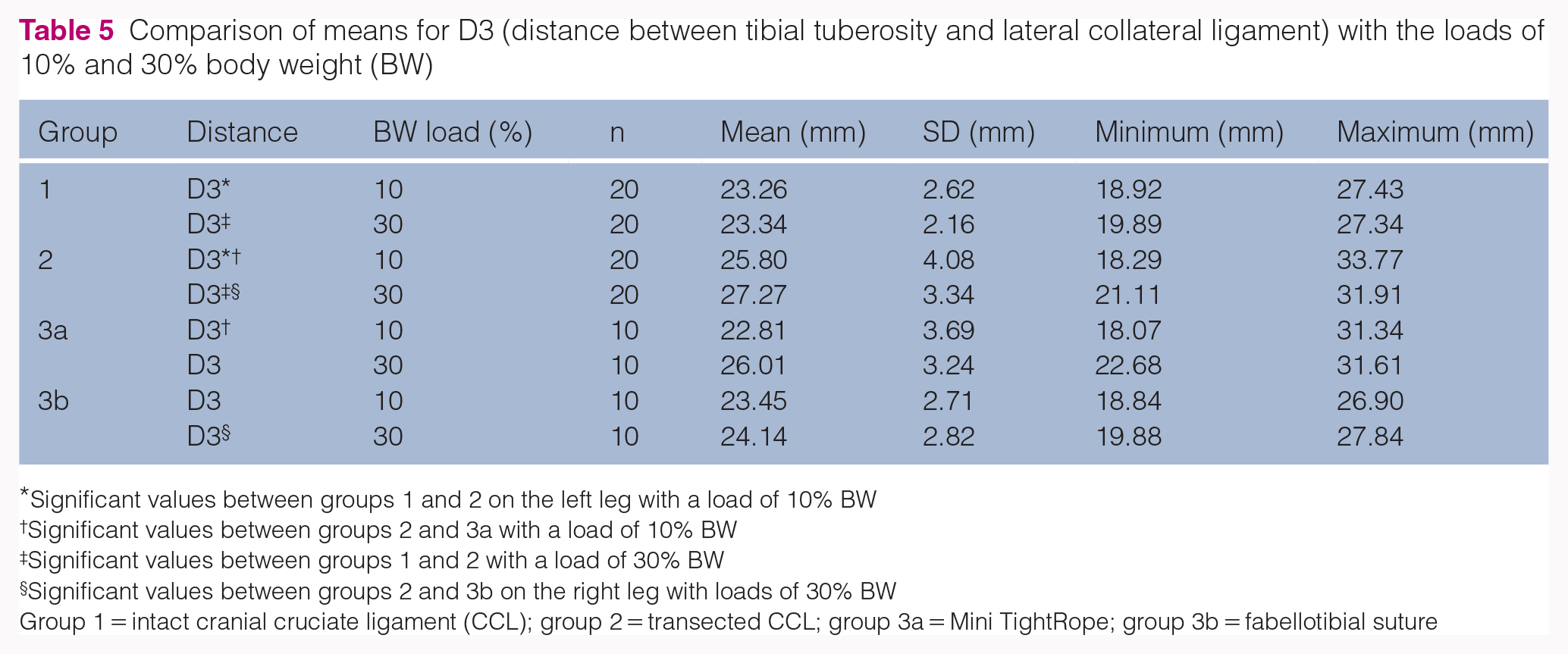
Significant values between groups 1 and 2 on the left leg with a load of 10% BW
Significant values between groups 2 and 3a with a load of 10% BW
Significant values between groups 1 and 2 with a load of 30% BW
Significant values between groups 2 and 3b on the right leg with loads of 30% BW
Group 1 = intact cranial cruciate ligament (CCL); group 2 = transected CCL; group 3a = Mini TightRope; group 3b = fabellotibial suture
At 10% BW load, mediolateral angle (W2) values of groups 1, 2, 3a and 3b were 89.26° ± 5.04°, 91.96° ± 4.41°, 88.70° ± 3.58° and 83.34° ± 3.35°, respectively. At 30% BW load, the corresponding values were 89.93° ± 5.50°, 96.12° ± 3.41°, 91.62° ± 4.23° and 84.55° ± 3.62°, respectively (Table 6).
Comparison of means of W2 (mediolateral angle) with loads of 10% and 30% body weight (BW)

Significant values between groups 1 and 2 on the right leg with a load of 10% BW
Significant values between groups 1 and 2 with a load of 30% BW
Significant values between groups 2 and 3a and 3b with a load of 30% BW
Significant values between groups 1 and 3a on the left leg with a load of 30% BW
Group 1 = intact cranial cruciate ligament (CCL); group 2 = transected CCL; group 3a = Mini TightRope; group 3b = fabellotibial suture
The test of within-subject effects showed a significant effect of load (f = 25.940; P <0.05), condition (f = 36.989; P <0.05) and load and condition combined (f = 7.951; P <0.05) (Table 6).
Discussion
The current study showed that the fabellotibial suture, as well as Mini TightRope, neutralised excessive cranial tibial thrust in cats that underwent experimental CCLT. However, we were unable to prove that the Mini TightRope technique is associated with less external rotation than standard fabellotibial suture; data analysis showed no significant differences between the two techniques.
With regard to craniocaudal cruciate-related instability, Kneifel et al, 14 who used the limb-press model previously, proved that monofilament nylon prostheses show greater stability than 0.5 cm wide strips of fascia lata applied intracapsularly. For the evaluation of cranial tibial translation, radiographs were used because superimposition of the spring mechanism’s metal components made it impossible to evaluate craniocaudal projections. 15 We decided to add another diagnostic tool to our model to evaluate mediolateral movements. Therefore, our study is the first to combine radiographic assessment with microscribe digitisation to evaluate the efficiency of the two techniques using a custom-made limb press for cats. A biomechanical study on unpaired pelvic hindlimbs of eight dogs, 18 in which microscribe digitisers were used to evaluate the effects of tibial plateau levelling osteotomy on three-dimensional kinematics in CCL-deficient stifles, reported no significant differences in three-dimensional femorotibial alignment between normal and TPLO-treated stifles. 18
Microscribe digitisers are useful tools for measuring three-dimensional kinematics of the stifle in a limb-press model because they can detect cranial or cranioproximal movements, as well as mediolateral movements of the tibia. In our model we used different test points for two-dimensional (radiographic) and three-dimensional (microscribe digitisation) assessment. The use of different test points made it impossible to compare the two methods directly. We used different test points to show the reproducibility of the test point records. For the microscribe digitiser, we selected easily identifiable and reproducible test points. Because the microscribe digitiser has a thin tip on its distal end, we had to prove that we recorded the exact test points in each leg and under each condition. The test point X2 used for the distance measurement on radiographs was defined as the centre of a circle that was superimposed over the caudal contour of the femoral condyles. On radiographs, this centre is easy to define, but it was impossible to mark this test point on the limb mounted into the limb press. Therefore, we had to seek microscribe test points that could yield similar results but that are easy to record on the limbs.Even if the radiographic assessment and microscribe digitisation cannot be compared directly, it is clear that both tools facilitated the detection of the cranial tibial thrust after CCLT (elongation of X1–X2 and D2 in group 2 measured in radiographs and calculated from microscribe coordinates, respectively). However, D2 did not show significant changes. We noted a mild but statistically insignificant elongation after CCLT. Either there is no significant difference or the system with the test points we have chosen is not suitable for this specific evaluation.On the basis of our results corresponding to the mediolateral plane, a shortening of D1 after CCLT is expected because of a medial rotation of the tibia. As it is a three-dimensional measurement, these effects are compounded with a lengthening because of cranial tibial thrust. Therefore, the distance is not significantly shortened or slightly lengthened. To account for that result, in future studies, researchers should assess more test points on different locations that are positioned further away from each other on the tibia and femur to obtain more specific results in the craniocaudal and mediolateral planes.
Recent studies show the importance of evaluating the positioning of different suture materials. However, because previous studies performed only radiographic evaluations, in future studies, it would be interesting to investigate the three-dimensional kinematics of CCL-deficient stifles fixed with bone anchors using microscribe digitising systems and the rotational stability in a craniocaudal plane.
In our study we compared the standard fabellotibial suture with Mini TightRope fixation. We decided to tie our sutures with a 20 N load to produce favourable biomechanical stabilisation of CCL-related stifle instability directly after surgery. 14 The fabellotibial suture has been previously tested in several biomechanical5,14 and clinical studies.2,7 To our knowledge, none of the studies evaluated the Mini TightRope for CCL fixation in cats and dogs; however, some studies evaluated the efficiency of TightRope for the extracapsular fixation of CCL-deficient stifles in dogs.6–8
Our study was limited by the fact that we used a three-dimensional biomechanical model that mimicked in vivo conditions. Therefore, further clinical studies must be performed to evaluate the techniques we used for CCLT in vivo. For this purpose, biplanar fluoroscopy, which has already been used in dogs, should be used. 19 Furthermore, microscribe digitisers are limited by the range of motion. In our study, we easily reached all our test points; however, in a better set-up when the test points are >30 cm away from the microscribe origin, it is impossible to record the whole data set. Furthermore, a slight displacement of the digitiser during recording leads to a completely changed coordinate set. If the microscribe digitiser is displaced during one test cycle, the cycle must be started again from the beginning. For further studies, additional diagnostic tools such as camera systems may be useful for the detection of three-dimensional kinematics.
For loading our specimens, we used 10% and 30% BWs of each cat. As we could not create a scenario with no load on the limbs, 10% BW served as a compromise for a low value. The load of 30% BW was used to mimic the load in normal gait. Nevertheless, these are not the loads that would be involved when cats jump. Consequently, with this set-up, our repair techniques were not tested under such high-stress or high-load situations as jumping or falling.
Conclusions
Both the techniques used in this in vitro study are suitable for CCL repair in cats. Lateral fabellotibial suture, as well as Mini TightRope tightened at a 20 N load, led to biomechanical stability after CCLT. Contrary to our assumption, Mini TightRope fixation did not cause less external rotation than the fabellotibial suture. In general, there were no significant differences between the two techniques in a mediolateral plane. The current study is the first to combine a feline custom-made limb press with radiographs and a microscribe digitiser. Further studies are planned to improve the set-up, evaluate different techniques for CCL repair and add a three-dimensional camera system to obtain specific three-dimensional data.
Supplemental Material
Supplemental Material
Cadaveric specimen
Supplemental Material
Supplemental Material
Custom-made limb-press model and patellar tendon load termination
Supplemental Material
Supplemental Material
Test points and reference points
Supplemental Material
Supplemental Material
CT scan and visualisation of bone displacements during limb-press experiments
Supplemental Material
Supplemental Material
Distances and angles
Footnotes
Acknowledgements
Supplementary material
The following files are available online:
File 1: Cadaveric specimen.
File 2: Custom-made limb-press model and patellar tendon load termination.
File 3: Test points and reference points.
File 4: CT scan and visualisation of bone displacements during limb-press experiments.
File 5: Distances and angles.
Conflict of interest
Eva Schnabl-Feichter is a consultant for Arthrex GmbH, Munich, Germany.
Funding
This work was supported by Arthrex GmbH, Munich, Germany, who provided the implants.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognised high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee was therefore not necessarily required.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). For any animals or humans individually identifiable within this publication, informed consent (either verbal or written) for their use in the publication was obtained from the people involved.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.