
Abstract
Objectives
Brachycephalic obstructive airway syndrome (BOAS) is a common cause of upper airway obstruction in dogs, but is appreciated less commonly in cats. Of the components of BOAS, stenotic nares appear to play a major role in cats. However, the axial deviation of the alar wing, a common cause of nasal obstruction in dogs, is typically not present. We report a series of brachycephalic cats with a ventral nasal obstruction resulting from redundant skin along the floor of the nares. In these cats, surgical techniques developed for dogs were felt to be suboptimal. Our aim is to describe a novel surgical procedure designed specifically to surgically correct stenotic nares in cats with an obstructive fold of skin ventral to the nostril.
Methods
Five brachycephalic cats presenting for clinical signs of stenotic nares underwent surgical repair. In each case, a resection of the skin fold followed by a bilateral single pedicle advancement flap technique was performed. Postoperative outcomes were obtained by contacting owners by telephone.
Results
All cats had positive outcomes, resulting in immediate reduction of the nasal fold and opening of the nares. Owners noted resolution of stertor and no episodes of respiratory distress. No surgical complications were reported.
Conclusions and relevance
In brachycephalic cats, the ventral skin fold may be a significant contributor to stenotic nares, unlike dogs. Resection of the skin fold, followed by bilateral single pedicle advancement flaps is a novel technique and appeared to be successful for treating stenotic nares in this series of brachycephalic cats.
Keywords
Introduction
Brachycephalic obstructive airway syndrome (BOAS) is a commonly observed cause of inspiratory obstruction in brachycephalic dogs, but occurs less commonly in cats. In dogs, the major anatomic abnormalities leading to airway obstruction include stenotic nares, tracheal hypoplasia, soft palate elongation, everted laryngeal saccules and laryngeal collapse.1–3 These abnormalities result in variable amounts of respiratory distress, stertor/stridor, exercise intolerance, and other craniofacial and gastrointestinal health problems.3–5 In brachycephalic cats, particularly Persian cats and exotic breeds, brachycephalic abnormalities have been seen but few clinical reports have been published.4,6
In 2012, Corgozihno et al 6 documented a soft palate elongation in a Persian cat presenting with recurrent episodes of respiratory distress and pulmonary edema. This was the first known report of an elongated soft palate in a brachycephalic cat causing an upper airway obstruction. Airway obstructions of this nature are common in brachycephalic dogs, but not readily identified in cats.
Brachycephalic cats occasionally present with stenotic nares. Anecdotally, these cats commonly do not have other components of brachycephalic airway disease observed in dogs. In the study reported here, we noted distinct visual and anatomical differences in stenotic nares in this series of cats compared with what is typically observed in dogs. Dogs are primarily affected by stenotic nares owing to an axial deviation of their alar folds. The cats reported here had a ventral obstruction of the nares secondary to redundant skin at the junction of the ventral floor of the nares and haired skin of the lip, and less significant axial deviation of the alar wings. The purpose of this paper is to describe a novel surgical procedure to account for potential feline-specific anatomical differences. We hypothesized that a resection of the ventral nasal fold, followed by bilateral single pedicle advancement flaps, will effectively relieve clinical signs of airway obstruction associated with stenotic nares in this series of brachycephalic cats.
Materials and methods
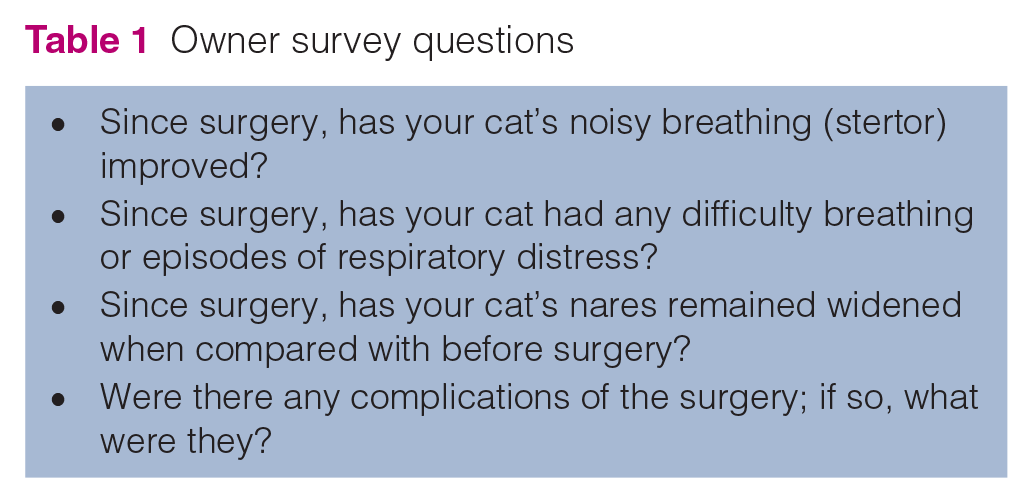
Medical records were reviewed between January 2009 and September 2019 for brachycephalic cats with a diagnosis of stenotic nares or BOAS that were undergoing this surgical technique. Five cats meeting these criteria were identified. Results of physical examinations, preoperative bloodwork, preoperative imaging and laryngeal examinations were recorded. All five cats underwent the surgical approach for stenotic nares described in this report, involving a resection of the ventral nasal skin fold followed by bilateral single pedicle advancement flaps. Postoperatively, owners were surveyed regarding surgical outcomes and clinical improvement in respiratory noise. Owner survey questions are provided in Table 1.
Owner survey questions
Description of technique
All five cats were preoxygenated prior to induction of anesthesia. Premedication protocols included an opioid agonist with or without a benzodiazepine. Four cats received midazolam (0.1–0.3 mg/kg IV) with either butorphanol (0.3–0.4 mg/kg IV/IM), buprenorphine (0.01 mg/kg IV) or oxymorphone (0.05 mg/kg IV). One cat received solely hydromorphone (0.1 mg/kg IV). Four cats were induced with propofol (4–6 mg/kg IV to effect) and one cat was induced with alfaxalone (3 mg/kg IV). All cats were maintained on an inhalant anesthetic and oxygen. During induction, a laryngeal examination was performed on three cats to evaluate for soft palate elongation or the presence of everted laryngeal saccules. Once intubated, an area ventrolateral to the nares was clipped and routinely prepared for surgery. The cats were placed in sternal recumbency (Figure 1a).A single pedicle advancement flap was created bilaterally using a number 11 scalpel blade (Figure 1b). The long axis of the flap was oriented in a rostrocaudal orientation. The base of the flap was just within the nasal cavity and extended rostrally to the haired skin of the lip (Figure 1b). The flap width encompassed the entire ventral floor of the nares. The excessive ventral nasal fold was excised en bloc at the entrance to the nares (Figure 1c). The flap was advanced and closed in a single layer with a simple interrupted closure using 5-0, monofilament suture (Figure 1d). The process was repeated on the other side (Figure 1e; Figure 2).

(a) Brachycephalic cat with stenotic nares secondary to ventral nasal obstruction. (b) Incision for advancement flap, extending into the nasal mucosa. (c) Undermining of flap and excision of redundant skin at entrance to nares. (d) Advancement of mucosal flap to cover defect, closure with a simple interrupted suture pattern. (e) Completion of single pedicle advancement flap, repeat on opposite side. Illustrated by Kip Carter, ©UGA 2019

(a) Brachycephalic cat with stenotic nares secondary to ventral nasal obstruction via redundant skin, preoperatively. (b) After undergoing the bilateral, single pedicle advancement flaps surgical technique
Postoperative considerations
All cats recovered in an oxygen cage. Cats received postoperative analgesia for 3 days. Analgesia varied between non-steroidal anti-inflammatory drugs (meloxicam or robenacoxib) and a partial mu-opioid agonist (buprenorphine), or a combination of the two. One cat received oral meloxicam (0.1 mg/kg q24h) and oral transmucosal buprenorphine (0.01 mg/kg q8h). Two cats received solely oral transmucosal buprenorphine (0.01–0.03 mg/kg q8h) and one cat received solely oral robenacoxib (1.7 mg/kg q24h). One cat received oral gabapentin (10 mg/kg q12h). An Elizabethan collar was recommended for 10–14 days after surgery, until the incision site was able to be reassessed and the skin sutures removed, if required.
Results
Three cats were seen at the University of Georgia Veterinary Teaching Hospital, one cat was seen at Texas A&M University Veterinary Teaching Hospital and one cat was seen at Westvet Animal Specialty Center.Case 1, an 8-year-old castrated male Persian, presented for evaluation of stenotic nares following intermittent episodes of respiratory distress and persistent stertor. Case 2, a 9-year-old spayed female Scottish Fold, presented for progressive stertor and non-productive sneezing. Case 3, a 7-month-old castrated male Persian, and case 4, a 2-year-old spayed female Persian, similarly presented for evaluation of stertor since birth and intermittent sneezing with nasal discharge. Case 5, an 8-month-old male Persian, presented for marked stertor and exercise intolerance.
Case 2’s preoperative blood work revealed mild hemoconcentration (red blood cells 10.47 ×106/μl [reference interval (RI) 4.9–9.8 ×106/μl], total protein 7.5 g/dl [RI 5.5–7.2 g/dl]), moderate hypercholesterolemia (269 mg/ dl [RI 76–152 mg/dl]) and mild hyperglycemia (124 mg/dl [RI 54–114 mg/dl]). Preoperative blood work, thoracic radiographs and urinalysis for the remaining cases were within normal limits.
Of the three cats undergoing a laryngeal examination prior to intubation, none had evidence of an elongated soft palate. The single advancement flap technique was successfully performed in all five cats. One cat had a wedge alaplasty performed in addition to the flap. The flaps were closed with a variety of sutures including poliglecaprone 25, polydioxanone, polyglactin 910 and nylon. Immediate results included reduction of the ventral nasal fold and opening of the nares. Healing of the surgical site was completed after 2 weeks in all cats. Success of the procedure was based on reduction of the ventral nasal fold, opening of the nares and appropriate healing of the advancement flap. Four of five cats were available for follow-up. Of those available, all four owners reported a reduction in stertorous breathing with no episodes of respiratory distress since surgery. All noted the nares remained open following surgery; no surgical complications were reported. Postoperatively, follow-up times were 9 years, 5 years, 7 months, and 3 weeks, for cases 1, 2, 4 and 5, respectively.
Discussion
In this study, the most common reason for surgical correction involved upper respiratory signs, primarily stertorous breathing, followed by sneezing. In 2016, Farnworth et al 4 surveyed 239 owners regarding their cat’s respiratory noise, activity levels and physical characteristics. Owner-submitted pictures of cats were used to calculate a nose position and muzzle length ratio. A respiratory score (1–4) was assigned to each cat, ranging from quiet (1) to continuous snoring/wheezing (4). Reduction of the nose position and muzzle length ratio were significantly associated with exercise intolerance and higher respiratory scores. These clinical signs were observed most commonly in Persian breeds and identified in 4/5 cats in our study.
Although not documented in our cases, cats with chronic upper respiratory obstruction may also present for gastrointestinal signs. In a recent report on cats with hiatal hernia, a condition commonly associated with upper airway obstruction in dogs, 9/31 cats had evidence of upper airway obstruction and, of those, three were brachycephalic cats. 5 If present, surgical correction of stenotic nares may play a critical role in managing that condition.
Resection of the skin fold followed by bilateral single advancement flaps is a novel and potentially useful technique for treating stenotic nares in cats. This technique allows for direct reduction of the ventral nasal fold and is effective at opening the nares. While few cases are reported here, it may be that this condition is underappreciated by veterinarians and owners of brachycephalic cats. This simple technique may reduce resistance to airflow in cats and, by doing so, may improve the quality of life of these cats.
A major limitation to this study is the small number of cases available. However, long-term outcomes are promising in most of these cats, suggesting that this technique may have potential for use in a larger number of clinically affected cats. In addition to the described technique, one cat underwent a wedge alaplasty, which is the standard surgical treatment for this condition.1,3 Future studies are warranted to objectively determine the effect of this procedure on airway resistance compared with traditional techniques. Finally, not all cats had documentation of a laryngeal examination prior to surgery, which highlights an important limitation to retrospective studies in general. Patients with evidence of upper airway disease or BOAS should undergo a complete diagnostic work-up prior to surgical repair, including thoracic radiographs and an upper airway examination under light anesthesia to allow for direct visualization of the oral cavity, pharynx and larynx. 3 Tracheoscopy may also be indicated in some cases. 7 Regardless, in the four cats with long-term follow-up following this procedure, all had resolution of clinical signs of upper respiratory obstruction. This suggests a significant component of an upper airway obstruction was related to the nares in this small population.
Conclusions
This study describes a novel technique for the treatment of stenotic nares in cats. At this point, it is premature to recommend this procedure in all clinically affected cats with BOAS. Clinicians should critically evaluate each cat’s nasal structure and be aware that stenotic nares and upper airway obstruction may arise from a ventral skin fold, a lesion not observed in dogs with BOAS.
Footnotes
Author note
This work was presented as an abstract at the Steeve Giguére Science of Veterinary Medicine Symposium, Athens, GA, 2019.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (owned or unowned), and followed established internationally recognized high standards (‘best practice’) of individual veterinary clinical patient care. Ethical approval from a committee was therefore not necessarily required.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work for the procedure(s) undertaken. For any animals or humans individually identifiable within this publication, informed consent for their use in the publication (verbal or written) was obtained from the people involved.