
Abstract
Practical relevance:
Abdominal ultrasound plays a vital role in the diagnostic work-up of many cats presenting to general and specialist practitioners. B-mode ultrasonography is likely the most widely used modality for imaging the gastrointestinal (GI) tract in cats and it can help in the diagnosis of GI masses, foreign bodies and disorders of the ileocaecocolic junction.
Clinical challenges:
Despite ultrasonography being a commonly used modality, many practitioners are not comfortable performing an ultrasound examination or interpreting the resulting images. Even differentiating between normal variations and pathological changes can be challenging for all but the most experienced. For example, while for inflammatory conditions of the feline GI tract changes are frequently identified on ultrasound, there may occasionally be no changes to the appearance of the intestine; hence a ‘normal’ ultrasound does not exclude the possibility of inflammatory disease.
Aim:
This review, part of an occasional series on feline abdominal ultrasonography, describes the appearance of a range of conditions that affect the feline GI tract; the normal GI tract is addressed in an accompanying article in this issue of JFMS. Aimed at general practitioners who wish to improve their knowledge and confidence in feline abdominal ultrasound, this review is accompanied by high-resolution images and videos available online as supplementary material.
Equipment:
Ultrasound facilities are readily available to most practitioners, although use of ultrasonography as a diagnostic tool is highly dependent on operator experience.
Evidence base:
Information provided in this article is drawn from the published literature and the author’s own clinical experience.
Gastrointestinal wall thickening: diffuse vs focal thickening
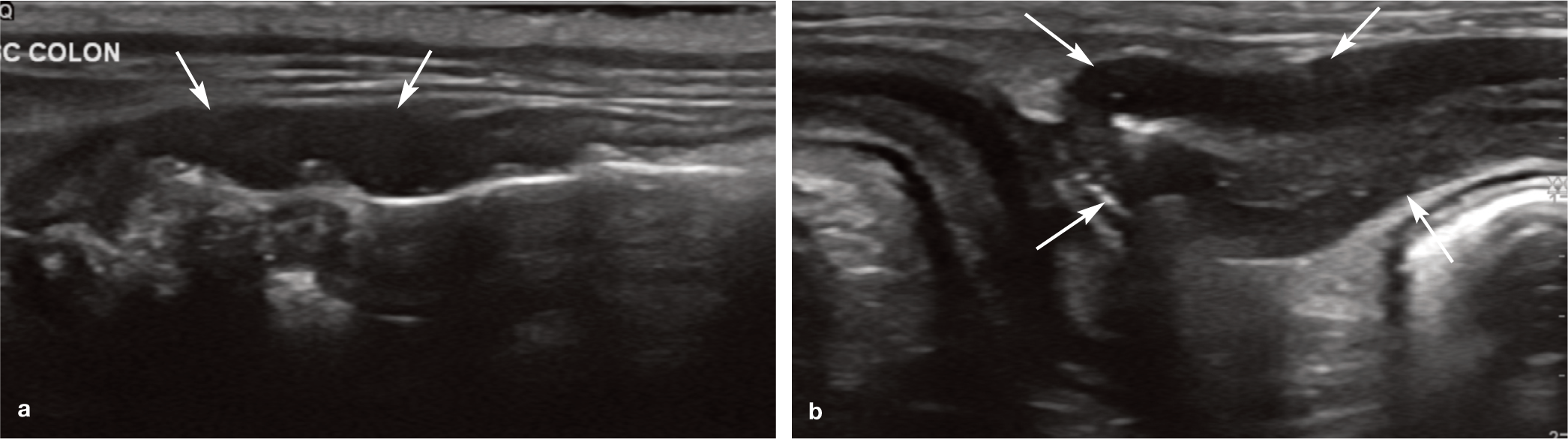
Inflammatory conditions of the feline gastrointestinal (GI) tract may occasionally result in no changes to the appearance of the intestine on ultrasound and therefore a ‘normal’ ultrasound examination does not exclude the possibility of inflammatory disease. However, changes are frequently present and typically take the form of mild diffuse thickening of the intestinal wall with preservation of layering and/or thicken ing of individual wall layers. 1 Hypoechoic nodules 1–3 mm in diameter have been reported in the submucosa of the colonic wall that are thought to represent reactive intraparietal lymphoid follicles and may indicate the presence of colonic inflammatory disease (Figure l). 2

Hypoechoic nodules (arrow), thought to represent lymphoid follicles, are visible within the submucosa of the colonic wall


The presence of one or more mass lesions within the GI tract (characterised by focal regions of moderate to marked wall thickening), associated with partial or complete loss of layering, is suggestive of neoplasia. 3 Particularly severe inflammation can, on occasion, also produce loss of layering, although this is much less common (Figure 2); very rarely, thickening of the bowel wall may be associated with intestinal infarction. 4 In the latter condition, prominence of the mucosa and submucosa, followed in the later stages by complete loss of layering, may be observed. 4
(a) Moderate thickening and loss of layering of a portion of the ascending colonic wall (arrows) in a 12-year-old male neutered domestic shorthair cat. A more normal appearance resumes in the colonic wall on the right, with which it is continuous. The final diagnosis based on histopathology was locally extensive lymphoplasmacytic colitis. (b) Ultrasound image from a 12-year-old male neutered Tonkinese cat that was presented with a chronic history of vomiting, diarrhoea and weight loss despite a good appetite. The wall of the jejunal loop (arrows) in the upper right portion of the image is moderately thickened with loss of normal layering. Although not shown here, there was diffuse selective thickening of the muscularis layer affecting the remainder of the small intestine. The final diagnosis was inflammatory bowel disease
Selective thickening of the muscularis
Diffuse circumferential thickening of the muscularis layer of the small intestine with preservation of wall layering and the absence of mass formation has been reported in cats with eosinophilic and, less commonly, lymphocytic enteritis and low-grade (small-cell) lymphoma (Figure 3).5–7 Thickening of the muscularis has been defined by the authors of one publication as a muscularis layer that exceeds half the thickness of the submucosal layer. 6 As mentioned in the accompanying article on the normal GI tract, however, the results of a later study suggest that the muscularis layer is normally equal to, or thicker than, the width of the submucosal layer in the stomach, duodenum, jejunum and ileum. 8 The authors of the second study suggest instead that the thickness of the muscularis layer may be compared with the diameter of the aorta, and report mean ratios of 0.079, 0.087 and 0.14 for the duodenum, jejunum and ileum, respectively, although specific upper limit cut-off values were not offered. 8 It is important to note that histopathology of the intestine was not performed and, therefore, it is not possible to rule out subclinical disease in the cats included in this study.

(a–d) Examples of selective thickening of the muscularis layer in three different cats. (a) Ultrasound image showing severe muscularis thickening of the ileocolic junction in a 13-year-old female neutered domestic shorthair cat presenting with anorexia and lethargy. The final diagnosis was inflammatory bowel disease, concurrent with bacterial cholangitis and pancreatitis. (b) Several loops of jejunum displaying uniform thickening of the muscularis layer in a 12-year-old male neutered Birman. Final histopathological diagnosis was lymphocytic enteritis. Images (c) and (d) are from a 16-year-old male neutered domestic shorthair cat. Severe thickening of the muscularis layer of several loops of jejunum (c) and of the ileal wall at the ileocolic junction (d) is shown. Two jejunal lymph nodes are visible in the centre of image (c). The owner declined intestinal biopsy. Videos showing marked thickening of the muscularis layer of the jejunum and ileum are available as supplementary material
Diffuse selective thickening of the muscularis layer is reported more commonly in cats with low-grade lymphoma than inflammatory bowel disease (IBD), probably owing to the higher prevalence of the former. 7 It should be noted that this statement is derived from a study in which the cats diagnosed with lymphoma were significantly older than those with IBD, which may have affected the results. 6 In cats with lymphoma, overall wall thickness is usually normal or increased and wall layering is typically preserved. 9 In a study of cats with low-grade lymphoma, the mean wall thickness was 4.3 mm (median 4.5 mm, range 3.4–5 mm). 9 Mesenteric lymphadenopathy is also common. 10 In a further study, 22/27 (81%) cats with low-grade lymphoma had evidence of intestinal thickening on ultra-sound. 11 Focal intestinal mass formation, intussusception and increased mucosal echo-genicity have also occassionally been observed in cats with low-grade lymphoma.9,12
Lymphadenopathy can occur with both IBD and lymphoma, although any changes present are often more marked with lymphoma than with enteritis.1,6,13 Furthermore, normal intestinal wall thickness and an absence of mesenteric lymph node changes do not exclude the possibility of low-grade lymphoma. 14 Therefore, since there is substantial overlap in the appearance of both disease processes on ultrasound, further tests including full thickness surgical biopsy, immuno-histochemistry and clonality analysis should be considered. 7
Selective muscularis thickening of the intestine proximal to a stenosis caused by alimentary lymphoma in one cat and an intestinal foreign body in a second cat have also been reported, and in both cases was believed to be due to smooth muscle hypertrophy. 15 Mast cell tumours and histoplasmosis have likewise been reported to cause selective thickening of the muscularis of the small intestine in cats.16,17 Focal thickening of a jejunal loop with loss of layering and peritoneal effusion were additional findings in association with histoplasmosis. 17 An unusual case involving severe diffuse thickening and increased echogenicity of the muscularis layer of the stomach has been reported in a cat due to eosinophilic fibrosing gastritis. 18 The authors of that study postulated that toxoplasmosis infection may have been the underlying cause. 18
Focal gastrointestinal masses
Despite the descriptions below of the typical appearance of various intestinal lesions, significant overlap exists. This lack of specificity means that the ultrasonographic appearance cannot be regarded as pathognomonic for a particular tumour type, or even for neoplasia vs benign disease, and thus sampling is required for a definitive diagnosis.
Neoplastic gastrointestinal lesions
Focal GI masses are usually neoplastic, although exceptions can occur (see below). It is generally agreed that lymphoma is the most common intestinal tumour and adenocarcinoma is the most common non-lymphoid tumour, followed by mast cell tumours,14,19–24 although a study by Rivers et al 19 suggests that adenocarcinoma may be the most common tumour. The Siamese breed and increasing age (particularly cats aged 10–14 years), equates to an increased risk.23,24 Lymphoma is also the most common tumour of the feline stomach; conversely, and in contrast to the situation in dogs, gastric adenocarcinoma is very rare. 25
Lymphoma can present as solitary or multiple intestinal masses or, as previously mentioned, a diffuse thickening of the (small intestinal) muscularis layer with otherwise normal wall layering. Masses owing to lymphoma are more likely to be intermediate or high grade in nature, and most commonly present on ultrasound as transmural, hypoechoic, circumferential thickenings of the GI wall, associated with loss of normal wall layering and reduced motility of the affected intestinal segment (Figure 4).14,26–28 The mass may be symmetrical or asymmetrical, and ulceration may or may not be present.26,27 Ultrasonographic evidence of extraintestinal involvement, and especially regional lymphadenopathy, is common,28–30 and often accounts for the mass effect detected during abdominal palpation.9,26,27 Mesenteric involvement due to direct extension from a lymphomatous colonic mass has also been described and, on ultrasound, resulted in the appearance of small hypoechoic nodules within the adjacent mesenteric fat. 28
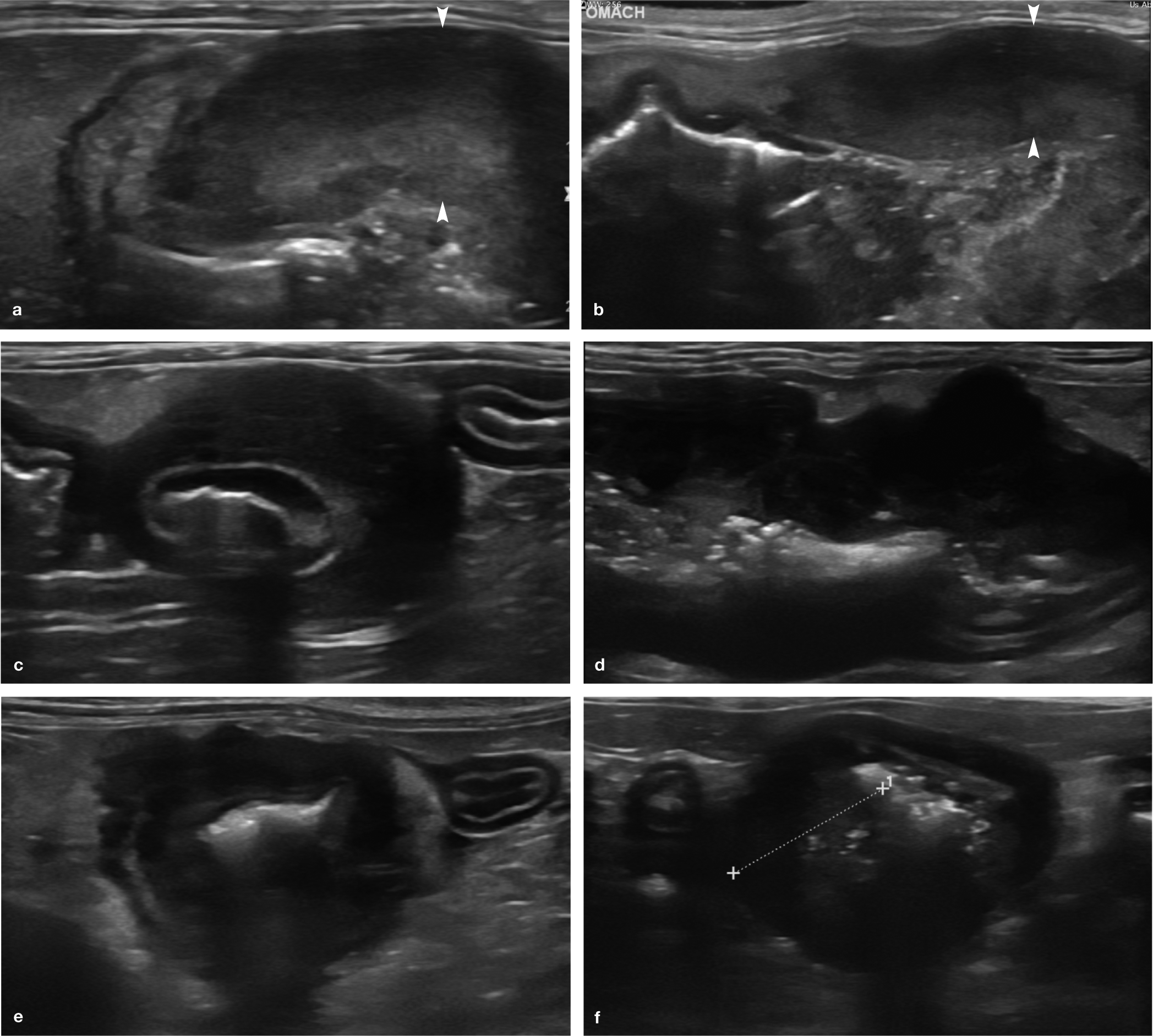
Examples of gastrointestinal (GI) lymphoma. (a,b) GI masses in two adult cats due to lymphoma. In both cases there is a focal marked thickening of the gastric wall (arrowheads), associated with complete loss of layering and an overall hypoechoic echogenicity. (c) Marked focal eccentric thickening of the muscularis layer of a jejunal loop in a 5-year-old male neutered domestic shorthair cat. Diffuse mild to moderate thickening of the muscularis layer was also noted throughout the jejunum. The final diagnosis of lymphoma was based on fine-needle aspiration of the mass. (d) Marked circumferential thickening of the jejunal wall owing to lymphoma. Note the complete loss of layering in the affected portion of bowel wall. Hyperechoic material centrally represents intraluminal gas and ingesta. (e) Marked focal circumferential thickening of the wall of a loop of jejunum in transverse orientation owing to lymphoma in a 7-year-old male neutered domestic shorthair cat with a history of weight loss, inappetence and lethargy, and a palpable abdominal mass. There is almost a complete loss of layering. The centrally located region of hyperechogenicity associated with distal acoustic shadowing represents gas within the intestinal lumen. (f) Eccentrically located mass (located between the measuring calipers) in the ileum of a 14-year-old male neutered domestic shorthair cat. Concurrent ultrasonographic findings included diffuse thickening of the muscularis layer and moderate enlargement of the jejunal and ileocolic lymph nodes. The final diagnosis was lymphoma. A video showing a focal gastric mass due to confirmed lymphoma in a cat is available as supplementary material
The ultrasonographic appearance of adenocarcinomas of the feline GI tract has similarly been reported. 19 Adenocarcinomas typically present as solitary intestinal masses. 31 Circumferential segmental wall thickening characterised by transmural loss of normal wall layering is a feature that has been described in cats with GI adenocarcinoma. 19 These tumours may be symmetrical or asymmetrical and can have a similar appearance to GI lymphoma. 19 One reported difference is that intestinal adenocarcinoma is more likely to be of mixed echogenicity compared with lymphoma, which is more commonly associated with a uniformly hypoechoic intestinal wall, although definitive diagnosis will always rely on tissue sampling. 19 Intestinal tumours and, in particular, adenocarcinomas can cause intestinal obstruction and fluid may accumulate within the intestine proximal to the lesion owing to localised ileus. 32
Mast cell tumours have been reported to present as focal masses in the duodenum or jejunum, at the ileocaecocolic junction (ICCJ) and in the colon or, much more rarely, as diffuse intestinal wall thickening.16,33 They are most commonly described as a focal hypo-echoic thickening of the intestinal wall associated with loss of normal layering and may be either non-circumferential and eccentric or circumferential, asymmetric and eccentric.16,33
Sporadic reports of unusual GI tumours in cats include a gastric smooth muscle hamartoma in an 11-year-old cat, which appeared on ultrasound as a 2 cm diameter, poorly vascular, hyperechoic mass within the gastric wall in the region of the cardia. 34 Intestinal haemangiosarcoma has been reported in three domestic shorthair cats variously affecting the colon, small intestine, ICCJ and rectum, and may cause luminal narrowing. 35 Finally, fibrosarcoma and leiomyosarcoma of the feline GI tract have also been reported, albeit rarely. 36 The latter presented ultrasonographically as a comma-shaped, heterogeneous mass in the intestine of a 13-year-old cat. 37
Non-malignant intestinal masses
Although less common, intestinal masses can also result from benign or non-neoplastic lesions such as granulomas associated with feline infectious peritonitis (FIP), feline gastrointestinal eosinophilic sclerosing fibroplasia (FGESF) and duodenal polyps.38,39
In a recent case report, severe jejunal (up to 9 mm) and ileocolic intestinal wall thickening with loss of layering were described in association with FIP in a 9-month-old entire male domestic longhair indoor cat (Figure 5). Following an enterectomy to remove the affected segments of intestine, histopathology confirmed the presence of severe pyogranulomatous enteritis with vasculitis. 40

(a,b) Ultrasound images from a 9-month-old entire male domestic longhair cat infected with feline coronavirus. The jejunal wall (between the measuring calipers) is markedly thickened with loss of layering. Severe pyogranulomatous enteritis with vasculitis consistent with feline infectious peritonitis was subsequently demonstrated on histopathology. Images courtesy of Maria A Ernandes, Ambulatorio Veterinario Brollo, Fidenza (Parma), Italy
FGESF is an inflammatory condition that primarily affects middle-aged cats and it has been suggested that Ragdolls may be over-represented. 41 FGESF is an important differential for an intestinal mass in the cat and can mimic neoplasia (Figure 6). 42 In a retrospective study of 25 cats with FGESF, the condition presented most commonly as an ulcerated intramural mass with loss of layering at either the pyloric sphincter or ICCJ junction, or, less commonly, within the duodenum, jejunum or colon. 43 Hyperechoic areas within FGESF lesions on ultrasound have been described and are thought to represent fibrotic regions. 44 An extramural FGESF lesion has more recently been described in a 4-year-old male neutered cat. The lesion originated within the soft tissues of the retroperitoneum and caused ventral displacement and narrowing of the descending colon, resulting in obstipation. On ultrasound, the mass was lobulated and heterogeneous with multiple hypoechoic to anechoic centrally located regions. Colour Doppler revealed moderate vascularity within the more peripheral regions of the mass. 45 Mild ascites and hyperechoic mesentery have also been reported on ultrasound of a cat with FGESF limited to mesentery. 46

Ultrasound images of suspected feline gastrointestinal eosinophilic sclerosing fibroplasia lesions in a 13-year-old female neutered domestic shorthair cat presenting with a history of chronic haematochezia and weight loss. Both masses are heterogeneous and completely efface wall layering. The first (a) was at the ileocolic junction and the second (b) within the wall of the mid-descending colon. There was also evidence of ileocolic lymphadenopathy. Cytology following fine-needle aspiration revealed a predominantly eosinophilic inflammation. While this could also be associated with parasitism and neoplasia (such as mast cell tumour and lymphoma), there was no direct evidence to support this in the examined smears. The owner declined an exploratory laparotomy for full-thickness gastrointestinal biopsies
Intracellular bacteria are also frequently identified in FGESF lesions on histopathology, although it is uncertain whether the bacteria are the cause or a result of the condition. It is hypothesised that these bacteria may gain entry to the intestinal wall as a result of damage such as that caused by a penetrating foreign body or ulceration.41,43,44 This may help to explain the predominance of lesions at the pyloric sphincter and ICCJ, where physical forces are usually greatest. 43 In cats with a genetic predisposition to this lesion, a subsequent eosinophilic response mounted against these intramural bacteria may result in the formation of FGESF lesions. 43 Nevertheless, the exact pathogenesis of FGESF remains unclear and food hypersensitivity has also been proposed as a possible cause. 43
Loss of layering within focal intestinal lesions caused by FGESF and associated lymph node enlargement are common findings, explaining why FGESF lesions can so easily be mistaken for neoplasia on ultra-sound. 44 However, unlike most neoplastic lesions, FGESF lesions have been described as feeling ‘hard and gritty’ when fine-needle aspiration or core biopsy are performed. 41
A further differential for a benign intestinal mass is an adenomatous polyp, the ultrasonographic appearance of which has recently been reported at the pyloroduodenal junction in six cats. 47 The typical presentation described was that of a small, echogenic homogeneous nodule projecting into the lumen of either the proximal duodenum or the pyloroduodenal junction. 47 The authors of the study found that the polyps were easily mistaken for ingesta and, while benign, could cause luminal obstruction, GI bleeding and obstruction of the biliary tract. 47 One of the main differentials for a solid duodenal mass in an older cat is primary intestinal neoplasia. However, in 5/6 cats with polyps, duodenal layering was preserved. 47 This is in contrast to neoplastic lesions, which are typically hypoechoic and result in partial or complete loss of wall layering. 39 Furthermore, while duodenal polyps project into the lumen, carcinomas and lymphoma usually affect the entire circumference of the wall and smooth muscle tumours tend to be exophytic. 39 Cats with duodenal polyps were mostly middle-aged to older (mean ± SD age of 9.6 ± 3.5 years), 47 which is similar to a previous report on 18 cats with duodenal polyps. 38 In both studies, acute vomiting was one of the most common clinical signs at presentation, presumably due to partial obstruction of the duodenal lumen.38,47 The prognosis after surgical resection is reported to be excellent. 38
Intussusceptions
An intussusception occurs when one part of the intestine (the intussusceptum) invaginates into the lumen of an adjacent intestinal segment (the intussuscipiens). 48 Any portion of the bowel may be affected but jejunojejunal and enterocolic intussusceptions appear to be the most common types in the cat.49,50
Publications detailing the ultrasonographic appearance of intussusceptions in the cat are sparse but, based on the limited information available, the appearance closely resembles that seen in dogs.37,51 In the transverse plane, an intussusception forms a circular target-like lesion (sometimes referred to as having a ‘bull’s eye’ appearance) owing to the presence of multiple concentric rings that represent the different layers within the adjacent walls of the intussuscipiens and intussusceptum (Figure 7a).37,51 In the longitudinal plane, the appearance is similar and again results from the multiple alternating hypoechoic and hyperechoic parallel lines formed by numerous wall layers. 51 Hyperechoic tissue may be visible within the centre of the lesion, representing mesenteric fat that has been pulled into the intussuscipiens along with the intus-susceptum (Figure 7b). Anechoic areas within the hyperechoic centre represent dilated lymphatics and blood vessels. 51 In chronic cases, the outer intussuscipiens segment can become thickened and hypoechoic, and individual wall layers may become less discernible owing to oedema and compromised blood flow. 37 Mesenteric lymphadenopathy and abdominal effusion have also been identified in cats with intussusceptions. 49

Ultrasonographic appearance of an intussusception in a 13-year-old male neutered domestic shorthair cat. (a) The intussusceptum fills the lumen of the intussuscipiens. (b) Echogenic fat and mesenteric vessels (arrows) have been drawn into the lumen of the intussuscipiens along with the intussusceptum. There is partial disruption to the normal wall layering of the intussuscipiens, most likely owing to oedema of the wall
Since the condition in older cats has been reported to occur in association with IBD, intestinal neoplasia, caecal inversion and the presence of a caecal polyp, the intestine should always be assessed carefully to determine whether additional conditions may be present.49,51–55
Foreign bodies
Linear foreign bodies such as sewing thread, dental floss and string are relatively common in the cat and represent the most frequent type of foreign body seen in this species.56,57 A portion of the foreign material becomes anchored, usually around the base of the tongue or less commonly at the pylorus, while the remainder travels distally into the small intestine. 57 Peristaltic contractions unsuccessfully attempt to transport the foreign body aborally, eventually leading to intestinal plication. 57 If left undetected, complications such as intestinal wall perforation and septic peritonitis can develop. Radiographs can be helpful in the diagnosis and may reveal bunching of small intestinal loops and abnormal ‘crescent’- or ‘teardrop’-shaped intestinal gas bubbles (Figure 8a). 58 Where radiographs are inconclusive or doubt exists, the diagnosis of a linear foreign body can usually be confirmed on ultrasound. 59 Evidence of intestinal plication on ultrasound is strongly suggestive of the presence of a linear foreign body, although definitive diagnosis relies on demonstrating the presence of linear foreign material within the lumen of the plicated intestine (Figure 8b). 59

(a) Cropped abdominal radiograph of a cat with a confirmed linear foreign body. The small intestine is bunched together within the mid-ventral abdomen. Abnormal teardrop- and crescent-shaped intestinal gas bubbles (arrows) are visible. (b) Ultrasound image showing plicated intestine in a 5-month-old male entire domestic shorthair cat that originally presented for further investigation of poor growth and inappetence. The linear foreign body is represented in the image by the thin hyperechoic line (arrows) passing through the centre of the plicated intestine. Subsequent oral examination under sedation revealed the presence of thread encircling the base of the cat’s tongue that extended down the oesophagus. A video showing the ultrasonographic appearance of plicated intestine owing to a linear foreign body (which is also visible) in the 5-month-old kitten in part (b) is available as supplementary material
The term plication describes the folding of intestinal loops such that adjacent loops become stacked in an accordion-like pleated fashion. 60 All layers of the intestinal wall within an affected bowel segment are involved, including the serosa.
As with non-linear foreign bodies, the precise ultrasonographic appearance of a linear foreign body will depend on the degree to which the material transmits or attenuates the ultrasound beam. 59 Typically, however, the foreign material will be represented by an echogenic line of variable diameter, running through the middle of the plicated segment of intestine, and may or may not be associated with distal acoustic shadowing depending on its physical properties. 59 Since linear foreign bodies usually cause only partial obstruction of the intestine, there is often little or no accompanying intestinal dilation. 61
Plication of the intestine should be differentiated from intestinal corrugation, which describes regular, symmetrical undulations of the intestinal wall in the presence of a straight serosa (Figure 9). 39 Intestinal corrugation is a non-specific change and may be associated with enteritis, pancreatitis, peritonitis, neoplasia and ischaemia of the bowel wall. 62
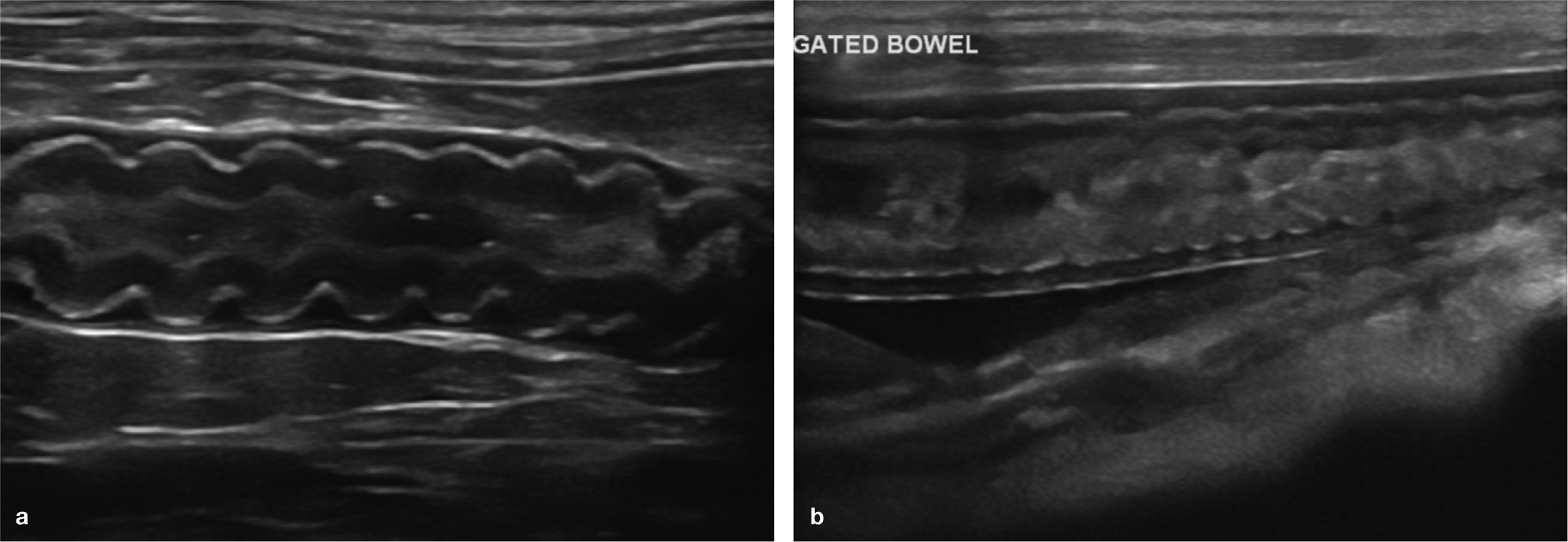
(a,b) Examples of corrugated intestine. In each ultrasound image, note that while the majority of the bowel wall is thrown up into a wave-like formation, the serosal layer remains completely straight
Roundworms can also potentially mimic linear foreign material as they appear on ultrasound as paired parallel hyperechoic lines within the intestinal lumen (Figure 10). 39 They are easily differentiated from linear foreign bodies, however, as they do not cause plication of the intestine, do not usually shadow and movement of live worms can often be observed. 39

Ultrasound image from a 4-year-old male neutered domestic shorthair cat with protein-losing nephropathy. A roundworm is visible in the lumen of a loop of jejunum. Movement of the worm could be appreciated during real-time ultrasound. A large volume of anechoic peritoneal fluid was also present owing to marked hypoalbuminaemia as a result of a protein-losing nephropathy. A video showing the roundworm present within the jejunal loop in this cat is available as supplementary material
Non-linear foreign bodies are occasionally seen in the cat and may be recognised by the presence of an intraluminal structure with a strongly echogenic interface associated with variable strong clean distal acoustic enhancement. The severity and chronicity of the obstruction determines the extent to which the intestine proximal to the foreign material dilates. One of the more common types of foreign body, seen particularly, but not exclusively, in longhaired cats, are tricho-bezoars, also known as hairballs (Figure 11).39,63–66 The typical ultrasonographic appearance is that of a mixed echogenicity cylindrical or spherical mass associated with variable acoustic shadowing, which is largely determined by the size and density of the hairball. 1


Ultrasound image depicting the typical appearance of a non-linear foreign body. The jejunal loop is distended on the left by a structure with a strong echogenic interface and clean distal acoustic shadowing. The intestinal loop towards the right side of the image rapidly resumes a normal diameter distal to the obstructing material. Three empty small intestinal loops are visible in the transverse plane in the upper right corner of the image. The final diagnosis following an exploratory coeliotomy was a trichobezoar
Mucosal fibrosis
A hyperechoic mucosal band paralleling the submucosa has been reported in cats (Figure 12). 69 It was suggested that this band, identified in cats with and without clinical signs of GI disease, represents mucosal fibrosis. 69 The clinical significance of this finding is unknown at the present time.

(a) Ultrasound image of several jejunal loops in a 12-year-old male neutered Birman (same cat as Figure 3b). A thin hyperechoic line (arrow) is visible within the mucosal layer, most clearly seen in the central loop and suspected to represent mucosal fibrosis. (b) A subtle hyperechoic line (arrow) is just visible within the jejunal mucosa in a 6-year-old male neutered domestic shorthair cat. The ultrasound scan was performed to investigate kidney disease and there were no clinical signs present to suggest concurrent intestinal disease
Fibrotic small intestinal stricture
The ultrasonographic and histopathological features of benign fibrotic small intestinal strictures have recently been described in eight cats with chronic intestinal obstruction. 70 The ages of the cats ranged from 2–10 years. Clinical signs included intermittent vomiting, anorexia and severe lethargy. In more advanced cases, projectile, large-volume fluid vomiting or regurgitation was reported and transient diarrhoea was observed in 3/8 cats.
Ultrasonographically, strictures were characterised by a segment of bowel with a non-distensible lumen and were identified in the duodenum (1/8), mid- to distal jejunum (4/8) and proximal ileum (3/8). 70 In all cats, there was evidence of moderate to marked gastric and either generalised or segmental small intestinal distension oral to the stenosis indicative of mechanical bowel obstruction. The length of the stenosed segment varied from 2–50 mm. The intestinal wall at the stricture site was mildly to moderately thickened (range 3–6 mm), with complete or, more commonly, partial loss of layering resulting in a predominantly hypoechoic appearance. Mesentery surrounding the stricture was hyperechoic in 6/8 cases. In some cases, the presence of a kink at the oral aspect of the stricture made identification of the stenotic segment more challenging.
Histopathology revealed transmural pathology, which was characterised by inflammation and marked fibrosis that affected the mucosal layer most severely. 70 Sections from three of the cats enabled the authors to demonstrate that fibrosis was indeed the main contributor to the narrowing of the intestinal lumen. Although the aetiology of the fibrosis in these cats is unknown, infectious agents and/or bowel ischaemia were suggested as potential underlying causes.
Abnormalities at the ileocaecocolic junction
Disorders of the feline ICCJ are relatively common and expected clinical signs might include weight loss, vomiting, dysorexia, diarrhoea and haematochezia. 71 One study describing ultrasonographic abnormalities at the ICCJ in 29 cats, of which 28 had GI signs, reported the presence of enlarged caecal lymph nodes, focal hyperechoic mesenteric fat and focal accumulation of peritoneal fluid in the region of the ICCJ (Figure 13). 72 Ileal and caecal wall thickening were also documented in six and 19 cats, respectively, although there may be substantial overlap in caecal wall thickness between healthy cats and cats with an inflamed caecum (typhlitis).72,73 During follow-up ultrasound examination, four cats with resolution of their GI signs also had resolution of the ultrasonographic abnormalities at the ICCJ, suggesting that such findings may be clinically significant in cats with GI signs. 72
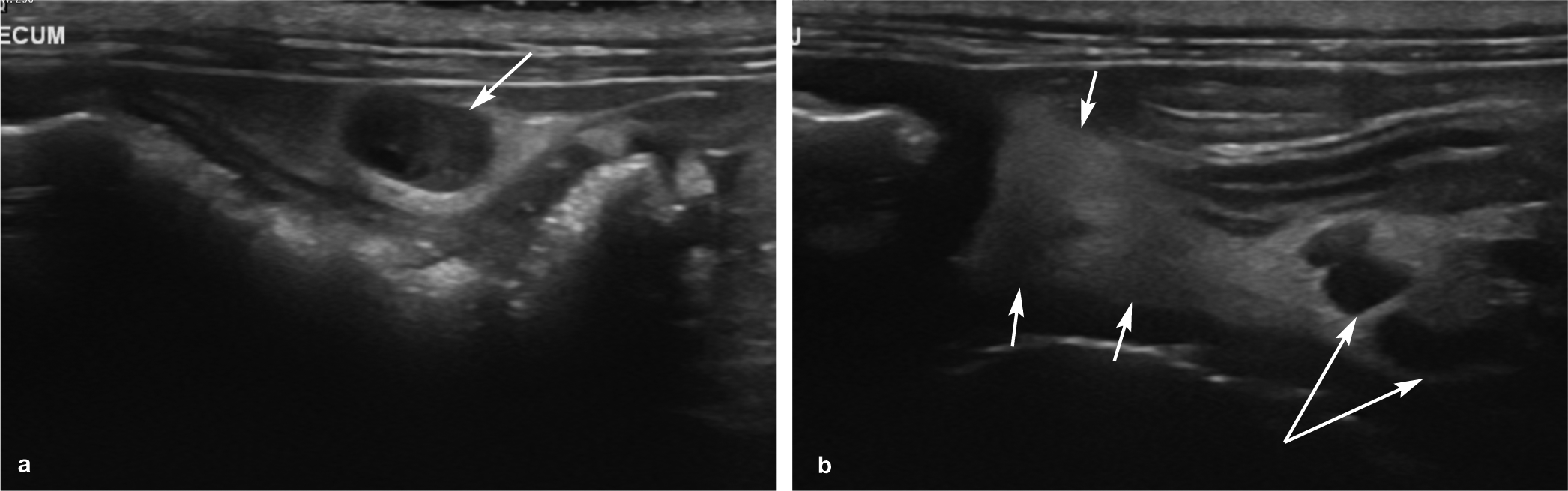
Ultrasound images from a 12-year-old male neutered domestic shorthair cat with confirmed inflammatory bowel disease. (a) Adjacent to the caecum there is an enlarged hypoechoic lymph node (arrow) measuring 7.9 mm in the short axis. Note the abnormal hyperechoic reactive fat surrounding the node. (b) A larger area of hyperechoic reactive fat (short arrows), associated with several reactive lymph nodes (long arrows) measuring up to 4.5 mm in the short axis, is visible at the level of the ileocaecocolic junction (not seen). A video showing an enlarged, hypoechoic lymph node and mildly hyperechoic fat adjacent to the caecum is available as supplementary material
Similar abnormalities were documented in a smaller cohort of 18 cats with chronic clinical signs of caecocolic disease. 73 Loss of caecal wall layering was identified in 7/18 cats, a feature that is typically strongly associated with neoplasia. 73 Of these cats, five underwent biopsy and histopathology. Interestingly, although neoplasia was not identified in any cat, all had evidence of inflammation leading the authors of the study to conclude that loss of caecal wall layering in the cat is suggestive of typhlitis but not necessarily neoplasia. 73 Local steatitis and lymph node size were also found to be unreliable indicators of the severity of inflammation or presence of neoplasia, and an absence of changes in the ICCJ region on ultrasound did not preclude the possibility of disease; as such, biopsy should be considered in cats with chronic clinical signs. 73
Conversely, ultrasound changes at the ICCJ may also occasionally be seen in cats without GI signs. 72 In particular, a proximal caecal follicular layer exceeding 2 mm in thickness at the caecal inlet is suggestive of possible mild subclinical caecal inflammation in asymptomatic cats. 71
Uncommon conditions
Duplication cysts
There are occasional reports documenting the presence of duplication cysts at various locations along the feline GI tract.74–77 Enteric duplications are rare congenital malformations that can arise at any level of the GI tract and result from the duplication of an intestinal segment.78,79 They can be small or large, singular or affect the intestine at multiple levels. 80 Cysts arising at the level of the oesophagus, 75 duodenum, 81 jejunum, 82 ileum, 82 colon 83 and rectum 77 have all been described in the cat. Similar to humans, 79 affected cats are usually presented at a young age, most <2 years old,74,80–82 although the condition is occasionally recognised in older animals, presumably as a result of clinical signs being overlooked and/or enlargement of the cyst as secretions accumulate. 77 Indeed, a search of the human literature reveals occasional reports of patients with enteric duplications and medical histories of chronic constipation (up to 20 years’ duration) prior to a correct diagnosis being made.84–86
In both humans and cats, duplication cysts can cause non-specific GI signs such as vomiting due to partial intestinal obstruction following accumulation of secretions within the cyst80,81,87 and constipation 77 depending on the location of the cyst. In other cases, some cats may be asymptomatic79,82 and the duplication cysts only identified by the presence of a palpable abdominal mass.74,78–80,82
Intestinal duplication cysts are defined by three key characteristics: a close association with the GI tract; a well-developed smooth muscle layer; and an epithelial lining that may differ from that of the adjacent bowel segment.78,82 They also usually share a common blood supply with the adjacent segment of intestine.79,82 They may be recognised ultra-sonographically as fluid-filled spherical or tubular cysts containing sterile fluid; 83 as in humans, they do not usually communicate with the intestinal lumen.74,77–79,82,88 The presence of a distinct hypoechoic layer of smooth muscle within the cyst wall has recently been described as a ‘muscular rim sign’ 74 and is typically continuous with smooth muscle of the adjacent intestinal segment.74,82 The cyst wall thus comprises an inner hyperechoic rim (the mucosa) surrounded by an outer hypoechoic layer (muscular layer), an appearance that is considered to be relatively specific for this condition.74,79
While duplication cysts are benign, malignant transformation of a duodenal duplication cyst has been described in a 15-year-old domestic shorthair cat. 76 Surgical excision is therefore recommended and usually curative, although recurrence has been reported.74,80 Definitive diagnosis requires histopathology, which reveals a normal GI mucosal lining, thereby allowing differentiation from other intra-abdominal cystic lesions. 79 Duplication cysts have also been reported in association with vertebral abnormalities in various species and, accordingly, radiography should be considered in affected animals.77,89,90


Gastrointestinal pneumatosis
The term pneumatosis describes the abnormal accumulation of gas within tissue. 91 The condition has only rarely been reported, with just four cats in the literature with pneumatosis within the gastric,91,92 small65,66 and large 93 intestinal wall.
Reported ultrasonographic findings included diffuse wall thickening (and in one case thinning), loss of or indistinct wall layering and the presence of one or more strong echogenic intramural interfaces within the GI wall associated with a reverberation artefact.91,92,94 All four cats presented with vomiting or regurgitation; two of them were collapsed, one cat showed progressive clinical deterioration and the remaining cat improved following partial gastrectomy and medical management.91–94 The final diagnosis in one cat was severe multifocal necrotising haemorrhagic enterotyphlocolitis secondary to Clostridium difficile toxicity. 94 In another of the cats, gastric wall necrosis and ulceration allowing the entry of gas-producing bacteria was suspected to be the cause of the gastric pneumatosis 91 and, similarly in a third cat, gastric ulceration was suspected to be the underlying cause. 92 In the final case, although Clostridium perfringens and Escherichia coli (both of which have the potential to result in emphysematous disease) were cultured from the bowel wall, specimens were collected post mortem and so it was not possible to confirm that these were the cause of the intestinal pneumatosis. 93
Key Points
Selective thickening of the muscularis layer of the small intestine is most suggestive of either IBD or small-cell lymphoma.
According to the majority of sources, lymphoma is the most common GI tumour in the cat and can present as one or more masses. An important differential for a GI neoplastic mass is a mass that is due to eosinophilic sclerosing fibroplasia, since the two conditions can have a similar appearance on ultrasound examination.
The ultrasonographic appearance of an intussusception in the cat is consistent with that described in the dog; in the transverse plane the affected intestinal segment assumes a circular ‘target-like’ or ‘bull’s eye’ appearance.
Linear foreign bodies are relatively common in the cat and cause intestinal plication, which is readily identifiable on ultrasound examination.
A thin hyperechoic line within the mucosal layer of the small intestine may indicate mucosal fibrosis, the clinical significance of which is presently unknown.
Pathology at the ICCJ may be detected ultrasonographically in the form of ileal and/or caecal wall thickening, enlargement of the caecal lymph nodes, hyperechoic mesenteric fat and/or a focal accumulation of peritoneal fluid in the region of the ICCJ.
A cyst with a muscular rim sign adjacent to a segment of intestine is suggestive of a duplication cyst.

Footnotes
Conflict of interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.