
Abstract
Practical relevance:
Traumatic stifle joint luxation is an uncommon but severe injury. There is usually rupture of several stabilising structures of the joint including the cruciate ligaments, collateral ligaments, joint capsule and menisci. Successful management of this condition requires good anatomical knowledge and repair or replacement of all damaged structures to achieve adequate joint reduction and stability. Better understanding of the treatment options available will aid clinical decision-making.
Clinical challenges:
Due to the significant joint instability associated with these injuries, surgical repair is challenging. The use of a temporary transarticular pin to hold the stifle joint in anatomic reduction greatly aids ligament repair or replacement. Postoperative joint immobilisation has traditionally been recommended to protect the primary repair and aid periarticular fibrosis, but prolonged immobilisation can have deleterious long-term effects on the joint. Thus recommendations for the duration of postoperative immobilisation vary between 2 and 6 weeks. Also, due to their independent, outdoor lifestyle, affected cats may have been involved in a significant trauma with important concurrent injuries that need to be addressed prior to the orthopaedic repair.
Evidence base:
Published data is limited, with reports including only a small number of cats. The information and recommendations in this article have therefore been drawn from the available literature, the authors’ experience and preliminary data from an ongoing multicentre retrospective study (unpublished).
Aims:
The aims of this article are to give the reader as thorough a summary as possible of the diagnosis, treatment, outcome and complications of traumatic stifle luxation.
Introduction
Cats are an extremely popular domestic pet across the world. In the UK alone, 25% of people own a cat, and there is an estimated population of 10.3 million cats. 1 Those with access to the outdoors are at risk of significant trauma, such as road traffic accidents or falls from a height, which can lead to injury of multiple body systems including the stifle joint and its associated soft tissue stabilising structures. Large extrinsic bending and torsional forces applied to the stifle can cause luxation due to variable disruption of multiple ligaments (primary joint restraints), the joint capsule, menisci, tendons and muscles (secondary joint restraints), all of which contribute to joint stability.2,3 The most common combination of soft tissue injuries is rupture of the cranial and caudal cruciate ligaments and the medial collateral ligament. 3
Initial triage and management
As these injuries are usually secondary to a high-energy trauma, the initial assessment should consist of evaluation of the major body systems to identify and treat any life-threatening injuries. A thorough description of the evaluation process for patients that have suffered a substantial trauma is beyond the scope of this article. As a brief summary, the mucous membrane colour, capillary refill time, pulse quality, and heart rate and rhythm should be assessed for evidence of haemodynamic compromise. Thorough thoracic auscultation and observation of the respiratory rate and character should be carried out. Pulmonary contusions, pneumothorax, rib fractures and diaphragmatic hernias can all lead to dyspnoea and therefore orthopaedic examination may need to be delayed. The abdomen should be palpated carefully to assess for discomfort and continuity of the body wall, in case of prepubic tendon injury and body wall rupture. The presence or absence of a palpable bladder should be noted, as the most common site of urinary tract rupture after trauma is the bladder. 4 An emergency minimum database should be performed, ideally including biochemistry (electrolytes, urea, creatinine, lactate, total solids), packed cell volume, blood pressure measurement, acid–base status, and thoracic and abdominal ultrasound (see box below). Screening thoracic and abdominal radiographs can be obtained once the cat is stabilised.
After initial assessment, appropriate analgesia should be provided. A full mu (μ) opioid agonist such as methadone (0.1–0.4 mg/kg IM or slow IV q4h) is recommended, with the dosage and frequency being based on appropriate pain scoring so as to avoid undesirable behavioural changes. Non-steroidal antiinflammatory drugs (NSAIDs) can be given if the patient is stable and biochemistry is unremarkable.
Diagnosis
Orthopaedic examination
Once the cat is stable, a careful orthopaedic examination should be performed to localise the source of pain. Most cats with stifle disruption will have a severe or non-weightbearing lameness with marked soft tissue swelling around the stifle joint. There will be pain on palpation of the stifle or on attempts to manipulate the joint.

Examination under sedation or general anaesthesia
Careful palpation of the stifle joint in the sedated or anaesthetised cat allows a better understanding of which structures have been compromised. Luxated stifles will be grossly unstable in multiple directions. The type of instability palpable will depend on the combination of structures affected but may include cranial and/or caudal drawer signs as well as valgus and/or varus instability. It is also relatively common for patellar luxation to be present. 13 In order to accurately assess the injured anatomical structures, the stifle joint should be manually reduced prior to applying any stress.
Radiography
Radiographs of the affected and contralateral stifle joint should be obtained for better characterisation of the injury, assessment of periarticular fractures (discussed in Part 2) and treatment planning (Figure 1). Avulsed fragments of bone may be seen at ligament insertion sites. Stress radiographs can be taken to assess for collateral ligament injury. For example, with medial collateral ligament injury there will be increased valgus movement and widening of the medial joint space. However, stress radiographs can be difficult to interpret and assessment by palpation of the anaesthetised patient is usually more rewarding.

Lateral (a) and caudocranial (b) radiographs of a luxated right stifle joint. Note the lack of contact between the articular surfaces of the femur and tibia, and the small avulsion fragments from rupture of the cruciate ligaments
Treatment
The goal of treatment is to repair damaged structures and restore anatomical joint alignment and stability.
Surgical exploration
The stifle joint is first explored surgically to definitively diagnose which structures will require repair. For this a lateral or medial parapatellar approach can be made. With either approach, the skin can usually be easily retracted to the other side to access the second collateral ligament. The joint capsule, collateral ligaments and intra-articular structures all need to be inspected (Figure 2). The cranial and caudal cruciate ligaments are usually both ruptured.

Cadaver specimen demonstrating the intra-articular anatomy of the stifle joint. CrCL = cranial cruciate ligament; CdCL = caudal cruciate ligament; MM = medial meniscus; LM = lateral meniscus
Almost all cases will have concurrent meniscal injuries, with peripheral avulsions being the most common. 3 Menisci should be probed in order to more accurately identify pathology. 14 Peripheral avulsions of menisci can be reattached to the joint capsule using horizontal mattress sutures of polydioxanone if the meniscus appears otherwise healthy; 3 however, more severe injury may require partial or total meniscectomy.
Dissection to view the collateral ligaments should be performed and sprains can be graded. Grade I sprains involve minimal fibre tearing and the ligament will appear intact. Grade II and III sprains are partial and complete ruptures, respectively, and will require surgical repair.
Temporary transarticular pin
In severely unstable joints a temporary transarticular pin can be placed prior to ligament reconstruction (see box below). This pin will hold the stifle joint in reduction, aiding appropriate tensioning of prosthetic sutures. 2 Overtightening and overcorrection can lead to subsequent subluxation. The pin is removed prior to closure and repair of the joint capsule.

Collateral ligaments
Ruptured collateral ligaments are sutured if possible using a locking loop pattern (Figure 3). A 4-0 monofilament slowly absorbable suture material, like polydioxanone, should be used.13,15 Suturing a ruptured ligament is sometimes not possible due to shredding of the ligament ends, in which case collateral ligament prostheses should be used.
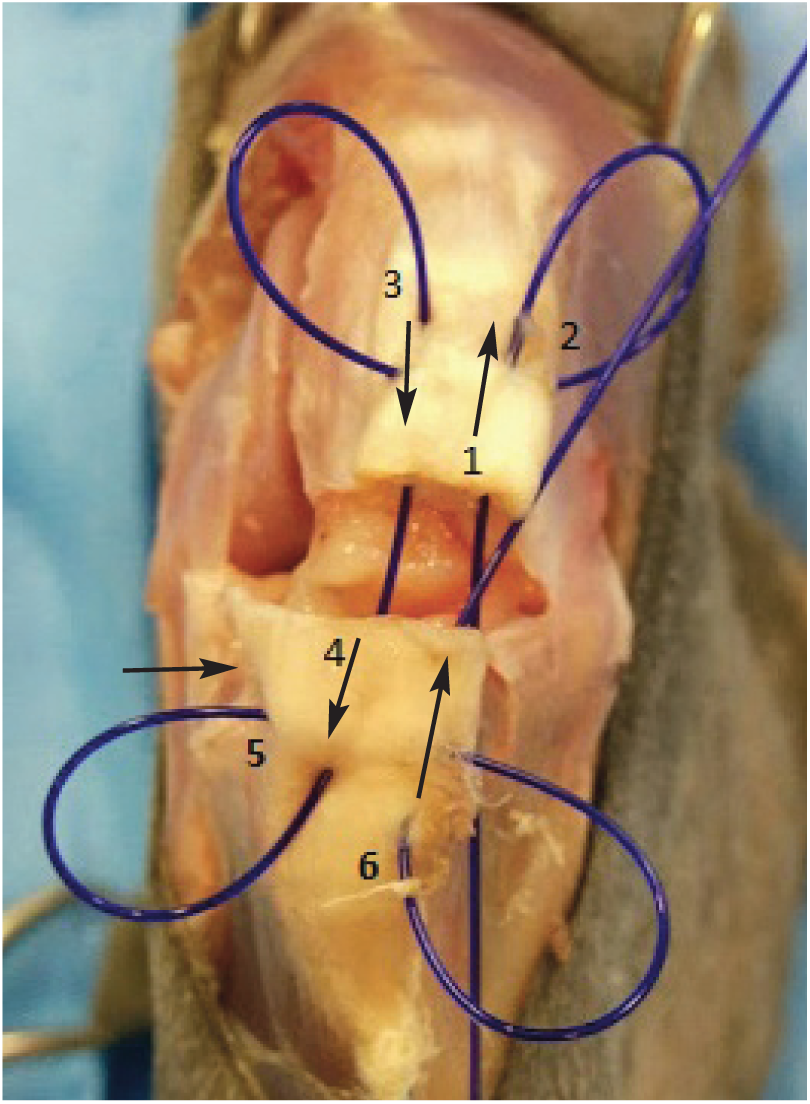
A locking loop suture performed on a patellar ligament (a cadaver specimen was used for the surgical images on this page). The numbers and arrows indicate the order and direction of needle passes required to complete the suture. The transverse bite should be closer to the ruptured end and more superficial than the longitudinal bite to encircle a bundle of fibres in the loop. Otherwise the suture will not grasp the fibres firmly
Medial collateral ligament prosthesis
A 2.0 mm screw or a suture anchor (Figure 4) is placed in the medial epicondyle of the femur, with another placed at the insertion site on the proximal tibia. If using screws, the use of washers will help to minimise suture slippage. Size 0 monofilament non-absorbable suture material should be anchored around the screw heads or threaded through the eyelet of the suture anchors in a figure-of-eight fashion (Figure 5).

2.0 mm suture anchors. Note the eyelet through which the suture is passed
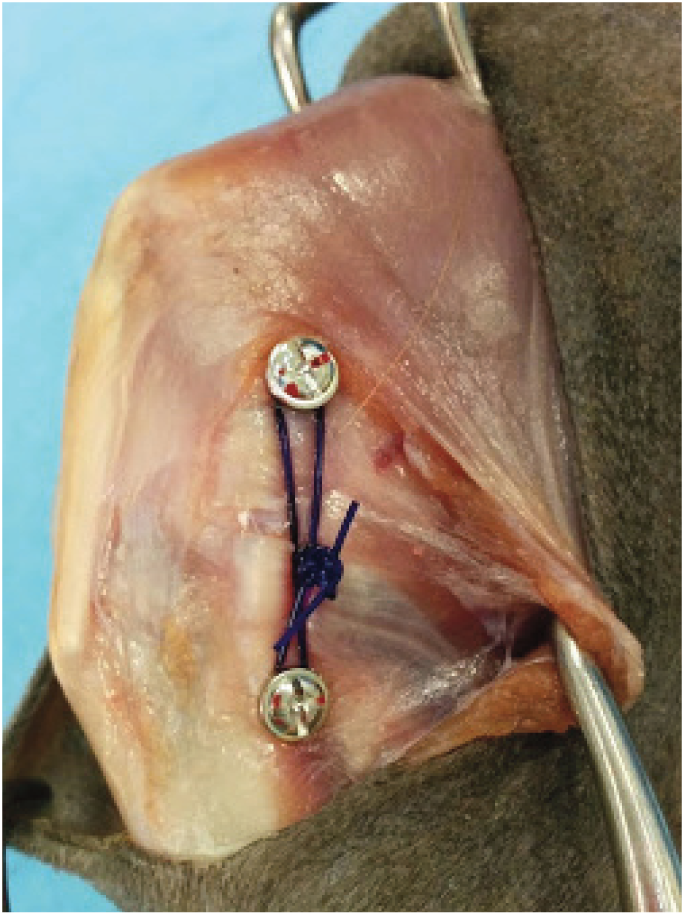
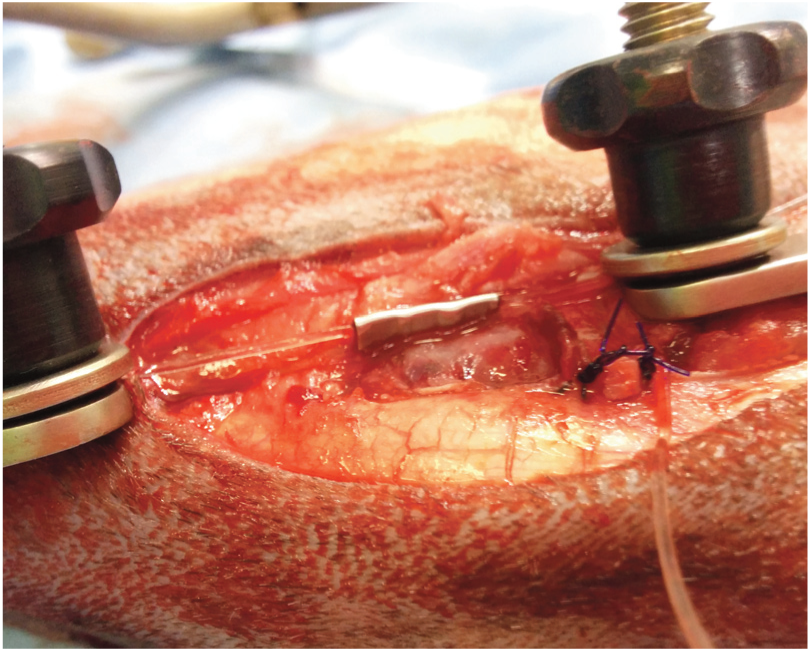
Example of a prosthetic suture applied when the medial collateral ligament of the stifle joint is compromised. Note the washers used to prevent suture slippage. The screws are placed at the origin and insertion of the medial collateral ligament
Lateral collateral ligament prosthesis
A 2.0 mm screw or a suture anchor is placed in the lateral epicondyle of the femur at the origin site of the lateral collateral ligament. The insertion point for the lateral collateral ligament is the fibular head. The suture can either be passed between the fibular head and tibia or passed through a small drill hole in the fibular head. Alternatively, a 1.5 mm screw can be directed from the fibular head into the tibia; 15 note that a 2.0 mm screw should not be used for this purpose as this may cause fragmentation of the fibular head. The peroneal nerve (Figure 6) runs just caudal to the fibular head, so care must be taken not to ensnare this in the suture. Size 0 monofilament non-absorbable suture is placed as described above in a figure-of-eight pattern (Figure 7).
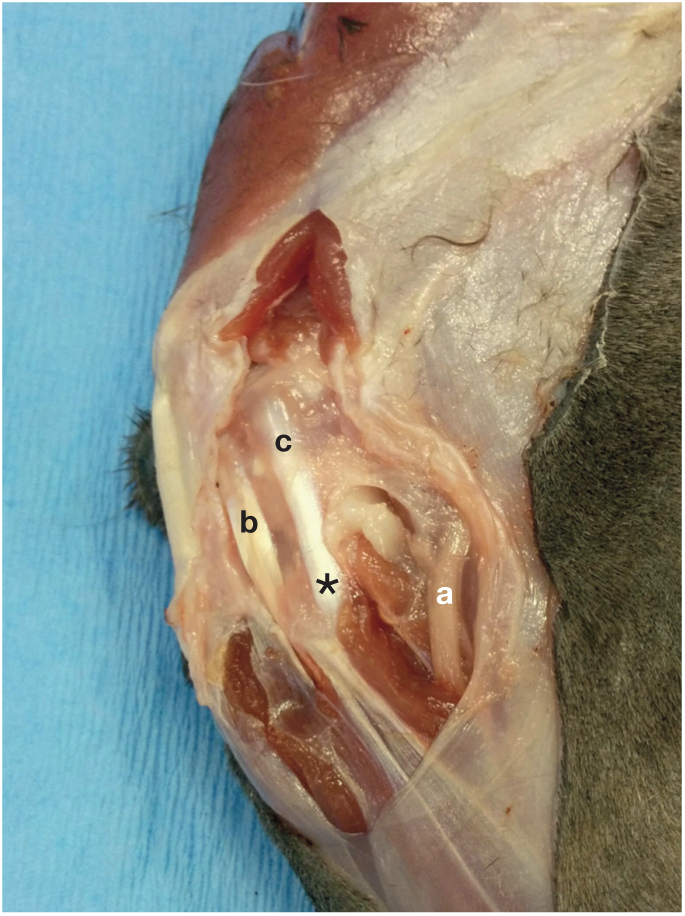
Position of the peroneal nerve (a) caudal to the fibular head. b = long digital extensor tendon; c = lateral collateral ligament; asterisk indicates the fibular head

Example of a prosthetic suture applied when the lateral collateral ligament of the stifle joint is compromised. The proximal screw is placed at the origin of the ligament on the lateral femoral epicondyle. The distal part of the suture is secured through a small drill hole in the fibular head

Cranial cruciate ligament
A lateral fabellotibial suture is placed to address rupture of the cranial cruciate ligament (see box above). The authors use 50 lb (23 kg) nylon leader line secured with a crimp, as this has been found to be stiffer and suffer less elongation than when secured with a knot (Figure 8). 16 The suture is traditionally placed around the fabella; however, in some cases there are concerns regarding laxity of the femorofabellar ligament or inadequate anchorage. If security of the suture around the fabella is a concern, a suture anchor can instead be placed caudally in the lateral femoral condyle just proximal to the joint capsule. 17 Note that if a suture anchor has already been placed for a lateral collateral ligament prosthesis then the same anchor can be used for both sutures. There is often insufficient space to place two suture anchors in this location.
Crimp clamp placement to secure a lateral fabellotibial suture. Note the three evenly spaced crimps along the crimp clamp to secure it in place. The suture is being held with the aid of a tensioner – two clamps are placed onto the suture which is held in tension during crimping by gelpi retractors applied to the end of the clamps (see image [d] in box above)
Caudal cruciate ligament
A fibulopatellar suture can be placed to address rupture of the caudal cruciate ligament (see box below). This suture is not always performed if a fabellotibial suture has already been placed. If caudal cruciate rupture has not been specifically addressed, the authors recommend repeat assessment of the caudal drawer test after placement of the fabellotibial suture and removal of the temporary transarticular pin. If there is any residual drawer sign, then placement of a fibulopatellar suture is recommended.
The suture can be placed circumferentially around the fibular head or through a small drill hole (1.1 mm) in the fibular head. It is then passed either around the patella or through the proximal aspect of the patellar ligament. This suture should not be over-tightened and may cause some irritation. Monofilament non-absorbable or slowly absorbable suture material can be used; the latter is usually the authors’ choice (0 polydioxanone).

Temporary postoperative immobilisation
Use of ancillary temporary transarticular immobilisation has traditionally been recommended to protect the primary repair and allow periarticular fibrosis to develop without loss of joint reduction. 15 The duration of time recommended for immobilisation ranges from 2–6 weeks.3,14 However, the use of postoperative immobilisation has been challenged due to the development of complications, such as fracture after placement of a transarticular external skeletal fixator, 3 as well as the deleterious effects of prolonged immobilisation on the health of the joint, including decreased cartilage stiffness and thickness, decreased production of synovial fluid, and reduced range of motion. 2 In order to limit the deleterious effects on the joint, the authors recommend a period of immobilisation of no longer than 4 weeks. Usually a period of 2–3 weeks is adequate. 15 Alternatively, a hinged transarticular external skeletal fixator, which allows some joint movement, can be used to limit some of these complications. 18
Splints and casts are not appropriate means of external coaptation because they are unable to provide rigid immobilisation of the stifle joint and are difficult to maintain. Sufficient immobilisation can only be provided using a transarticular pin or transarticular external skeletal fixator.
Transarticular pin
Unlike temporary transarticular pinning (ie, using a small pin to temporarily hold the joint in reduction, which is then removed intraoperatively – see box on page 422), a larger transarticular pin can be placed instead to maintain longer term joint immobilisation. A 2.4–3.2 mm Steinmann pin is introduced just proximal to the trochlear groove, through the stifle joint and exits the cranial cortex of the tibia (Figure 9). 15 The joint is immobilised at a functional standing angle (110–135°) and the pin is left slightly long to aid retrieval. After the period of immobilisation, a small stab incision is made over the femur or tibia to gain access to the pin for removal.

Lateral radiograph of a stifle joint stabilised with a transarticular pin. Note the screw position for placement of the prosthetic suture for repair of the lateral collateral ligament and the drill hole position in the cranioproximal aspect of the tibial tuberosity for the lateral fabellotibial suture. Courtesy of Sorrel Langley-Hobbs
Transarticular pins are relatively simple to place; however, they cause additional injury to intra-articular structures during placement. Fracture through the transarticular pin site, pin loosening, bending or migration, and pain associated with the pin while it is in place are also other possible complications. 19 Therefore, this technique is not recommended by the authors.
Transarticular external skeletal fixator
A type I lateral transarticular external skeletal fixator is used with 2.0 mm positive profile pins placed in the femur and 1.6–2.0 mm positive profile pins in the tibia. 15 Transfixation pins should not exceed 25% of the width of the bone. 20 The small Kirschner-Ehmer or mini-Imex systems are usually appropriate for most cats.
To place the pins, a small stab incision is made in the skin and a curved haemostat is used to bluntly dissect down to bone. The haemostat jaws can be spread to keep soft tissue away from the pin entry site. A pilot hole that is 10% smaller than the pin diameter is drilled first; placing positive profile pins without pre-drilling a pilot hole can lead to microfractures of the cortex, which reduces the integrity of the pin–bone interface and can increase the risk of pin loosening. The pin is then inserted at a slow speed (≤150 rpm) and it should exit the transcortex. 20 A connecting bar is bent to hold the stifle at a functional standing angle and is supported with an additional (‘A’ frame) bar connecting the proximal and distal ends (Figure 10). Alternatively, a hinged connecting bar can be used, which will allow some joint movement.

Lateral (a) and caudocranial (b) radiographs of a type I lateral transarticular external skeletal fixator. A crimp clamp was used to secure the lateral fabellotibial suture. Note the placement of the pins extending from the proximal third of the femur to the distal third of the tibia to reduce the risk of fracture. (In radiograph [a] the stifle is a little overflexed – ideally the stifle should be at a functional standing angle of around 110–135°)
Potential complications include pin breakage, pin loosening and iatrogenic fractures, which tend to occur through the pin holes. 3 Complications can be minimised by using positive threaded pins, which have increased resistance to pull-out in comparison with smooth pins. Slow-speed pin insertion is also important to limit heat generation, bone necrosis and thus pin loosening. Pins should be placed centrally in the bone and be of an appropriate size. If they are inserted and protrude too far out of the transcortex they should be left in place. Withdrawing them will weaken the pin–bone interface and increase the risk of pin loosening. 20 The risk of iatrogenic fracture can be reduced by placing the most proximal pin in the proximal third of the femur and the most distal pin in the distal third of the tibia, 3 in accordance with the near-far-far-near principle.
Postoperative care
Cats should be strictly confined for the first 6 weeks. If a transarticular external skeletal fixator is placed, the owners should be educated regarding pin tract cleaning and daily assessment. After 2–3 weeks (and no longer than 4 weeks), the postoperative immobilisation can be removed under sedation. Joint stability should be assessed at this time. Range of motion will be markedly reduced initially, but should improve when increased levels of activity are resumed. Continued confinement is still important at this stage, however, to prevent iatrogenic fractures through pin holes. 15
Additional analgesia at the time of removal of the transarticular fixation is advised – for example, meloxicam (0.05 mg/kg PO q24h) and/or buprenorphine (0.01–0.02 mg/kg sub-lingually q8h). Initially, a restricted range of motion of the stifle joint is expected and there may be some reluctance to use the limb. Analgesia and physical rehabilitation may be of assistance in reducing pain, increasing joint range of motion and improving outcome. For further discussion on feline physiotherapy and rehabilitation readers are referred to an earlier two-part article series in JFMS.21,22
Cats should be reassessed at 6 weeks postoperatively. If there is persistent discomfort or lameness, careful palpation of the stifle joint under sedation should be performed to identify any residual instability or surgical failure. Radiographs should also be obtained to assess the surgical repair, joint reduction and joint congruity. If the cat is progressing well, exercise can be increased slowly. The authors recommend a 4 week period of house rest prior to allowing any outdoor activity.
Outcome and complications
Information in the literature regarding the prognosis for a satisfactory return to function is very limited, with reports of only a very small number of cats available. One of the authors (EA) is involved in a multicentre retrospective study assessing these injuries in cats. Collection of long-term follow-up data is ongoing, but the results so far (unpublished) suggest that around 62% of cases have a good outcome (ie, minimal or non-existent ongoing lameness). One-third of cases, however, have persistent lameness or complications, that may lead to amputation or euthanasia. Reported complications include persistent stifle instability, medial and lateral patellar luxation, and those associated with the postoperative immobilisation (pin loosening/infection/breakage/migration, fracture of the tibia or femur through pin holes, reduced stifle range of motion). Owners should also be educated regarding long-term management of osteoarthritis and the importance of the prevention of obesity.
If surgical repair fails, arthrodesis is a possible salvage treatment; some owners may opt for amputation instead. Arthrodesis will cause a significant gait alteration with circumduction of the hindlimb. It can also affect the cat’s ability to jump, climb or walk with a crouched gait. Complications include fracture of the femur or tibia and at the bone–implant junction, as well as non-union and infection. 15 Therefore, careful owner education and thorough discussion is required prior to performing this procedure.
Key Points
Stifle disruption is usually secondary to a significant trauma; therefore, a thorough evaluation of the patient should be performed prior to addressing the orthopaedic injury.
Examination of the stifle joint under sedation or anaesthesia is the most accurate way to identify which supporting ligaments are affected. Radiography is performed to identify periarticular fractures and to aid treatment planning.
Meniscal damage and patellar luxation is commonly seen alongside this injury.
Affected ligaments should be repaired or replaced with prostheses to restore joint congruity and stability.
Postoperative stifle immobilisation can be used to protect the primary repair and aid periarticular fibrosis. However, the authors recommend a maximum duration of 4 weeks to limit long-term deleterious effects on the joint.
When treated appropriately, around two-thirds of cases will have a good outcome.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.