
Abstract
Objectives
The aim of this study was to assess the effect of three oral potassium supplements (potassium gluconate tablets [PGT], potassium gluconate granules [PGG] and potassium citrate granules [PCG]) on hypokalemia and serum bicarbonate in cats with chronic kidney disease (CKD).
Methods
Medical records (2006–2016) were retrospectively searched for cats that had been prescribed an oral potassium supplement for management of their CKD-associated hypokalemia. For inclusion, laboratory work had to be available at the time of hypokalemia diagnosis, and at recheck within 1–6 weeks. Treatment response was defined in three ways: any increase in potassium, an increase in potassium to within the normal reference interval, and an increase to >4 mEq/l.
Results
Thirty-seven cats met inclusion criteria (16 PGT, 11 PGG, 10 PCG). Dosing ranged from 0.21 to 1.6 mEq/kg/day for PGT, from 0.25 to 1.48 mEq/kg/day for PGG and from 0.04 to 1.34 mEq/kg/day for PCG. After supplementation, 36/37 cats had an increase in potassium, 34/37 increased to within the reference interval and 24/37 had an increase in potassium to >4 mEq/l. There was a statistically significant difference in serum potassium post-supplementation for all three treatments: PGT (P = 0.0001), PGG (P = 0.001) and PCG (P = 0.002). There was a positive correlation between PGT dose and change in potassium concentration (P = 0.04), but there was no significant correlation for PGG or PCG. In cats that had data available, serum bicarbonate increased >2 mEq/l in 1/6 PGT, 1/6 PGG and 3/4 PCG cats.
Conclusions and relevance
All three potassium supplements were effective in treating hypokalemia secondary to CKD in the majority of cats despite variable dosing. Data were limited to assess the alkalinizing effect and prospective studies are needed.
Introduction
Hypokalemia is a common finding in cats with chronic kidney disease (CKD), with approximately 20–30% of patients affected.1,2 It appears most commonly in International Renal Interest Society (IRIS) stage 2 and 3 CKD patients, and appears less commonly in IRIS stage 4 CKD cats, likely due to markedly decreased glomerular filtration. 3 The exact mechanism by which hypokalemia occurs in feline CKD patients is poorly understood, but is thought to be due to a combination of increased urinary loss due to polyuria and subsequent decreased reabsorption, vomiting, activation of the renin–angiotensin–aldosterone system and inadequate dietary intake.4,5 Potassium is the major intracellular cation and 95% of potassium is contained within muscle tissue. 6 Chronic metabolic acidosis associated with CKD encourages intracellular potassium depletion due to intracellular influx of excess hydrogen ions and concomitant efflux of potassium. 7 Therefore, it is thought that serum potassium concentrations may not be representative of intracellular potassium concentrations as normokalemic cats with CKD have been demonstrated to have lower muscle potassium concentrations than normal control cats. 6
Clinical signs of moderate-to-severe hypokalemia can include muscle weakness, particularly cervical ventroflexion, polyuria and polydipsia, tachycardia, constipation and anorexia. 4 Although hypokalemia has not been shown to be a risk factor for disease progression or outcome in CKD cats,8,9 studies in CKD cats have demonstrated improvement in renal function when normokalemia was restored with potassium supplementation. 10 In another study, healthy adult cats fed potassium-deficient experimental diets were shown to develop renal dysfunction, which was worsened with concomitant acidification.11,12 Therefore, evidence is sufficient to recommend potassium supplementation in CKD cats when serum potassium concentrations fall below the normal reference interval. Additionally, owing to the concern for failure of serum potassium concentrations to be representative of muscle potassium concentrations in the face of metabolic acidosis, 6 some clinicians advocate supplementation even when serum potassium is in the low normal reference interval, with a goal of maintaining serum potassium concentration above 4 mEq/l. 13
Although oral potassium supplementation has been demonstrated to effectively correct CKD-induced hypokalemia,6,10,14 there is little literature comparing the type of potassium supplementation and dosing regimens. Potassium comes in several oral forms: potassium gluconate, potassium citrate, potassium chloride and potassium bicarbonate, the latter two of which are not widely used owing to low palatability. 14 Dosing of potassium has been described by many,3,4,10,14 and the International Society of Feline Medicine consensus guidelines for CKD recommend treating with 1–3 mEq per cat q12h, with adjustment based on response. 13 Potassium citrate is thought to be an alkalinizing agent,3,4 which would provide additional benefit to address metabolic acidosis associated with CKD, but there is little information about its efficacy for this indication or the appropriate dose to achieve this effect. Adding supplements to the food of cats with CKD can be problematic and lead to food aversion; therefore, an understanding of the lowest effective dose would be beneficial for these patients.
The purpose of this retrospective study was to describe the effect of three oral potassium supplements on serum potassium and bicarbonate concentrations in cats with CKD.
Materials and methods
Data acquisition
Medical records from cats diagnosed with CKD that received oral potassium supplementation from June 2006 to June 2016 were retrieved from the Colorado State University Veterinary Teaching Hospital. Only those cats that were prescribed potassium supplementation for CKD-associated hypokalemia were included. For inclusion, one of three potassium supplementations had to be prescribed: potassium gluconate tablets (PGT [Tumil-K Tablet, Virbac]), potassium gluconate granules (PGG [Tumil-K Powder; Virbac]) or potassium citrate granules (PCG [Nutrived Potassium Citrate Granules; Vedco]). Concurrent use of parenteral potassium supplementation or oral sucralfate, or diagnosis of hyperaldosteronism or no diagnosis of CKD were the exclusion criteria.
Data collected included signalment (breed, sex, age, body weight), potassium supplement type, dose and directions for use, intended use of potassium supplementation, diet, indication owner was unable to give the supplement, and serum chemistry and urinalysis values. A biochemistry panel had to be available at the time of diagnosis of hypokalemia, as well as a recheck biochemistry within 1–6 weeks of diagnosis.
Data analysis
A total of 205 records of cats prescribed oral potassium supplementation were identified in the search. Altogether, 168 were excluded for the following reasons: no follow-up within 1–6 weeks (n = 61), concurrent use of KCl in intravenous fluids (n = 55) or subcutaneous fluids (n = 11), deceased before recheck (n = 12), on potassium supplementation before initial visit (n = 7), medical records unavailable (n = 4), diagnosis of Conn’s syndrome (n = 4), diagnosis of acromegaly (n = 1), no diagnosis of CKD (n = 1) or other miscellaneous reasons, including vague documentation of whether supplementation was continued to recheck, or discontinuing supplementation before recheck. This left 37 cats for inclusion in the study.
The determination of kidney disease was based on the attending clinician’s discretion and upon a combination of history, physical examination, serum biochemistry, urinalysis and diagnostic imaging. Enrolled cats were not staged according to IRIS guidelines as in some cases insufficient information to determine if this was appropriate was present in the medical record. The determination of comparative dosing between formulations was presented as a total daily dose and was calculated using the information that 1 PGT contains 2 mEq/l potassium, one one-quarter teaspoon PGG contains 2 mEq/l potassium and one scoop of PCG contains 2.8 mEq/l potassium. 15 Response to potassium supplementation was defined in three ways: (1) any increase in potassium from baseline; (2) an increase in potassium to within the normal reference interval (RI; 3.5–5.2 mEq/l); and (3) an increase in potassium >4 mEq/l.
Data were assessed with D’Agostino and Pearson test for normality and as not all data were normally distributed, a paired Wilcoxon Sign Rank test was used to compare pre- and post-supplementation serum potassium concentration. A Kruskal–Wallis test was also used to compare pretreatment serum potassium concentrations and prescribed dose between groups. Spearman’s rank correlation coefficient was used to assess correlation between potassium dose and change in serum potassium and serum bicarbonate. In order to assess the relative ‘potency’ of potassium supplementation type, change in serum potassium from baseline was divided by mEq/kg/day dose and the resulting number was compared between groups with the Kruskal–Wallis test. All analyses were performed in Prism version 7 (GraphPad), with significance defined as P >0.05.
Results
Thirty-seven cats were included in the study, two were ⩽5 years of age, three were 6–9 years of age, 11 were 10–15 years of age and 21 were >15 years of age. There was one intact female, 17 spayed females and 19 castrated males. Twenty-six cats were domestic shorthairs, eight were domestic longhairs and three were Siamese. Serum creatinine was 1.6–2.8 mg/dl in 18/37 cats, 2.9–5.0 mg/dl in 14/37 cats and >5.0 mg/dl in 5/37 cats. Diet history was available in 94% of cases: prescription renal diets exclusively (34%), prescription renal diets non-exclusively (5%) or non-renal diets (55%).
Of the 37 cats included in the analysis, 16 were given PGT, 11 were given PGG and 10 were given PCG. Several different dosing intervals were prescribed, including q48h (n = 2), q24h (n = 15), q12h (n= 17), q8h (n = 2) and q6h (n = 1). No significant difference in pretreatment serum potassium concentrations or mEq/kg dose of potassium prescribed were found between the supplementation groups.
After supplementation, 36/37 cats had an increase in potassium, 34/37 increased to within the RI and 24/37 had an increase in potassium to >4 mEq/l. Information regarding dosing and response to supplementation based on formulation is presented in Table 1. There was a statistically significant difference in serum potassium post-supplementation for all three medications: PGT (P = 0.0001), PGG (P = 0.001), and PCG (P = 0.002). There was no significant difference in dose of any of the formulations between cats that reached a target serum potassium concentration >4 mEq/l and those that did not. There was a positive correlation between PGT dose and change in potassium concentration (P = 0.04; Figure 1), but no significant correlation for PGG or PCG. When the relative potency of potassium supplementation type was assessed by dividing the change in serum potassium from baseline by mEq/kg/day dose there was no significant difference between groups.
Two of 37 cats had a change of dose at recheck (one increase and one decrease), and supplementation was discontinued in one cat per owner preference at the time of recheck due to difficulty with administration. In 7/37 cats, the supplement type was changed (three cats PGT to PGG, two cats PGG to PGT, one cat PGG to PCG and one cat PCG to PGG), with 5/7 cats having a notation in the chart this was due to palatability.
Only a small subset of patients had serum bicarbonate concentrations available for analysis (PGT: n = 6; PGG: n = 6; PCG: n = 4) and dosing and serum bicarbonate concentrations in response to supplementation are presented in Table 1. There was no significant difference between pre- and post-supplementation serum bicarbonate nor a correlation between potassium supplement dose and serum bicarbonate level. There were not enough data to describe effect on urine pH.
Dosing and response to potassium supplementation based on formulation

Data are median (range) unless otherwise indicated. A significant correlation was not found for potassium gluconate or citrate granules
Some cats had initial serum potassium 3.5–3.9 mEq/l (PGT: n = 3; PGG: n = 4; PCG: n = 2)
PGT = potassium gluconate tablets; PGG = potassium gluconate granules; PCG = potassium citrate granules; RI = reference interval
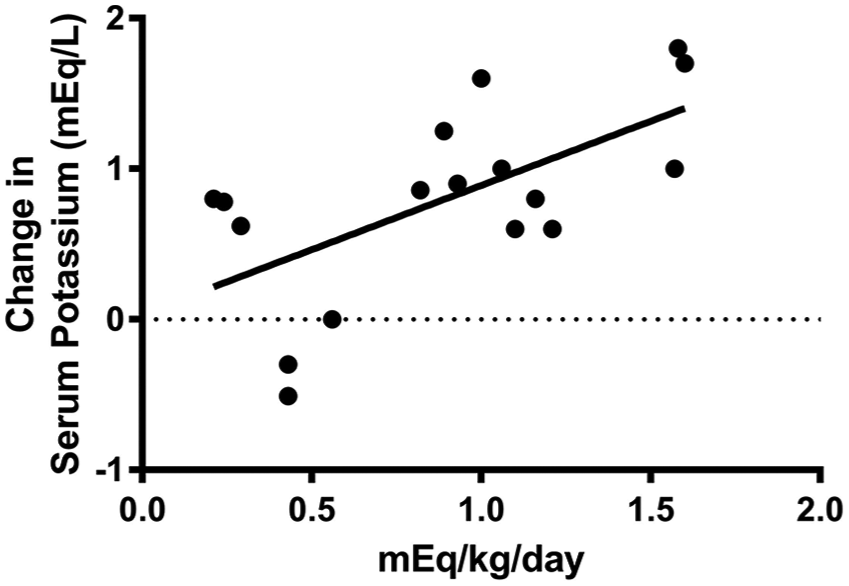
Correlation of dose vs change in serum potassium concentrations for potassium gluconate tablets using the Spearman rank correlation (P = 0.04, r = 0.51)
Discussion
In the majority of cats in this retrospective study, all three potassium formulations assessed were effective in treating hypokalemia secondary to CKD. However, ‘success’ varied depending on the therapeutic target used. When treatment success was defined as a serum potassium concentration >4 mEq/l, fewer cats met this target. However, this likely does not represent a ‘failure’ as, owing to the retrospective nature of the study, it was not possible to determine what the target potassium concentration was of the prescribing clinician. A small number of cats with an initial serum potassium of 3.5–3.9 mEq/l were started on potassium supplementation and it can likely be inferred in these cases that the target was >4.0 mEq/l. Although commonly suggested, it is still unknown whether a target serum potassium of >4 mEq/l is associated with a better outcome than a target of within the normal RI (or approximately 3.5 mEq/l). 13 An added complication is variability between laboratory normal RIs.
A wide range of doses and dose regimens were observed in the study. Dosing regimens ranged from every other day to four times daily, and thus for purposes of comparison the dose was presented as a calculated daily dose. The lowest prescribed dose of PGT resulting in a treatment response (for both increasing serum potassium into the RI and increasing to >4 mEq/l) was equivalent to 1 mEq/day. For PCG, the lowest prescribed dose was equivalent to 0.25 mEq/day (directions in two cats were to give 1/8 teaspoon once daily), which is significantly lower than consensus recommendations. 13 Despite this, both cats achieved a serum potassium >4 mEq/l on recheck laboratory work. This raises the question of whether lower doses of potassium would be equally as effective and potentially better tolerated if used as a food additive.
PGT supplementation showed a statistically significant correlation between dose and change in serum potassium concentration; however, there was a lack of correlation between PGG and PCG dose and change in serum potassium concentrations. A possible explanation for this observation is that as the powders are typically mixed into food, cats may have not finished the portion provided. Although no data could be collected about the amount of food ingested or appetite of the cats in this study, this finding may imply an inherent concern in mixing supplements into the food. Two of the three cats that did not achieve a serum potassium within the RI were also two of the cats reported to have a change in supplement type at recheck. Overall, despite potential feline non-compliance and the lack of correlation between dose and serum potassium concentration, the majority of cats experienced a treatment effect.
The cats included in this study were on a range of diets (prescription renal diet vs non-renal diet) and thus oral potassium intake was varied. Feline prescription renal diets typically include more potassium compared with other diets, 13 and therefore the question arises of whether lower amounts of potassium supplementation would be needed to achieve a therapeutic target in cats eating a renal diet. A previous study demonstrated that potassium supplementation was needed by 23% of cats on a normal diet vs 27.5% of cats on a renal diet, when a therapeutic target of 3.5 mmol/l was used. 16 However, the specific diet used in that study may not be applicable to the cats in the present study given changes in diet formulation over time. In future studies assessing the efficacy of potassium supplementation, having a standardized diet would be ideal to control for dietary potassium intake.
Based on these observations, response to supplementation seems unpredictable, and individual variation such as formulation, acceptance, diet, stage of kidney disease, acid–base status, intestinal health, concurrent medications, etc, likely play a role. Therefore, monitoring of serum potassium levels after initiation of therapy would allow a plan to be tailored to the individual patient.
Potassium citrate is commonly recommended as an alkalinizing agent, and in CKD it could be dually beneficial for both potassium supplementation and alkalization.3,4 However, few studies have been performed to confirm its efficacy. Analyses of the alkalinizing effect of potassium citrate supplementation were underpowered in this study owing to a lack of a recheck serum bicarbonate concentration and urine pH in the time frame of interest. Additionally, blood gas parameters may be more accurate for assessing acid–base status and this was uncommonly performed in these patients. However, when the data were subjectively assessed, more CKD cats receiving PCG had an increase in serum bicarbonate >2 (75%) in comparison to CKD cats receiving the other supplement forms (17% for both PGT and PGG). Additionally, the cats receiving PCG had subjectively lower doses than cats receiving other forms of supplementation. Thus, the perception that potassium citrate acts as an alkalinizing agent in CKD merits further investigation.
There are inherent limitations to a retrospective study that were encountered. The target patient population of interest was cats with CKD that were receiving potassium supplementation, but a determination of chronic, acute or acute on chronic could not necessarily be made from the data gathered. As such, no conclusion regarding the effect of potassium supplementation on serum creatinine can be drawn from the present data given the uncontrolled and retrospective nature of the study. The target indication was based on the attending clinician’s discretion. A wide range of doses, dosing frequency, recheck times, and starting and target serum potassium concentrations were found during data collection, which is an inherent limitation of a retrospective study. In a prospective study, timing and dosing schedule would be consistent to better compare response to therapy. Owner compliance with medication administration is a possible concern that has to be considered when viewing the results, as owners may have indicated the supplement was given more regularly than was actually achieved. Lastly, the records did not include all the data of interest for some cats, and this decreased the power.
Conclusions
In the majority of cats, all three potassium supplements examined were effective in treating hypokalemia secondary to CKD. Response to supplementation seemed unpredictable based on dose, likely for a variety of reasons, with some cats achieving a therapeutic effect with smaller doses than commonly recommended. Thus, monitoring should be recommended to tailor therapy to individual patients and minimize the burden of medications administered. Data were limited to show a definitive alkalinizing effect of potassium citrate. Prospective studies to investigate dose–response correlation and the alkalinizing ability of potassium citrate are needed for a more thorough assessment.
Footnotes
Author note
The results of this study were presented in part, as a poster abstract, at the American College of Veterinary Internal Medicine Annual Forum, National Harbor, MD, 2017.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by Buttons Fund for Feline Chronic Kidney Disease Research.
Ethical approval
This study did not involve the use of animals and therefore ethical approval was not required.
Informed consent
This study did not involve the use of animals and therefore informed consent was not required. No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.