
Abstract
Objectives
The aims of this study were to evaluate the safety of mustargen, vincristine, procarbazine and prednisone (MOPP) chemotherapy in the treatment of relapsed or refractory feline lymphoma, and to determine the overall response rate and median remission time with this protocol.
Methods
The medical records of 38 cats with relapsed or refractory lymphoma treated with MOPP chemotherapy at three institutions (University of Pennsylvania, the Animal Medical Center, and VCA Western Veterinary Specialist and Emergency Centre) were examined. Information evaluated included patient signalment, feline immunodeficiency virus/feline leukemia virus status, anatomic location(s) of lymphoma, prior protocols (type and number), MOPP doses, MOPP response, remission duration, hematologic and biochemical parameters, and owner-reported adverse effects.
Results
Overall, 70.3% of cats responded to MOPP chemotherapy. Among the responders, the median remission duration was 166 days. The most common adverse effects were neutropenia and gastrointestinal upset, which were reported in 18.4% of cats. In 55.3% of cats, no adverse effects were reported. In total, 30.8% of responders continued to respond 6 months following the initiation of MOPP, and 15.4% maintained a response 1 year after starting MOPP.
Conclusions and relevance
MOPP is a safe protocol for the treatment of relapsed or refractory feline lymphoma, with a promising overall response rate and median remission time.
Keywords
Introduction
Lymphoma is the most frequently diagnosed hematopoietic tumor in cats, representing approximately one-third of all feline neoplasms. 1 The Working Formulation classification scheme identifies a majority of feline lymphomas as intermediate (35%) to high (50%) grade, for which multi-agent chemotherapy protocols are the mainstay of treatment. 2 Induction chemotherapy protocols for cats with intermediate- and high-grade lymphoma most commonly comprise a combination of cyclophosphamide, vincristine and prednisolone (COP) or cyclophosphamide, doxorubicin, vincristine and prednisolone (CHOP), and reported response rates vary from 38% to 96%.3–7
A persistent challenge in the treatment of feline lymphoma is re-induction of durable remissions following relapse. Previously reported rescue protocols include single-agent treatment with lomustine or doxorubicin (for cats treated with COP at induction), or combination protocols such as dexamethasone, melphalan, dactinomycin and cytarabine (DMAC), or mechlorethamine, vincristine, melphalan and prednisolone (MOMP) – response rates to these protocols vary from 22% to 58.3%, with median progression-free intervals ranging from 14 to 39 days.8–11 To date, mechlorethamine-based rescue therapy for feline lymphoma has received little attention in the literature. One publication reports on 4/16 cats with gastric lymphoma receiving mechlorethamine-based chemotherapy, with no response rate reported. 12 Martin and Price retrospectively evaluated MOMP rescue chemotherapy in 12 cats, with a reported response rate of 58.3% and median progression-free survival of 39 days. 11
The MOPP chemotherapy protocol is comprised of mechlorethamine, vincristine, procarbazine and prednisone, and was originally developed for the treatment of Hodgkin and non-Hodgkin lymphoma in people.13,14 MOPP is commonly used in the treatment of canine lymphoma, where response rates of up to 98% in chemo-naive patients and 75% in the rescue setting have been reported.15,16 When used as a rescue protocol in canine patients, a median overall response duration of 33 days has been reported. 15
The aims of this retrospective study were to evaluate the safety of MOPP chemotherapy in the treatment of relapsed/refractory feline lymphoma, and to evaluate the overall response rate and median remission time with this protocol. To our knowledge, this is the first evaluation of the MOPP protocol in feline lymphoma patients.
Materials and methods
Case selection
The medical records database of the Matthew J Ryan Veterinary Hospital of the University of Pennsylvania was reviewed from January 1992 to July 2018, and cats with a cytologic or histopathologic diagnosis of lymphoma that were treated with a MOPP-based protocol in the rescue setting were included. Twenty-nine additional cats treated with MOPP between January 1992 and November 1997 at the Animal Medical Center (New York City) were also included, and one case was contributed from VCA Western Veterinary Specialist and Emergency Centre (Calgary, Canada).
Information obtained from the medical records included patient signalment, feline immunodeficiency virus (FIV)/feline leukemia virus (FeLV) status, anatomic location(s) of lymphoma, prior protocols (type and number), date of relapse or progression, date of MOPP initiation, chemotherapy doses, date of progression, hematologic and biochemical variables (when available), and owner-reported adverse effects. Details of the MOPP protocol are outlined in Table 1.
MOPP drugs and dosing

Either vincristine or vinblastine was chosen, based on clinician preference
Either prednisolone or prednisone was chosen, based on clinician preference
Among responders, MOPP remission time was calculated from the date of clinical response following the first MOPP cycle to the date of clinical progression as recorded by the attending clinician. Owing to the retrospective nature of this study, standardized restaging evaluations did not occur. Therefore, response to therapy was defined as improvement in clinical signs or measurable disease, and progressive disease was defined as worsening or recurrence of disease-associated clinical signs, or worsening of measurable disease (based on physical examination and diagnostic testing). When available, hematologic, biochemical and clinical toxicities were recorded. Toxicities were graded according to the Veterinary Comparative Oncology Group – common terminology criteria for adverse events (VCOG-CTCAE) version 1.1 when possible. 17
Statistical analysis
Descriptive statistics were calculated. Continuous data are expressed as means ± SD, unless not normally distributed, in which case median values and ranges are reported. Categorical data are expressed as frequencies. Median remission and survival times were determined using the Kaplan–Meier product limit method.
Results
Thirty-eight cats with a diagnosis of relapsed/resistant lymphoma treated with MOPP were identified (Table 2). The majority of the cats were domestic shorthairs (n = 27/38 [71%]), and mean age at diagnosis was 11.6 ± 3.99 years. All cats were altered, with 11/38 (29%) female spayed cats and 27/38 (71%) male castrated cats.
Patient characteristics
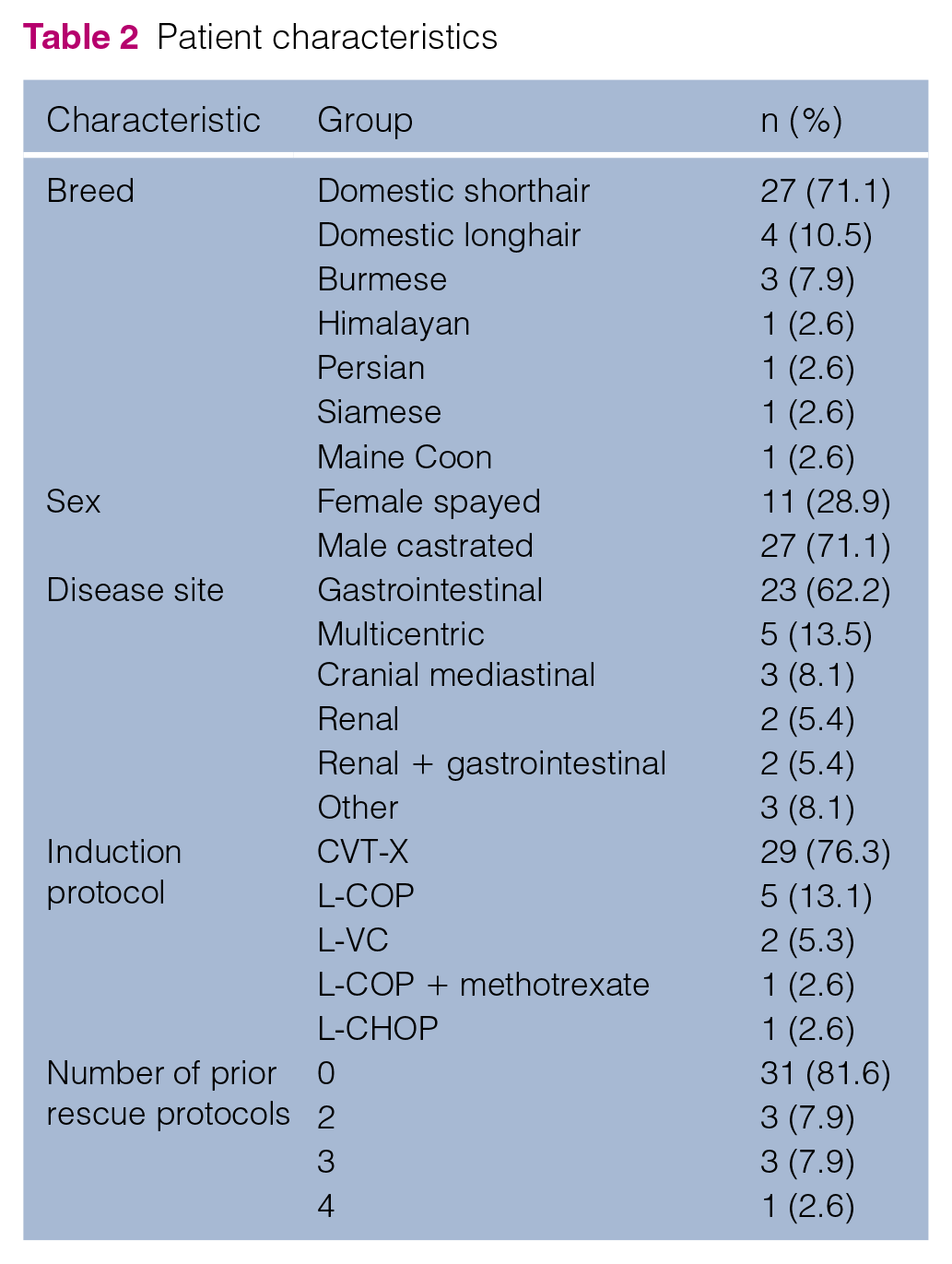
Anatomic site of disease was available in 37/38 cats, with a majority (n = 23/37 [62%]) having gastrointestinal lymphoma. The next most common site was multicentric, in 5/37 (13.5%) cats. Other disease sites included cranial mediastinal (n = 3/37 [8%]), renal (n = 2/37 [5%]) and renal plus gastrointestinal (n = 2/37 [5%]). One cat had multicentric lymphoma with conjunctival involvement in the right eye, which was identified as B-cell Hodgkin-like lymphoma on histopathology with immunohistochemical staining. Another cat’s lymphoma appeared to be restricted to the right mandibular lymph node, which was identified as a T-cell-rich B-cell lymphoma. Aside from these two cats, immunophenotyping was available for one additional cat with multicentric T-cell lymphoma. FIV/FeLV status was available for 31 cats, 30 of which were FIV/FeLV negative. The single FeLV-positive cat was the cat with B-cell Hodgkin-like lymphoma. Disease stage or subtype was not available for the majority of cats.
Prior to MOPP rescue therapy, induction protocols included: L-asparaginase and vincristine, followed by alternating cyclophosphamide, doxorubicin, vincristine and methotrexate, with continuous prednisone (CVT-X); 18 L-asparaginase followed by alternating cyclophosphamide, vincristine and vinblastine with concurrent prednisolone treatment (L-COP); L-asparaginase followed by alternating cyclophosphamide, vincristine and vinblastine (L-VC); L-COP + methotrexate; and L-asparaginase followed by alternating cyclophosphamide, doxorubicin and vincristine with concurrent prednisone treatment (L-CHOP). All cats were transitioned to MOPP chemotherapy because of progressive (relapsed or refractory) lymphoma.
Response to induction protocol was known for 30 cats. A complete response (CR) was observed in 22 (73%) cats, a partial response (PR) in seven (23%) cats and no response (NR) in one (3%) cat; thus, 29/30 (97%) cats were considered to have relapsed lymphoma, and the one cat that did not respond to induction chemotherapy was considered to have refractory lymphoma. First remission duration was known for 37 cats, and the median was 71 days (range 0–1026 days). Cats that had a CR to their induction chemotherapy had a median first remission duration of 166.5 days (range 45–1026 days), and cats that had a PR to their induction chemotherapy had a median first remission duration of 21 days (range 7–36 days). Induction and rescue protocol data are summarized in Table 1. In addition to other rescue protocols, one cat had a lymph node extirpation performed prior to MOPP rescue, and one cat had radiation therapy (nine fractions of 4 Gy) performed prior to MOPP rescue.
Vincristine was given at a median dose of 0.4 mg/m2 (range 0.35–0.43 mg/m2). Vinblastine was substituted for vincristine for 5/38 (13%) cats, with a median dose of 1.35 mg/m2 (range 0.96–1.45 mg/m2). Mechlorethamine was given at a median dose of 3.0 mg/m2 (range 1.9–3.0 mg/m2). Thirty-six of 38 (95%) cats received 10 mg per day of procarbazine on days 0–13 of each MOPP cycle. Procarbazine was held in one cat during the first week of therapy, and dosing information was not available for the second cat. Prednisone or prednisolone was chosen for the glucocorticoid component of therapy, based on clinician preference. Seven of 38 (18%) cats received 5 mg prednisolone daily, with the remaining majority of cats receiving 10 mg of prednisone daily. One cat began treatment with prednisone, and was later transitioned to prednisolone owing to improved options for oral dosing. Patients received dose reductions or drug holidays at the discretion of the attending clinician.
Quantitative hematologic and biochemical data were not available for the majority of cats, prohibiting grading according to the VCOG-CTCAE. However, 6/38 (15.8%) cats were reported to experience anemia following initiation of MOPP rescue, 7/38 (18.4%) cats were reported to experience neutropenia, 2/38 (5.3%) cats were reported to experience thrombocytopenia, 3/38 (7.9%) cats experienced lethargy and 6/38 (15.8%) cats experienced inappetence or anorexia. One cat experienced each of the following adverse effects: an extravasation reaction, vomiting and weakness. One cat with renal involvement of its lymphoma experienced progressive azotemia during MOPP rescue. In 21/38 (55.3%) cats, no adverse effects were reported.
Complete restaging was not routinely performed in all cases; therefore, objective classification of patients into complete responders, partial responders or non-responders was not performed. Response to therapy was defined as improvement of clinical signs and measurable disease (based on physical examination and/or diagnostic testing) following initiation of MOPP chemotherapy, and disease progression was defined as worsening or recurrence of clinical signs, and/or progression of measurable disease (based on physical examination and/or diagnostic testing).
MOPP remission time was available for 30 cats. Out of the responders within this cohort (19 cats), the median remission time following institution of MOPP rescue was 166 days (range 7–833 days; Figure 1). Overall, 26/37 cats responded to MOPP rescue, resulting in an overall response rate of 70%. Of the 22/37 cats with a known CR to induction chemotherapy, 14 (63.6%) of these cats responded to MOPP for a median of 190 days (range 7–833 days). For the 7/37 cats with a PR to induction chemotherapy, four (57.1%) responded to MOPP for a median of 125.5 days (range 51–585 days). Also, 8/26 (30.8%) responding cats maintained a response 6 months after beginning MOPP rescue, and 4/26 (15.4%) responding cats maintained a response 1 year after starting MOPP rescue.

Kaplan–Meier survival plot showing the median remission time (defined as the time from clinical response to MOPP rescue to the time of clinical disease progression) of cats treated with MOPP
Discussion
Although response rates of up to 96% are reported in chemo-naive feline lymphoma patients, 7 the re-induction of sustained remissions remains a challenge in cats with relapsed or resistant lymphoma. The mechlorethamine-based MOPP protocol outlined herein resulted in a favorable overall response rate of 70.3% in the rescue setting, which is comparable to the 75% response rate previously reported in the rescue setting in canine patients. 15 Although a direct comparison to other rescue protocols is limited by the retrospective study design, this response rate compares well with previously reported rescue protocol response rates in feline patients, which range from 22% to 58.3%.8–11 Out of the responding cats, the median remission duration following MOPP-based rescue therapy was 166 days. This compares favorably with previously reported response durations of other rescue protocols in feline patients, ranging from 14 to 39 days.8–11
A recurrent concern regarding mechlorethamine-based chemotherapy protocols is the risk of treatment-related adverse effects. MOPP rescue therapy was well tolerated by a majority of cats in this study, with 55.3% of cats reporting no adverse effects. In total, 18.4% of cats experienced an episode of neutropenia, which is comparable to the 21–42.7% of cats previously reported to experience neutropenia when treated with multi-agent chemotherapy protocols in the rescue setting.8,11 Altogether, 18.4% of cats experienced gastrointestinal toxicity, which is comparable to the 5–42.7% incidence that has been previously reported with other multi-agent chemotherapy rescue protocols.8,11 To our knowledge, one other publication (Martin and Price) 11 has evaluated a mechlorethamine-based chemotherapy protocol in 12 feline patients. In this study, 41.7% of patients experienced hematologic toxicity (four cats with grade 1 neutropenia, one cat with grade 3 neutropenia) and 8.3% of patients (one cat) experienced gastrointestinal toxicity. 11 Taken together, these data suggest that mechlorethamine-based rescue protocols are well tolerated by most cats, with comparable incidences of adverse effects to other rescue protocols.
Another concern with mechlorethamine-based protocols is that of patient and healthcare personnel safety during chemotherapy administration. Mechlorethamine is a toxic compound with irritant and vesicant properties, and any inhalation of vapors or dust (or contact with skin/mucous membranes) should be avoided. 19 USP<800> is a recently revised chapter written by the United States Pharmacopeial Convention to describe the best practices for handling hazardous drugs in healthcare settings. USP<800> advises healthcare personnel to wear appropriate personal protective equipment (PPE) during receipt, storage, transport, compounding, administration, deactivation/decontamination, cleaning, spill control and waste disposal of hazardous drugs. 20
For mechlorethamine specifically, the safety data sheet recommends preparation of injectable mechlorethamine in a class 2 laminar flow biological safety cabinet, with attendant personnel wearing chemical-resistant, impervious gloves, safety goggles and outer garments. 19 Following administration, mechlorethamine is chemically transformed within several minutes and is no longer circulating in its active form. 19 As with all chemotherapy protocols, owners and healthcare providers should be counseled regarding the potential risks of chemotherapy exposure prior to treatment. With appropriate patient handling (including chemical restraint if warranted), owner and staff education, and safety measures (class 2 laminar flow biological safety cabinet, closed injection system, PPE including respiratory protection), mechlorethamine can be administered in a comparably safe manner to other injectable chemotherapeutics.
Another set of factors to consider are the risks of compounding oral chemotherapy (procarbazine) for use in feline patients. Owing to the large number of compounding pharmacies and the lack of consensus standards to evaluate accuracy and consistency, there is concern for substantial variation between compounded products. This concern is underscored by a publication from Burton et al, 21 in which the potency of compounded lomustine for use in canine patients was reported to range from 50% to 115% of the labeled concentration. In an effort to mitigate this risk, the use of compounding pharmacies that practice independent quality-control assessment is recommended. Compounding of chemotherapy is not routinely practiced in all countries, which obviously limits this particular risk for practitioners who do not use compounded drugs. Another risk involved with administering oral chemotherapy is the potential for owner exposure. For this reason, it is recommended that pregnant or nursing individuals avoid handling chemotherapy, and that gloves are worn at all times during administration.
Limitations of this study include its retrospective nature, resulting in inconsistencies in staging performed and lack of quantitative hematologic data. Protocols for nadir assessment varied between institutions, which may have resulted in differences in the reporting of adverse hematologic effects. The patients evaluated were treated at three institutions over a wide timespan – with the earliest cats treated in 1992. Given this, the available data are limited to what was recorded at that time. Histopathology was performed for a majority of cases, but histologic tumor descriptions were unavailable (owing to the long time span of the study) – as such, the cases reported herein were not able to be classified by cell size. As the prognosis varies considerably between feline small-cell and large-cell lymphoma, and because overall survival measures are often confounded by variability in owners’ decisions on euthanasia, overall survival data are not reported.
Regarding future directions, a prospective assessment of first-line feline rescue protocols would allow a contemporaneous comparison of protocol toxicities, response rates and durations. The median remission time reported herein was 166 days, with 30.8% (n = 8/26) of responding cats maintaining a response 6 months following the initiation of MOPP rescue, and 15.4% (n = 4/26) of responding cats maintaining a response 1 year after starting MOPP rescue. Given these findings, a prospective assessment of MOPP in the first-line setting for feline lymphoma may be warranted. For cats with gastrointestinal involvement of their lymphoma, radiation therapy has previously been described in both the induction and rescue setting,22,23 with favorable results. Prospective evaluation of combination abdominal irradiation with MOPP chemotherapy in the induction or rescue setting represents another avenue of potential research.
Conclusions
MOPP rescue chemotherapy was well tolerated in the patient group assessed in this study, with a promising overall response rate of 70.3% and median remission duration of 166 days.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.