
Abstract
Objectives
The aim of this study was to prospectively compare perioperative pain score and wound parameters, inclusive of postoperative swelling and erythema, between flank and midline ovariectomy (OVE) in cats, performed by final-year veterinary students.
Methods
Healthy cats presented for routine OVE were randomly assigned to either the midline or flank group after owner consent to participate in the study. Perioperative protocols were standardised for both groups. Clinical data were collected prior to surgery, intraoperatively, at 1 h postoperatively, at the time of discharge, and at 3 and 10 day postoperative re-examination appointments. Data recorded included duration of surgery and anaesthesia, intraoperative complications, Feline Acute Pain Scale (FAPS) scores, a simple descriptive scale of reaction to wound palpation (SDSwound), a dynamic and interactive visual analogue scale assessment of pain (DIVAS), and both a simple descriptive scale (SDSswelling) and a visual analogue scale (VASswelling) of surgical wound swelling.
Results
Thirty-eight cats received a flank OVE and 37 received a midline OVE. Duration of surgery, duration of anaesthesia and intraoperative complications did not vary significantly between the two groups. Cats in both groups had significantly higher FAPS scores after surgery (P = 0.0002), with cats receiving a flank OVE having significantly higher pain scores compared with a midline OVE at 1 h postoperatively (P = 0.0004) and at discharge (P = 0.002). Swelling of the surgical wound (SDSswelling) was significantly higher in cats receiving a midline OVE at the time of discharge (P = 0.048), as well as at the 3 day (P <0.0001) and 10 day (P = 0.001) postoperative re-examinations. FAPS scores were significantly higher in cats receiving a midline OVE at the 3 day (P = 0.016) and 10 day re-examinations (P = 0.045). No cats in either group suffered a wound breakdown or infection.
Conclusions and relevance
Our study does not support advocating a preferred surgical approach for feline OVE within a teaching environment.
Introduction
While elective sterilisation of female cats is one of the most common procedures performed by veterinary surgeons worldwide, significant geographical variations are noted both in the technique and the surgical approach. 1 Historically, removal of both ovaries and the uterus (ovariohysterectomy [OVH]) was advocated, although there is an increasing trend towards removal of the ovaries alone (ovariectomy [OVE]), which has been performed for decades in some European countries.2,3 Reasons for sterilisation include population control, 4 elimination of undesirable behaviours, 5 and preventing hormonally driven diseases of the female reproductive tract and mammary tissues.6,7 All of these aims can be accomplished through OVE alone and this is the current method of routine, healthy, female feline sterilisation taught to veterinary students at our institution.
OVE can be performed through either a flank laparotomy or ventral midline coeliotomy approach. There is limited published data describing which approach is favoured for feline OVE; however, in the UK, 96% of practitioners report favouring a flank approach for OVH in cats, while a midline OVH approach is preferred in the USA.8,9 Multiple studies have shown no strong superiority between the flank or midline approach to OVH in cats, although flank laparotomy may be associated with increased pain scores and wound complications in the immediate postoperative period.8,10,11 There are limited data comparing feline OVE surgical approaches, although a single study comparing flank with midline OVE in cats showed no difference in pain scores between the approaches. 3
The aim of this prospective, cohort study was to test the null hypothesis that there would be no significant differences in the duration of surgery and anaesthesia, intraoperative complications, pain scores and perioperative wound parameters between the flank and midline approaches to OVE in cats when performed by final-year veterinary students under the supervision of a qualified veterinary surgeon.
Materials and methods
Study population
Client-owned, healthy female cats presenting for elective neutering were enrolled prospectively. Cats were required to be classified as American Society of Anesthesiologists category 1 based on a full physical examination. Cats displaying signs of oestrus or pregnancy, or lactating at the time of presentation were excluded. Enrolment was voluntary and required full written consent from the owner. Owners with a preference for either a flank or midline approach were excluded from the study. Approval for the study was granted by the university ethics committee.
Cats were admitted on the morning of surgery and discharged later the same day. Owners were instructed to withhold food but not water from midnight prior to the procedure. Following enrolment and admission to the hospital, cats were randomly assigned to either the flank or midline group by block randomisation.
Anaesthetic protocol
A standardised anaesthetic protocol for both approaches was followed. Buprenorphine hydrochloride (Buprecare; Animalcare) at 0.02 mg/kg was administered by intramuscular (IM) injection as a pre-anaesthetic medication (analgesic) 30 mins prior to surgery. The hair overlying a cephalic vein was clipped and EMLA cream 5% (AstraZeneca) applied, with a loose bandage placed over it to prevent ingestion. After 20 mins an IM injection of medetomidine hydrochloride (Domitor; Pfizer Animal Health) at 0.01 mg/kg was administered. Cats were left undisturbed in their cage for a further 5 mins before an intravenous (IV) cannula was placed in the prepared cephalic vein. General anaesthesia was induced with IV propofol (Propoflo; Abbott Animal health), administered to effect. Lidocaine hydrochloride (Intubeaze; Dechra) was applied to the larynx to facilitate the placement of a non-cuffed endotracheal tube. General anaesthesia was maintained by spontaneous breathing of isoflurane (IsoFLo; Abbott Animal Health) delivered in oxygen via a Jackson Rees modified T-piece with a closed bag and an adjustable pressure limiting valve. Anaesthetic depth was assessed by monitoring trends in heart and respiratory rate, blood pressure, eye position, jaw tone, response to surgical stimulation and palpebral reflex, with isoflurane concentration tailored accordingly. A multi-parametric monitor (iMEC 8Vet; Mindray) was used to monitor capnography, oesophageal temperature, electrocardiography and pulse oximetry throughout anaesthesia. Non-invasive blood pressure was measured using the Doppler technique, with the Doppler probe (Ultrasound Blood Flow Detector MD4; Sonomed) placed over the palmar metacarpal arch artery of the thoracic limb that had not been intravenously cannulated. IV fluid therapy was not administered to patients unless a mean blood pressure lower than 60 mmHg was noted. In such a situation, a 10 ml/kg bolus of lactated Ringer’s solution (Aquapharm Hartmann’s Solution for Infusion; Animalcare) was administered over 5 mins before re-evaluation of blood pressure and repeating the bolus if necessary. Active heating was performed using an electric heat pad (flexible heat pad; JAK Marketing) placed beneath the bedding on which the cat was positioned.
On completion of surgery meloxicam (Metacam; Boehringer Ingelheim) at 0.2 mg/kg was administered by subcutaneous injection. The endotracheal tube was removed following a clear return of the palpebral reflex, but prior to the return of the swallowing reflex. Cats were continuously monitored in the postoperative period until they were normothermic and able to maintain sternal recumbency independently. Active warming, using a heat pad beneath the bedding, was implemented until rectal temperature was >37.0°C. A second dose of buprenorphine at 0.02 mg/kg was administered sublingually at the time of discharge; the time of this administration was noted.
Surgical protocols
Final-year undergraduate students were allocated to cases prior to revealing the approach to eliminate bias, with students encouraged to prepare for surgery by familiarising themselves with the standardised method for both flank and midline OVE. All surgeries were performed by the student under the direct and continuous supervision of a veterinary surgeon who was scrubbed into the procedure. Prior to surgery, the urinary bladder of the cat was manually expressed. Cats were placed in dorsal or right lateral recumbency, depending on the approach allocated, and routinely prepared for aseptic surgery. Following surgery an Elizabethan collar was placed on all cats to prevent interference with the surgical site.
Flank approach
Cats were placed in right lateral recumbency with legs extended caudally. An equilateral triangle was visualised with vertices at the greater trochanter, wing of the ilium and mid-point of the proposed incision. 12 Skin incisions were standardised at 15 mm using the marker on a sterile scalpel handle to ensure consistency. The abdominal cavity was entered by sequentially incising the skin, subcutaneous fat, external aponeurosis, internal and transverse abdominal oblique muscles, and peritoneum in a dorsal-to-ventral direction. The uterus was identified and the left ovary exteriorised. The left mesovarium was fenestrated and a three-clamp technique used to isolate the vasculature of the ovarian pedicle. A single ligature was placed immediately below the haemostatic forceps using two metric polyglycolic acid (Vicryl; Ethicon) before transection between the clamps. The ovarian pedicle was grasped using rat-toothed forceps to ensure appropriate haemostasis prior to release. The three-clamp technique was repeated on the uterine horn in close proximity to the proper ligament. A single two-metric polyglycolic acid ligature was placed distal to these. The uterine horn was transected between the clamps and the ovary removed. The uterine horn was followed to the bifurcation to exteriorise the contra-lateral horn, and the procedure repeated. All sites of transection were checked prior to closing to ensure adequate haemostasis. The muscle layers were apposed and closed using two-metric polydioxanone (PDS II; Ethicon) in a simple continuous pattern. The subcutaneous layer and skin were each apposed and closed using two metric poliglecaprone 25 (Monocryl; Ethicon) in a simple continuous appositional and simple continuous intradermal pattern, respectively.
Midline approach
Cats were placed in dorsal recumbency. A 25 mm skin incision was made directly caudal to the umbilicus. Subcutaneous fat was sharply incised to expose the linea alba. The linea alba was tented using rat-toothed forceps and a small stab incision made through the linear alba and peritoneum using an inverted scalpel blade. The incision was extended caudally and cranially until it was the same length as the skin incision. Following identification of the reproductive tract, the OVE and wound closure was performed as described for the flank approach.
Data collection
Six veterinary surgeons participated in the study, all of whom were trained in the study protocol by the lead assessor prior to participating. All assessments were performed by the same veterinary surgeon on the day of surgery. Heart and respiratory rate, as well as a pain score using the Colorado State University Feline Acute Pain Scale (FAPS; see Appendix 1 in the supplementary material) at the proposed site of surgery, were recorded after the cat had been settled in the hospital for at least 30 mins but prior to the administration of any of the premedication drugs. Cats were assigned a FAPS score of 0–4 by assessing psychological and behavioural signs, response to palpation and body tension. If the distribution of scores for individual components of the scale overlapped two pain scores, the overall score was moderated by half a point so that it fell between the two. Duration of surgery and anaesthesia, as well as any intraoperative complications, inclusive of hypotension, haemorrhage, slipping of ligatures or break in aseptic technique, were recorded.
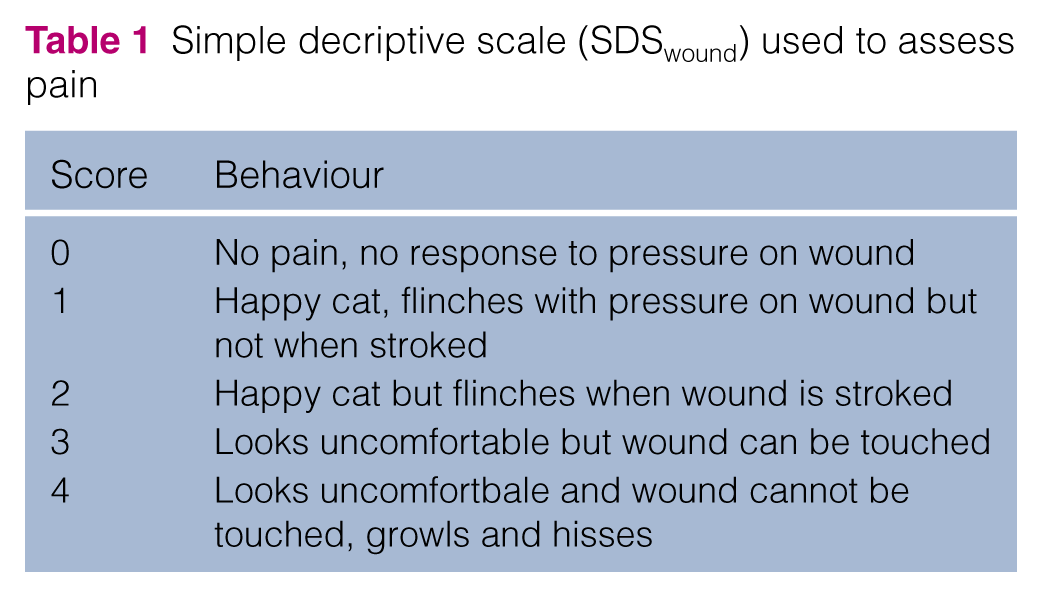
Cats were assessed 1 h postoperatively and at the time of discharge (exact time noted) for pain and wound tenderness using the FAPS, a simple descriptive scale (SDSwound; Table 1), 13 and a dynamic and interactive visual analogue scale (DIVAS) using a 100 mm line anchored by ‘no pain’ and ‘worst pain imaginable’. A DIVAS score was assigned by firstly observing the behaviour and posture of the cat within the kennel prior to being disturbed. Secondly, behaviour and reaction were observed when the cat was approached, spoken to and the kennel door opened, with the cat being handled, petted and gently stroked. Finally, gentle digital pressure was applied to the incision site and surrounding skin. A mark was placed on the DIVAS line corresponding to the behaviour of the cat. 14 Swelling of the surgical wound was assessed with the simple descriptive scale (SDSswelling) used in the study by Muir et al (Table 2), 15 and a 100 mm visual analogue scale (VASswelling) anchored by ‘no swelling associated with surgical wound’ and ‘worst possible swelling associated with surgical wound following OVE’. Other wound parameters monitored were discharge from the wound using a 100 mm visual analogue scale (VASdischarge) anchored by ‘no discharge’ and ‘continuous discharge’. Any discharge was characterised as either serous, serosanginous, haemorrhagic or purulent. Periwound erythema was assessed using a 100 mm visual analogue scale (VASerythema) anchored by ‘no erythema’ and ‘worst possible erythema following OVE’. The same pain score and wound parameters were assessed again at the 3 day and 10 day postoperative re-examinations. However, it was not always possible for the same veterinary surgeon that had assessed the cat on the day of surgery to perform the re-examination.
Simple decriptive scale (SDSwound) used to assess pain
Simple decriptive scale (SDSswelling) used to assess swelling

Statistical analysis
Power calculations by Polson et al indicated that 25 cats in each group would achieve 90% power to detect clinically relevant differences in pain scores (DIVAS 10 mm, SDS 1). 16 Additional cats were recruited over the study period in an effort to maximise the numbers returning for postoperative reassessment. For final statistical analysis, data were grouped as described below. As statistically significant differences were observed, post-power calculations were not performed.
Normality of continuous numerical variables was assessed using the Shapiro–Wilk test. For continuous variables, median (range) or mean ± SD were reported; for ordinal and categorical variables, frequency and percentage were reported. Age was compared using the Mann–Whitney U-test. Duration of anaesthesia and surgery, and time to discharge were compared using the Student’s t-test. Most of the VAS and DIVAS scales were skewed, and data were categorised as 0, 1–50 or 51–100 for analysis. χ2 test for trend, or Fisher’s exact test were used to assess differences in SDS and (DI)VAS measures between the two treatment groups. Analysis was carried out in SPSS (IBM), with significance level set at 5%.
Results
Seventy-five cats were enrolled into the study; 38 in the flank group and 37 in the midline group. Age did not vary significantly between groups (P = 0.49). Table 3 summarises population data, duration of anaesthesia and surgery, and time to discharge. Where data are normally distributed the mean ± SD are reported; for skewed data median (range) are reported.
Summary of age, duration of surgery and anaesthesia, incidence of hypotension and time from surgery until discharge
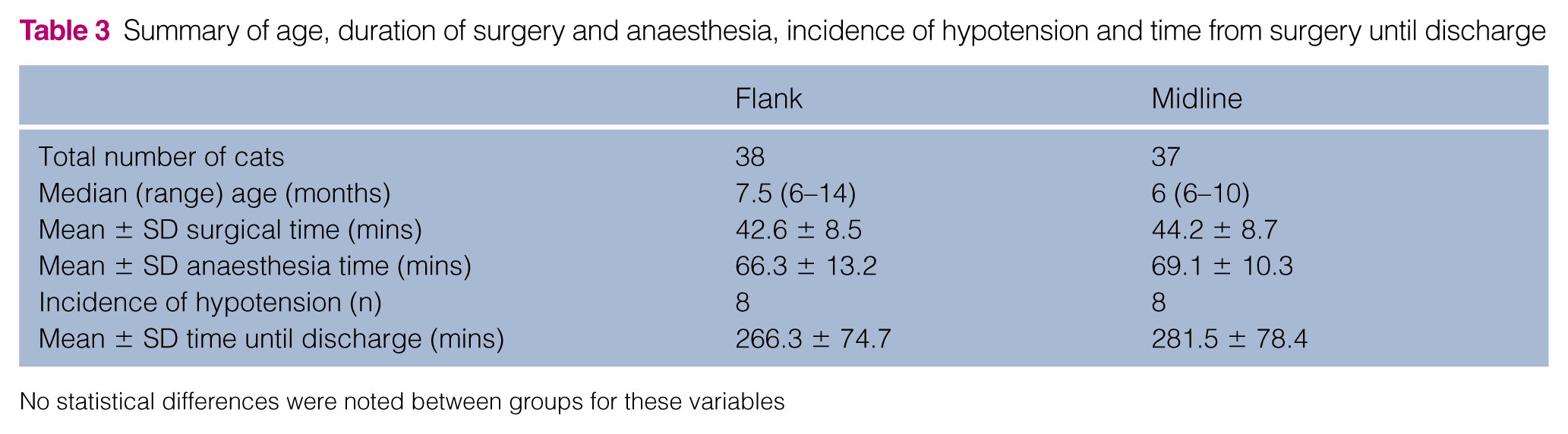
No statistical differences were noted between groups for these variables
There was no statistical difference in duration of anaesthesia (P = 0.84) or surgery (P = 0.78) between the two groups. Sixteen cats (eight in each group) had a mean blood pressure <60 mmHg during anaesthesia that was responsive to a single IV 10 ml/kg bolus of lactated Ringer’s solution. No other intraoperative complications, including bleeding from the uterine or ovarian pedicles, were reported for either group. There was no statistical difference in the need for an IV fluid bolus between the flank or midline approach (P = 0.48).
There was no statistical difference in FAPS scores between groups prior to surgery (P = 0.125; Figure 1). Both groups demonstrated statistically higher FAPS scores at 1 h after surgery compared with before surgery (P = 0.0002), with the FAPS scores of the flank group being significantly higher compared with the midline group (P = 0.0004) at 1 h after surgery. SDSwound (P = <0.0001; Figure 2) and DIVAS (P = 0.0002; Figure 3) scores were also significantly higher in the flank group compared with the midline group at 1 h after surgery. VASswelling (P = 0.299; Figure 4) and SDSswelling (P = 0.178; Figure 5) scores did not vary significantly between approaches. Seven cats in the flank group and six cats in the midline group had mild erythema associated with their surgical wounds, with no statistical significance noted between approaches (P = 1). There was no statistical difference in wound discharge between the groups (P = 0.432).

Summary of Feline Acute Pain Scale (FAPS) scores at all time points between groups, displayed as the percentage of cats with each score. Statistically significant differences were noted at 1 h after surgery (P = 0.0004), time of discharge (P = 0.002) and at both the 3 day (P = 0.016) and 10 day (P = 0.045) re-examinations
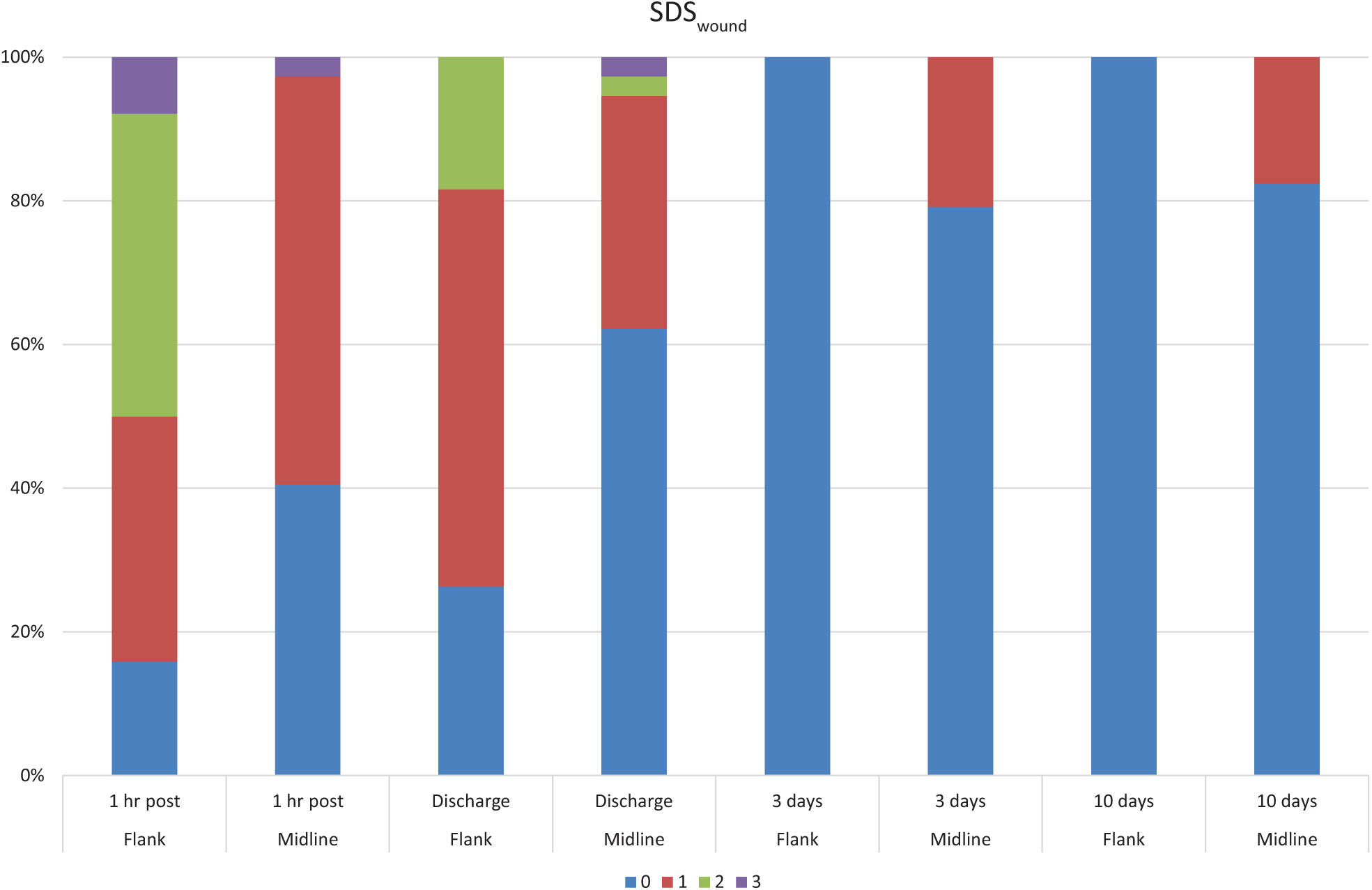
Summary of simple descriptive scale for pain and wound tenderness (SDSwound) scores at all time points between groups, displayed as percentage of cats with each score. Statistically significant differences were noted at 1 h after surgery (P <0.0001), time of discharge (P = 0.005) and at the 3 day (P = 0.05) re-examination

Summary of dynamic and interactive visual analogue scale (DIVAS) scores at all time points. For statistical analysis and presentation, DIVAS scores were categorised as 0, 1–50 and 51–100. Percentage of cats within each category for flank and midline groups are shown. Statistically significant differences were noted at 1 h after surgery (P = 0.0002), time of discharge (P = 0.001) and at the 3 day (P = 0.05) re-examination

Summary of swelling visual analogue scale (VASswelling) scores at all time points. For statistical analysis and presentation, scores were categorised as 0, 1–50 and 51–100. Percentage of cats within each category for flank and midline groups are shown. Statistically significant differences were noted at both the 3 day (P = 0.0004) and 10 day (P = 0.0001) re-examinations
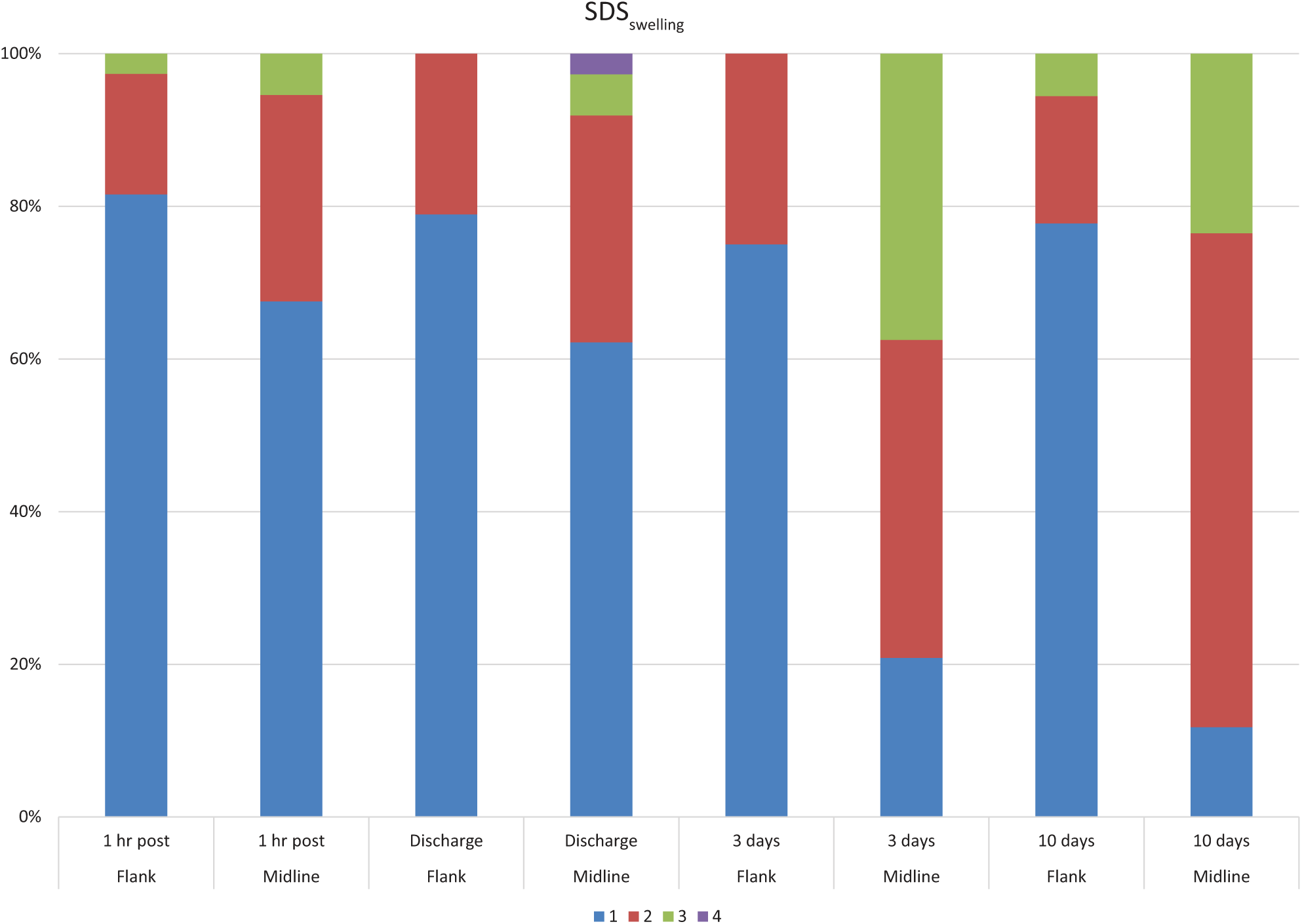
Summary of simple descriptive scale for wound swelling (SDSswelling) scores at all time points between groups, displayed as percentage of cats with each score. Statistically significant differences were noted at discharge from hospital (P = 0.048), and at the 3 day (P <0.0001) and 10 day (P = 0.001) re-examinations
There was no significant difference in time from surgery to discharge between the groups (Table 3). At the time of discharge cats in the flank group had significantly higher FAPS (P = 0.002), SDSwound (P = 0.005) and DIVAS (P = 0.001) scores compared with the midline group. Cats in midline group demonstrated more swelling at discharge when comparing SDSswelling scores (P = 0.048) but not VASswelling scores (P = 0.051), with 37.8% of cats in the midline group being categorised as having grade 2 swelling or greater using the SDSwound criteria vs 21.1% in the flank group. Wound discharge (P = 1) and erythema (P = 0.516) did not vary significantly at this time point.
Forty-eight cats (68%) returned for their scheduled 3 day postoperative re-examination; 24 cats from each group. Cats in the midline group had significantly higher FAPS (P = 0.016), SDSwound (P = 0.05) and DIVAS (P = 0.05) scores compared with the flank group. There was significantly more wound swelling in the midline group when comparing both SDSswelling (P <0.0001) and VASswelling (P = 0.0004) scores with the flank group. Nineteen cats (72.9%) in the midline group that presented for re-examination had an SDSswelling score of ⩾2 vs six cats (25%) in the flank group. Wound discharge (P = 1) and erythema (P = 1) did not vary significantly between the groups.
Thirty-five cats (46.7%) presented for their scheduled 10 day postoperative re-examination; 18 from the flank group and 17 from the midline group. Cats in the midline group had significantly higher FAPS scores (P = 0.045) compared with the flank group, but SDSwound and DIVAS scores were below the 5% significance level (P = 0.104). There was significantly more swelling associated with the midline approach for both SDSswelling (P = 0.001) and VASswelling (P = 0.0001). Fifteen cats (88.2%) in the midline group that presented for re-examination at 10 days had an SDSswelling score of ⩾2 compared with four cats (22.5%) in the flank group. A single cat in the midline group was observed to have mild erythema associated with the wound, and two cats in this group were noted to have mild serous discharge. No cats in the flank group had any wound-associated erythema or discharge; however, this was not statistically significant (VASdischarge P = 0.229; VASerythema P = 0.486). No cat was reported to have a wound breakdown or infection, and there was no requirement for open wound management, antibiotics, further analgesia or surgical revision apart from one cat from the midline group that was erroneously prescribed antibiotics at the 3 day postoperative re-examination appointment due to seroma formation (wound swelling).
Discussion
A clear preferred approach for OVE in the cat is not apparent from the results of this study. Surgical and anaesthetic duration, and intraoperative complications did not vary significantly between groups. Interestingly, surgical duration of OVE in this study was directly comparable with a previous study comparing flank and midline approaches for OVH, also performed by final-year veterinary students (flank OVE 42.6 mins vs OVH 41.1 mins; midline OVE 44.1 mins vs OVH 43.8 mins). 8 When performed by an experienced surgeon the difference in surgical time between flank and midline approaches for both OVH and OVE is also likely to be negligible.
Signs of pain in cats are often subtle and can be hard to appreciate.17,18 In this study the inclusion of a DIVAS and FAPS to assign postoperative pain scores was used in addition to the SDSwound to try and maximise sensitivity.17,18 While the strength of this study could have been improved by blinding the assessor from the surgical approach through abdominal bandaging, this was found to cause significant alterations in behaviour, making pain scoring impossible in a previous study, 11 and thus was not performed. In this study the FAPS, SDSwound and DIVAS scores following OVE surgery up to discharge the same day were consistent with previous studies showing higher pain and wound palpation scores in cats following a flank vs midline approach for OVH performed by veterinary students,10,11 but not with the only study comparing pain scores in cats undergoing OVE, which found no significant difference between flank or midline approaches. 3 It is possible that the lack of difference in the latter study could be explained by the use of morphine in the premedication instead of buprenorphine, and that an experienced surgeon was performing the procedures. Our findings were also consistent with another previous study of cats undergoing OVH (approach not clarified but assumed to be flank) by UK veterinary students which found that the administration of meloxicam immediately following surgery did not prevent postoperative wound tenderness up to 24 h. 19
Most previous studies have not monitored postoperative discomfort beyond 24 h.3,10,11,19 One study relied on an owner questionnaire at 7 days, which asked ‘How much discomfort did you feel your cat experienced after the operation?’, with no difference reported between cats undergoing OVH by a midline or flank approach. 8 Another study, investigating owner perceptions of postoperative discomfort and behavioural changes following OVH (approach not specified), demonstrated perceivable changes that could be the result of pain for the 3 days following surgery. 20 In this study, the significantly higher pain scores reported in the flank group the same day as surgery was reversed when the cats were re-examined by a veterinary surgeon at 3 and 10 days postoperatively, with cats in the midline group demonstrating significantly higher FAPS, SDSwound and DIVAS scores at 3 days, and significantly higher FAPS scores at 10 days. As SDSwound and DIVAS were not significantly different at 10 days postoperatively, it is difficult to say whether difference in discomfort was clinically significant between groups. Owners were encouraged to bring back their cats for both re-examination appointments; however, bias may have been introduced at this stage, with owners only re-presenting if they were concerned by behavioural changes or obvious swelling associated with the surgical wound. Therefore, it is impossible to say with certainty if cats re-examined were representative of the population as a whole, and if all cats had re-presented, whether FAPS scores would have been significantly different between groups. A single study investigating the use of non-steroidal anti-inflammatory drugs (NSAIDs) following OVH in dogs concluded that postoperative comfort was improved for the 3 days following surgery when these medications were administered compared with a control group. 21 Given that cats are also likely to experience discomfort following OVE, with evidence that behavioural changes can be observed in the first 3 days following surgery, the use of an extended course of oral NSAID should be considered for at least this time period following OVE.20,22
Significant limitations of the long-term follow-up performed in this study include the declining proportion of cats returning for the 3 day and then 10 day re-examinations and that it was not possible to have a single assessor conduct all postoperative wound assessments, even for the same cat. Six veterinary surgeons participated in the study, all of whom were trained in the study protocol by the lead assessor prior to participating. For future work investigating postoperative discomfort following feline OVE the use of a validated composite measure pain score tool, such as that developed by Calvo et al, 18 is likely to be preferential to reduce variability between assessors.
Cats in the midline group may have had a tendency for higher pain and wound tenderness scores at postoperative re-examination appointments owing to the increased swelling that was also noted in this group, with SDSswelling scores being significantly higher in the midline group at the time of discharge, as well as at the 3 day and 10 day postoperative re-examinations. However, veterinary re-examination of the cats that returned did confirm no wound breakdown or infection, although one cat in the midline group had antibiotics erroneously administered owing to the presence of a seroma (wound swelling). Wound inflammation in cats following OVH is low (6% in one study of 312 cats), with cats undergoing midline OVH vs flank OVH having significantly more wound inflammation when the cats were <12 weeks but not when they were >12 weeks of age. 23 Another study that relied on an owner questionnaire at 7 days to grade postoperative wound swelling reported no significant difference between cats undergoing OVH by a midline or flank approach. 8 However, swelling following midline coeliotomy OVH in cats is a recognised complication in other studies.15,24,25Swelling following midline coeliotomy OVH in cats appears to occur independently to the type of suture material used. 24 Poliglecaprone 25 was chosen for this study for subcutaneous and intradermal closure owing to its relatively short lived inflammatory response in the feline linea alba. 25 There is conflicting evidence in the literature as to whether the inclusion of a subcutaneous closure affects the incidence of postoperative wound swelling, with Freeman et al advocating subcutaneous closure for midline OVH, 24 and Muir et al reporting less swelling when the subcutaneous layer was not closed. 15 Closure of the subcutaneous tissues was included in this study for additional security of the incision line and to provide a further barrier to dehiscence if the skin sutures are removed by the cat, as recommended by Langley-Hobbs. 26 In this study only direct midline dissection, with no subcutaneous dissection on either side of midline, was performed so as to minimise the potential for seroma. As outlined above, significant limitations of the long-term follow-up performed in this study include the reducing proportion of cats returning for the 3 day and then 10 day re-examinations and that it was not possible to have a single assessor conduct all postoperative wound assessments. Additionally, the results from this study, in which the surgery was performed by veterinary students, may not be directly applicable to the situation in general practice. Higher rates of wound infection have been reported in procedures performed by inexperienced surgeons, with longer surgery times and rougher tissue handling cited as the cause. 27
Conclusions
There appears to be no strong reason based on similar surgical or anaesthetic times, and varying perioperative pain and wound parameters between approaches, for advocating a preferred surgical approach for feline OVE within a teaching environment. Cats in the flank group had higher pain scores and wound tenderness until the point of discharge, while cats in the midline group had a higher incidence of postoperative wound swelling and discomfort at 3–10 days. It may be prudent to discharge all cats with a 3 day course of an oral non-steroidal anti-inflammatory drug following OVE to ensure postoperative comfort and reduce the incidence of swelling.
Supplemental Material
Appendix 1
Colorado State University Feline Acute Pain Scale
Footnotes
Acknowledgements
The authors would like to thank the staff, students and cat owners from the Beaumont Sainsbury Animal Hospital for their assistance, cooperation and participation in this study. Thanks are also due to Dr Ruby Chang and Dr Jake Bayley for their assistance with statistical analysis.
Author note
This paper was presented, in part, at the Australian and New Zealand College of Veterinary Scientists Science Week 2015.
Supplementary material
The following file is available online:
Appendix 1: Colorado State University Feline Acute Pain Scale.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.