
Abstract
The absorption of medetomidine released by continuous infusion from an osmotic pump in the abdominal cavity was studied in pregnant sheep during the 24 h postoperative period. Additionally pain and sedation was assessed. Eleven sheep were studied: six were treated with a medetomidine loaded osmotic pump delivering 10 μL/h (3 μg/kg/h medetomidine); and five with a saline loaded osmotic pump (control). Serial blood samples were taken and analysed to determine plasma medetomidine levels. Medetomidine was absorbed from the peritoneal cavity and a steady plasma concentration was achieved within 10 h, mean (SD) peak concentration was 2.87 (0.22) ng/mL. Sheep receiving medetomidine analgesia had significantly lower pain scores at 10 h than controls. Four control sheep required rescue analgesia, compared with 0 in the treatment group. Delivery of 3 μg/kg/h medetomidine by an intraperitoneal osmotic pump to pregnant sheep in the 24 h postoperative period provides adequate plasma concentrations of medetomidine for analgesia without sedation.
The Australian code of practice for the care and use of animals for scientific purposes states that pain management appropriate to the species, the procedure and the circumstances must be provided. 1 This remit is difficult to achieve in some species as there may not be sufficient evidence to apply safe and effective analgesic strategies. Pregnant sheep are used in a range of medical research projects but providing appropriate analgesia is challenging as there is a paucity of data in the literature. The challenge in providing anaesthesia and analgesia for pregnant sheep lies in the selection of a combination of drugs that do not cause adverse effects to either the ewe or the fetus. In the perioperative period, analgesia can be provided by administering drugs from the following drug classes: opioids; non-steroidal anti-inflammatory drugs (NSAIDs); local or regional anaesthetic drugs; α2 adrenoreceptor agonist drugs; and other miscellaneous drugs such as ketamine and tramadol.
The analgesic efficacy of opioids in sheep is controversial and there is little convincing data to support their use for acute surgical pain. There is a significant body of evidence regarding the danger of NSAID use in pregnant women and theoretically these drugs may cause premature closure of the ductus arteriosus, which may be fatal for the fetus in utero.2,3 Local anaesthetic drugs have been commonly used in sheep to provide regional anaesthesia and analgesia 4 but they are not devoid of significant cardiopulmonary side-effects and may also cause temporary paralysis of the hindlimbs when administered by the epidural route. 5 α2 adrenoreceptor agonists are commonly used to provide analgesia and anaesthesia in a number of species including sheep. Xylazine has been extensively studied after administration by a number of different routes: intramuscular; 6 intravenous; 4 epidural. 4 It is known that α2 adrenoreceptor agonists are associated with a number of dose-dependent side-effects: hypoxaemia; peripheral vasoconstriction; bradycardia and uterine muscle contraction. These side-effects are associated primarily with α1 adrenoreceptor stimulation. Xylazine has an α2:α1 ratio of 160:1 and is registered for use in sheep in Australia; however, medetomidine is more specific for the α2 adrenoreceptor (ratio 1620:1). 7 Hypoxaemia is an important side-effect seen following the use of α2 adrenoreceptor agonists in sheep. The exact mechanism of developing hypoxia is not fully known. It is thought to be attributed to a peripheral effect independent of its sedative effect. 8 Despite the potential for significant cardiopulmonary side-effects, the analgesic properties of α2 adrenoreceptor agonists hold promise for the provision of perioperative analgesia in pregnant sheep. We aimed to investigate the absorption of medetomidine from the abdominal cavity of pregnant sheep in the postoperative period.
Materials and Methods
Animals
Eleven adult merino, singleton ewes at 128 days’ gestation (term = 150 days) underwent general anaesthesia for a laparotomy and hysterotomy for instrumentation of the fetus as part of a series of studies approved by the animal ethics committee at the University of Western Australia. This study was performed as an adjunct study and was approved by the animal ethics committees of both the University of Western Australia and Murdoch University, according to the guidelines of the National Health and Medical Research Council of Australia code of practice for the care and use of animals for scientific purposes.
Preoperative management
All sheep were housed in a purpose-built large animal research facility. Two days prior to surgery the sheep were weighed and then moved from a communal raised pen to individual raised pens with open front and sides. Sheep were housed with at least two other sheep in the room at all times. A diet of oaten chaff was given to all sheep and water was offered ad libitum.
Anaesthesia
Anaesthesia was induced with xylazine (0.5 mg/kg, Xylazil-20, Ilium Veterinary Products, Troy Laboratories Pty Ltd, Glendenning, NSW, Australia) and ketamine (20 mg/kg, Ketamil, Ilium Veterinary Products, Troy Laboratories Pty Ltd) by intramuscular injection. The trachea was intubated (7.5 mm internal diameter, cuffed, Portex Ltd, Ashford, Kent, UK) and anaesthesia was maintained with isoflurane in 100% oxygen delivered through a circle breathing system. A line block of 100 mg ropivacaine (Naropin 1%, AstraZeneca, North Ryde, NSW, Australia) was performed along the laparotomy incision site prior to surgery. Electrocardiography, oxyhaemoglobin saturation, end-tidal CO2 and non-invasive blood pressure measurements were recorded by a dedicated anaesthetist throughout the procedure and any complications encountered were managed appropriately.
Surgery and pump placement
Sheep were positioned in dorsal recumbency and a midline abdominal incision allowed access to the uterus for hysterotomy and instrumentation of the fetus. Sheep were randomly assigned to a treatment group (n = 6) or a control group (n = 5). A 2 mL osmotic pump (Alzet osmotic pumps, Durect, Cupertino, CA, USA) releasing the drug at 10 μL/h was secured in a pocket of omentum at the end of surgery. Pumps were loaded aseptically with either 2 mL of sterile saline (control group) or medetomidine diluted with sterile saline to deliver 3 μg/kg/h (treatment group). Medetomidine (30 mg/mL, Zalopine, Orion Corporation, Espoo, Finland) loaded pumps were primed overnight at 37°C according to the manufacturer's instructions. An intravenous catheter was secured in the jugular vein to facilitate serial blood sampling in the postoperative period.
Postoperative management and data collection
Sheep were returned to their individual pens to recover from anaesthesia. The sheep were closely observed from the adjacent room and the time to standing was recorded for all animals. Blood samples were collected from sheep in the treatment group at 0, 1, 2, 3, 6, 10, 20 and 24 h and at 0, 3, 10, 24 h from those in the control group. Time 0 was the time the pump was positioned in the abdomen. The samples were collected into 10 mL glass ethylendiaminetetraacetic acid vacutainer tubes and were promptly centrifuged to separate the plasma. Plasma was transferred into Teflon coated glass vials for storage at –80°C.
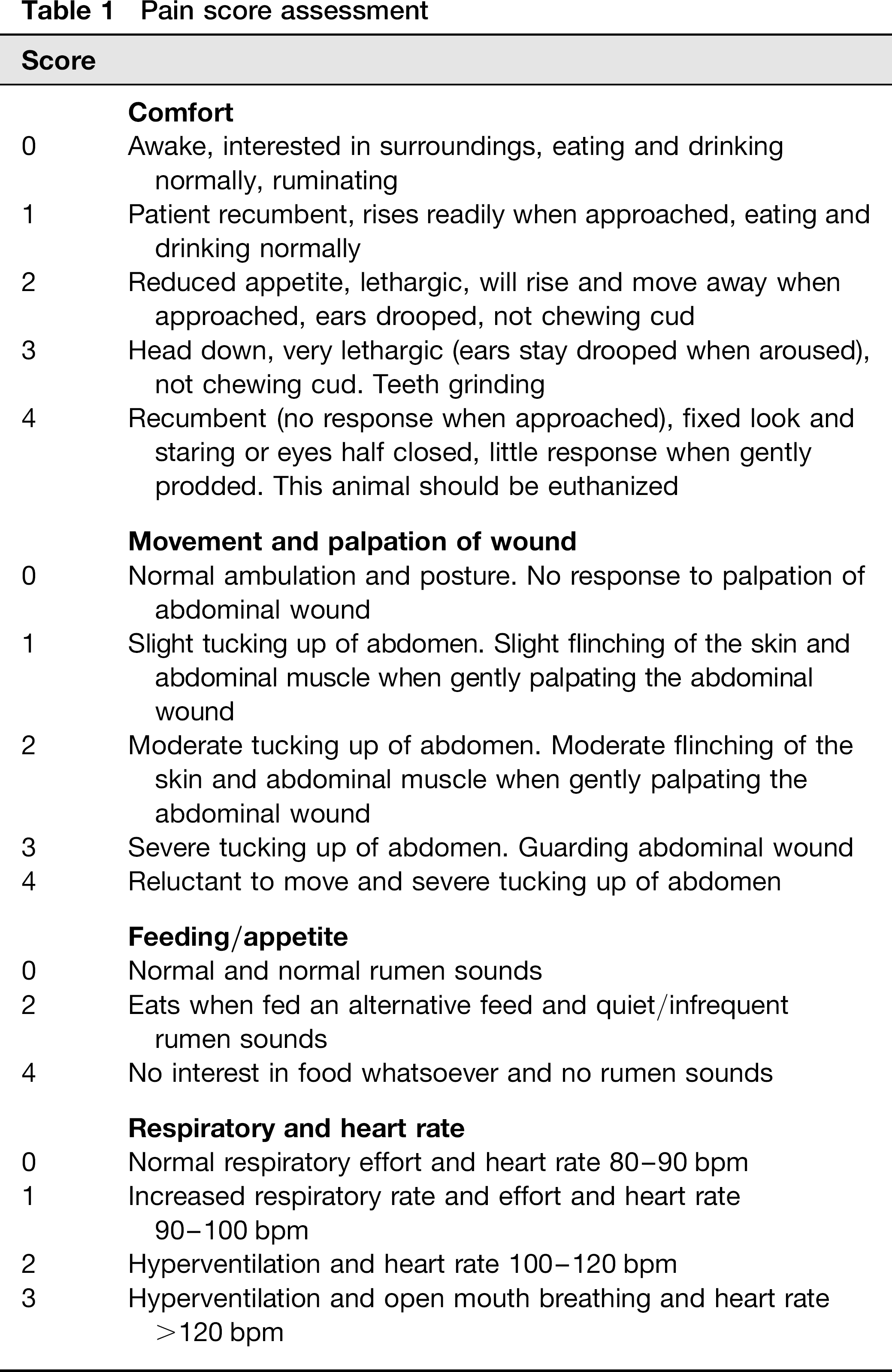
Pain and sedation scoring were performed by the same two, non-blinded individuals immediately prior to the collection of each blood sample. These scores were not recorded until the sheep was standing. Pain scoring addressed a variety of parameters including activity and palpation of the wound, comfort, feeding/appetite, rumen contractions, respiratory and heart rate (Table 1). Rescue analgesia, morphine 0.1 mg/kg every 4 h (DBL Morphine sulphate Injection BP 10 mg/ml, Hospira Australia Pty Ltd), was administered if the pain score was >5 (maximum 15).
Pain score assessment
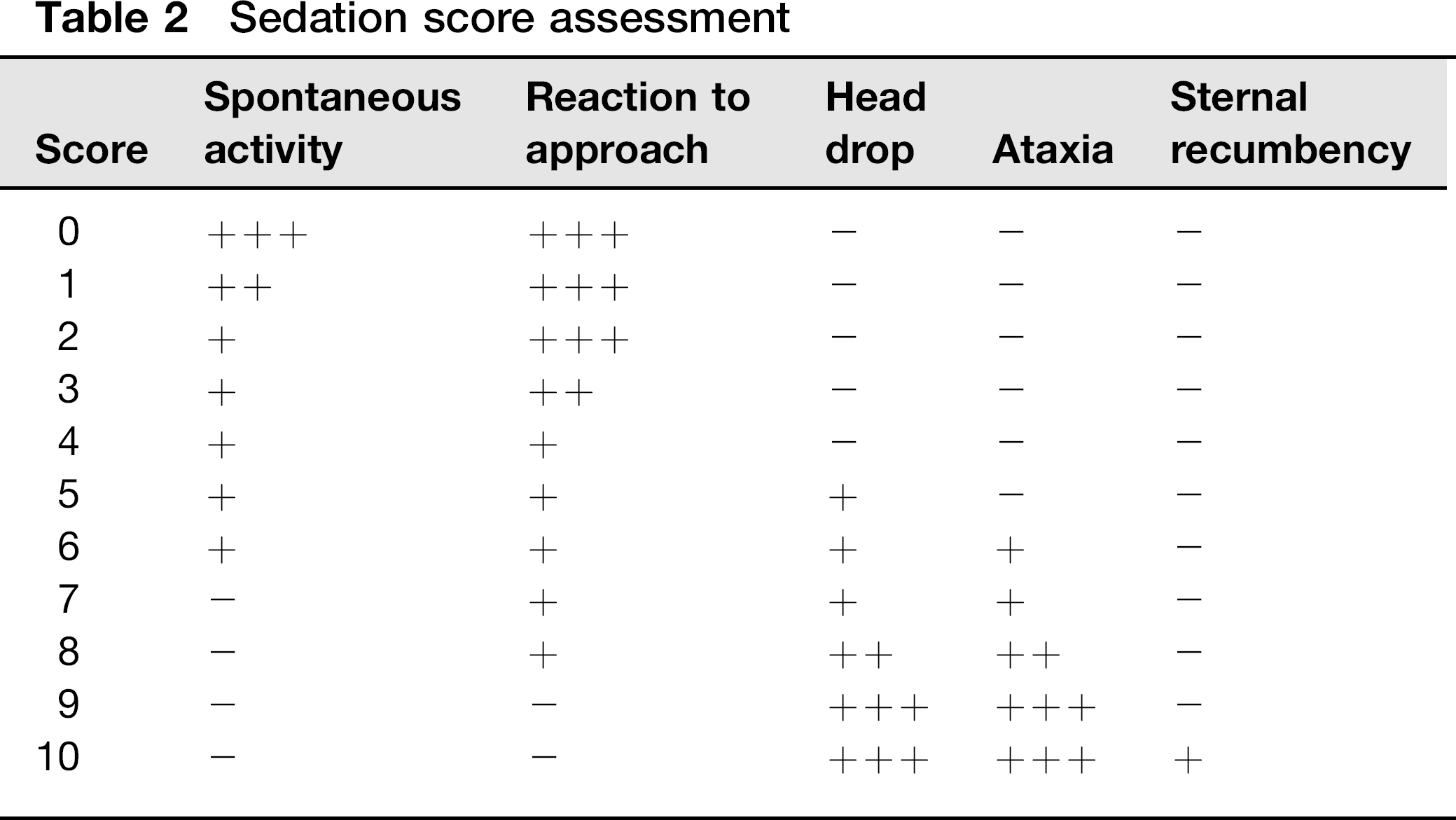
Sedation scoring also focused on a variety of parameters including spontaneous activity, reaction to approach, ataxia, head drop and sternal recumbency based on a modified sedation scoring system (Table 2). 9 If the sedation score was >10 (maximum 50), atipamezole 5 μg/kg (Antisedan 5 mg/mL, Pfizer Animal Health, Pfizer Australia Pty Ltd) was administered by intravenous injection to reverse the sedative effects of medetomidine.
Sedation score assessment
Sample analysis
Samples were prepared and analysed by a method previously described. 10 Plasma samples were extracted by solid phase extraction (SPE) using 30 mg Bond Elut Plexa (Varian Inc, Palo Alto, CA, USA) 1 mL cartridges. Standards and samples were injected individually in 1 μL volumes into an Agilent 1100 HPLC (Agilent Technologies, Santa Clara, CA, USA). The analytical column used was a Pursuit XRs Ultra diphenyl (Varian Inc) with dimensions of 30 mm × 2.0 mm × 3 μm. The HPLC was coupled to an Agilent Classic series ion trap mass spectrometer with an electrospray ionization source (Agilent Technologies) in positive ionization mode. Tandem mass spectrometry (MS/MS) of medetomidine was carried out using the transition m/z 201 → 95.
Statistical analysis
Data is expressed as mean (SD) unless otherwise stated. Serial data were compared between groups using two-way ANOVA with repeated measures (Sigmastat v12.0, SPSS Inc). Post hoc comparisons performed using the Holm-Sidak method (Sigmaplot version 12 [Systat Software Inc, San Jose CA, USA]). Correlations between plasma medetomidine concentrations and pain or sedation scores were conducted using a linear regression analysis. P < 0.05 was considered significant.
Results
There was a trend for lower live weight in the treatment group, 49.5 (4.18) kg compared with controls 60 (6.12) kg (P = 0.056). Sheep in the medetomidine group appeared to stand sooner after surgery than those in the control group (control: 156.8 [47.6] min, treatment: 125.8 [40.0] min), however this failed to reach significance (P = 0.317). All sheep began to eat and drink at a similar time and maintained normal feeding behaviour throughout the postoperative observation period.
The plasma concentration of medetomidine increased over the first 10 h in the treatment group and remained stable for the remainder of the study period (Figure 1). The mean peak concentration of medetomidine in the plasma was 2.87 (0.22) ng/mL. Medetomidine was not detected in the plasma collected from sheep in the control group at any time point.
Mean (SD) plasma medetomidine concentration •=medetomidine group, ○=control group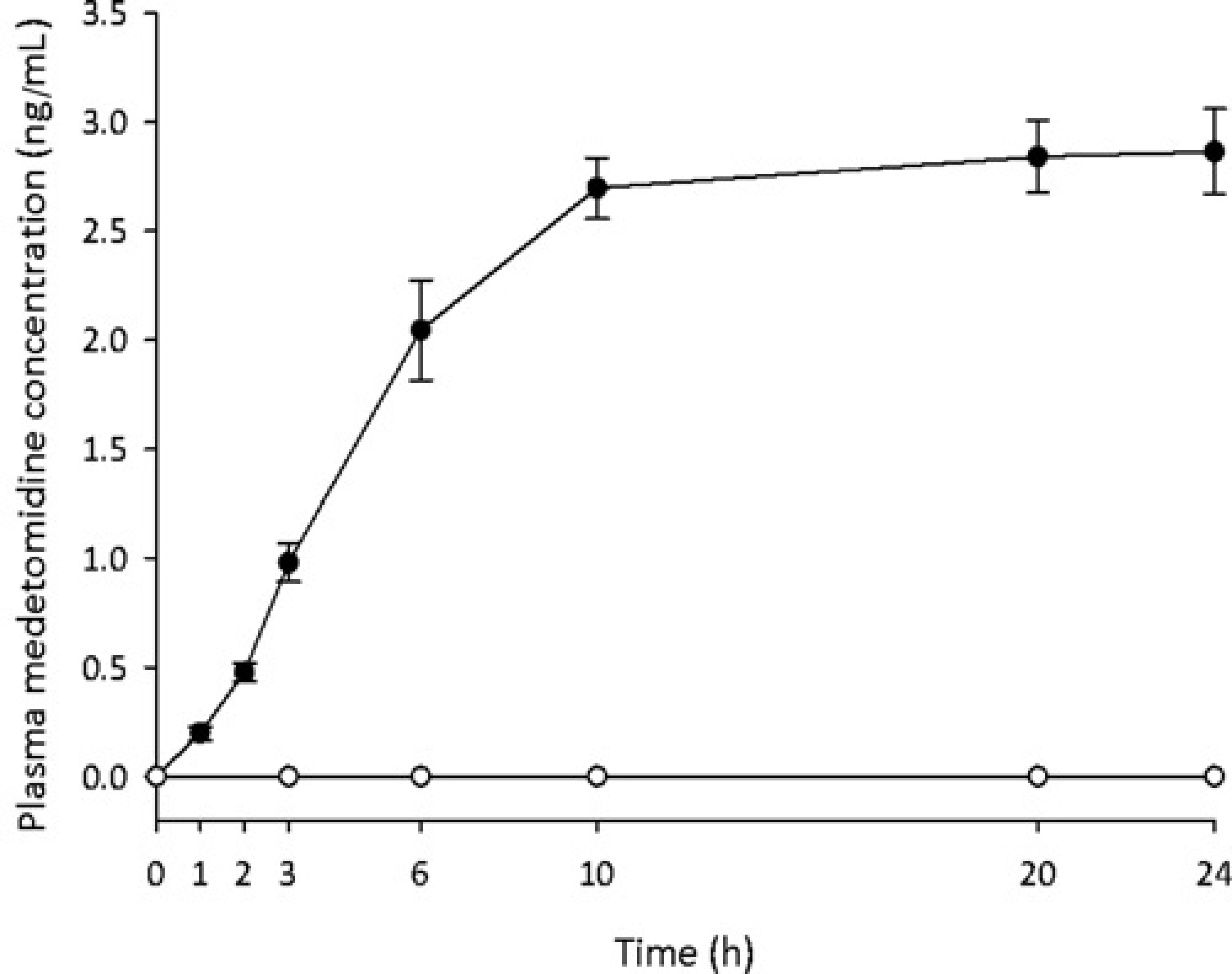
Sheep in the medetomidine group maintained a lower and more stable pain score than the control group. Control animals had a higher pain score at 10 h postoperatively than the medetomidine group (P = 0.046; Figure 2). No sheep in the medetomidine group required supplementary analgesia. Two of the four sheep in the control group required more than one dose of supplementary analgesia. There was no correlation between the pain score and the plasma medetomidine concentrations, meaning that no additional benefit was observed with higher plasma concentrations (Figure 3).
Mean (SD) pain score over time. •=medetomidine group, ○=control group, *P = 0.046 Pain scores and plasma medetomidine concentrations. •=medetomidine group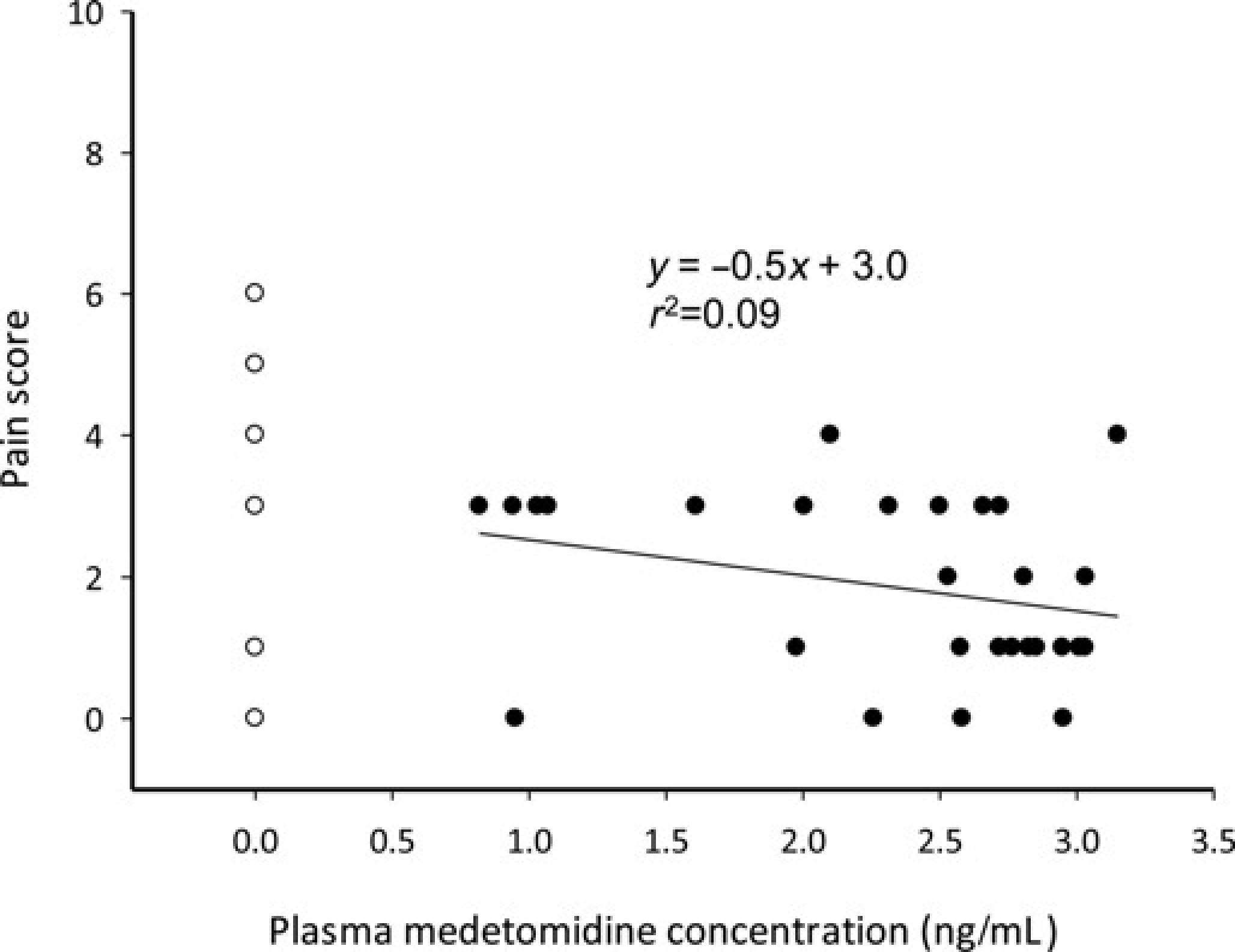
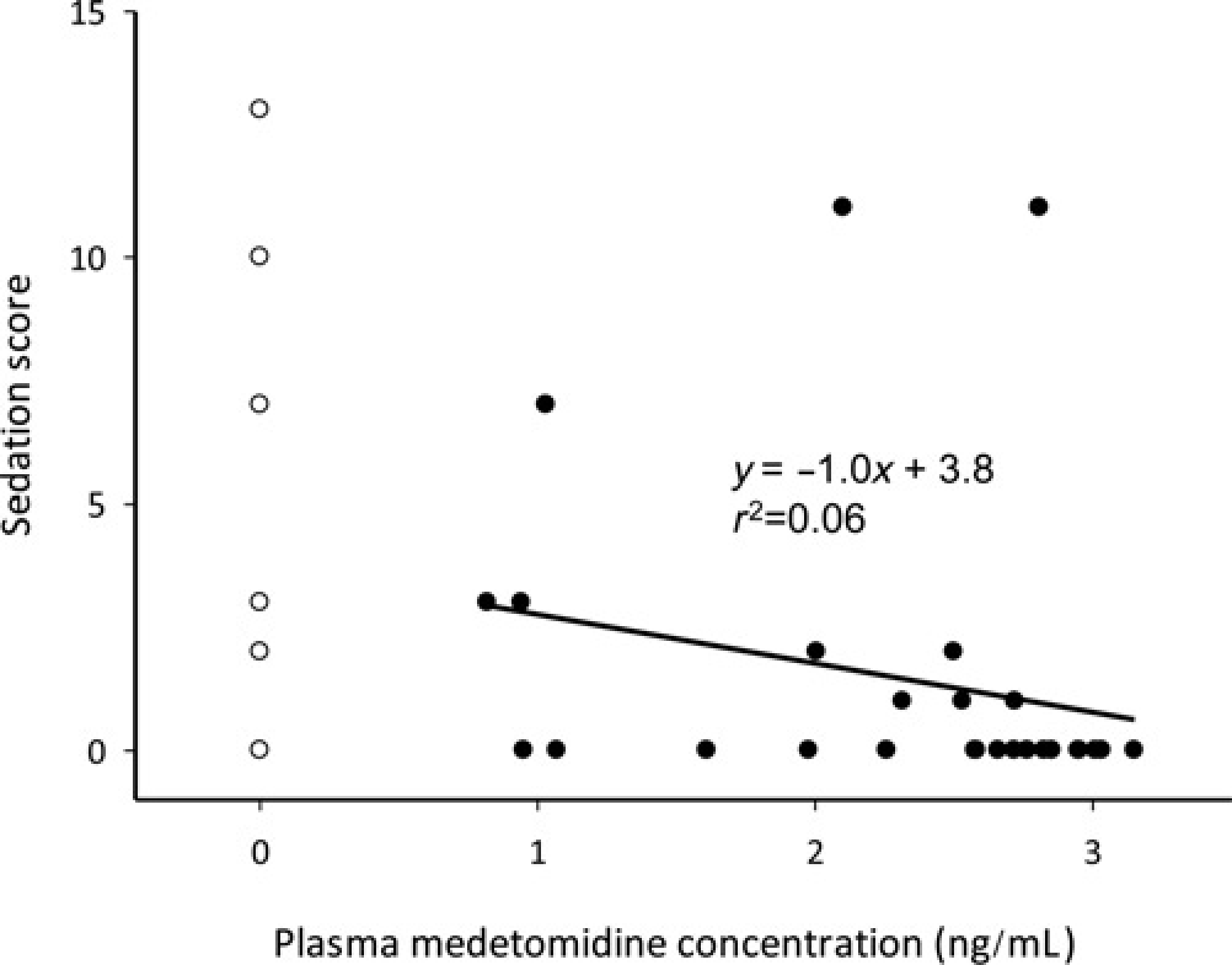
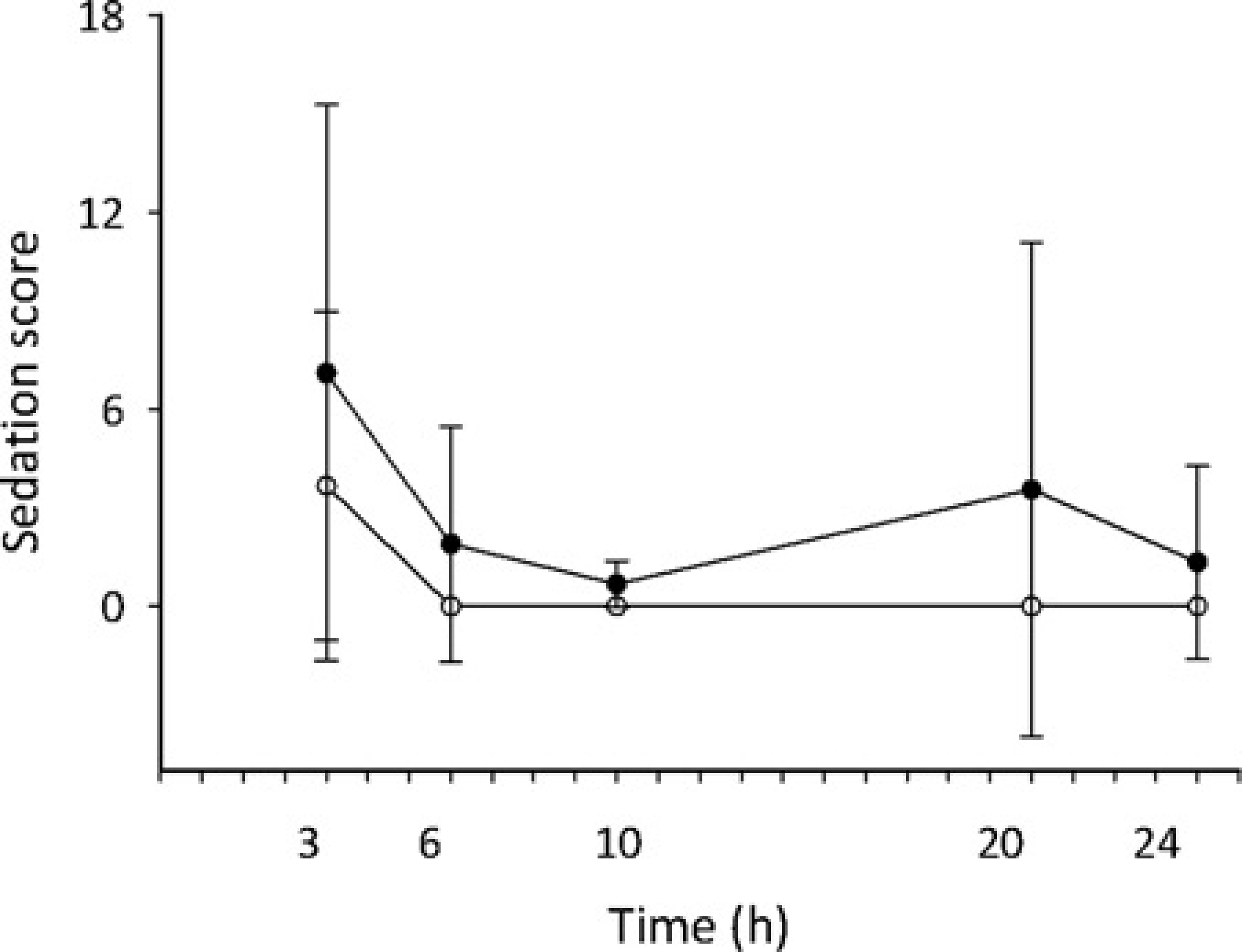
Sedation scores in both the treatment and control groups decreased over time (P = 0.010) and there was no difference in sedation scores between the groups (P = 0.813; Figure 4). There was no correlation between the sedation scores and the plasma medetomidine concentration (Figure 5). Only one sheep in the treatment group required administration of atipamazole at 3 h post-pump placement due to mild sedation, score 12 out of 50.
Sedation score and plasma medetomidine concentrations Mean sedation scores (SD) against time. •=medetomidine group, ○=control group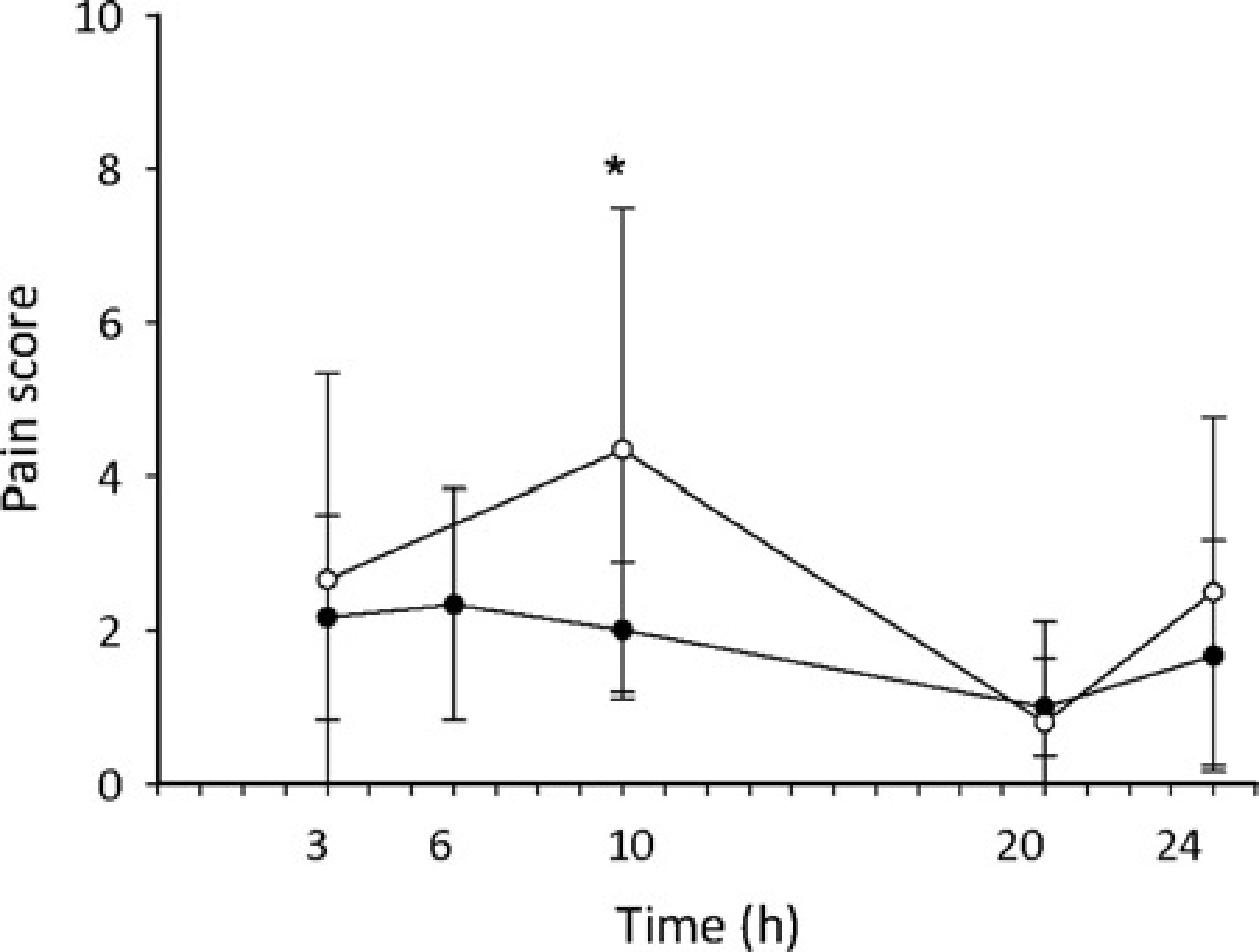
Discussion
Sheep are commonly utilized as an animal model in biomedical research, but the provision of perioperative analgesia is difficult. This study aimed to investigate the absorption of medetomidine when delivered by an osmotic pump into the abdomen of pregnant sheep. Furthermore, we aimed to determine whether intraperitoneal medetomidine provided analgesia, without sedation, in pregnant sheep in the immediate postoperative period.
Xylazine has been used extensively for analgesia for sheep in clinical 11 and research 12 environments. Prolonged analgesia from an α2 adrenoreceptor agonist, however, requires continuous delivery of the drug. To this end either repeated doses must be administered or intravenous access is required for drug infusion. The former approach will result in troughs and peaks of plasma concentration of a drug, and consequently an unstable clinical effect. The latter requires maintenance and care of an intravenous catheter which must remain aseptic, intact and patent. Vigilance over the catheter and drug administration equipment must be continuous to prevent infection, catheter emboli, haemorrhage or inadvertent drug overdose. We chose to investigate drug delivery via an osmotic pump to determine whether therapeutic plasma concentrations of medetomidine could be achieved and maintained at a stable concentration in the immediate postoperative period, without the labour required to care for an intravenous catheter. The osmotic pumps proved ideal in this regard as once they were positioned in the abdominal cavity they did not require ongoing care. The pumps used in this study are designed to release a constant rate of medication for a seven-day period. Longer and shorter duration pumps are also available. A potential issue, however, is that the administration of the drug cannot be easily terminated without surgical removal of the pump. The effects of leaving a pump in situ long term is unknown, as a foreign object it is anticipated that an inflammatory response will occur around the pump. In the authors’ experience, leaving pumps in situ for up to six days is not associated with any complications. The contingency plan for medetomidine overdose was the administration of atipamezole. Atipamezole is an α 2 adrenoreceptor antagonist and was available if required. At the dose of medetomidine used in this study, we did not observe excessive sedation and only one of the treatment group animals required atipamezole. Various studies document the pharmacokinetics of medetomidine in sheep following intravenous and intramuscular injections.9,13 Following intramuscular injection of 30 μg/kg of medetomidine the peak plasma concentration was 4.98 ng/mL, 9 while the peak plasma concentration following intravenous administration of medetomidine (15 μg/kg) was 23.52 ng/mL. 13 Sheep became heavily sedated when the plasma concentration of medetomidine was 5 ng/mL. 9 In our study, the mean peak plasma concentration of medetomidine was 2.87 ng/mL and heavy sedation was not observed.
There are a number of limitations to this study: as part of the anaesthesia protocol, all animals received a combination of drugs which have analgesic properties that may confound our assessment of postoperative pain; assessment of pain in sheep is difficult, as they are naturally prey animals which will hide pain to avoid attack; and although the mean pain scores decreased as the plasma concentration of medetomidine increased, the pain scoring tool we used has not been validated in this species. Furthermore, comparison of the pain scores between the two groups is difficult as animals received supplementary analgesia when their pain score was >5, reducing the pain scores seen in the control animals which received supplementary analgesia. Additionally, the number of animals in this study was small but for the purposes of demonstrating absorption of medetomidine from the abdominal cavity this sample size was adequate. Larger groups would be required to further investigate the analgesic and sedative effects of intraperitoneal medetomidine.
Conclusion
Medetomidine is absorbed from the peritoneal cavity of pregnant sheep when administered by an osmotic pump placed at the end of surgery. The administration of 3 μg/kg/h of medetomidine provided analgesia without significant sedation for the 24 h period following surgery. Further work investigating this postoperative analgesic strategy is warranted to determine whether it is safe and efficacious for longer periods of time. This can only be achieved with an improved understanding of pain assessment in sheep.
Footnotes
Acknowledgements
The Women and Infants Research Foundation is gratefully acknowledged for funding this study, as well as an NHMRC/NHFA Fellowship (GRP). We also appreciate the assistance of Large Animal Facility staff at the University of Western Australia.