
Abstract
Practical relevance:
Abdominal ultrasound plays a vital role in the diagnostic work-up of many cats presenting to general and specialist practitioners. Ultrasound examination of the liver can be key in the diagnosis of diseases such as hepatic lipidosis and hepatic neoplasia.
Clinical challenges:
Despite ultrasonography being a commonly used modality, many practitioners are not comfortable performing an ultrasound examination or interpreting the resulting images. Even differentiating between normal variation and pathological changes can be challenging for all but the most experienced. When assessing the liver via ultrasound, a diffuse alteration in liver echogenicity may be difficult to detect unless the change is marked and, although comparisons can be made with the spleen and kidneys, this relies on these organs being normal.
Equipment:
Ultrasound facilities are readily available to most practitioners, although use of ultrasonography as a diagnostic tool is highly dependent on operator experience.
Aim:
This review, the first in an occasional series on feline abdominal ultrasonography, discusses ultrasonographic examination of the normal and diseased liver, with focus on the liver parenchyma. It is aimed at general practitioners who wish to improve their knowledge of and confidence in feline abdominal ultrasound and is accompanied by high-resolution images. Ultrasound-guided sampling of the liver is also covered. Future articles will discuss the biliary tree and hepatic vascular anomalies.
Evidence base:
Information provided in this article is drawn from the published literature and the author’s own clinical experience.
Keywords
Scanning the liver and biliary tree
B-mode ultrasonography is probably the most widely used modality for imaging the feline liver. It provides information regarding the size, contour and echogenicity of the liver parenchyma while allowing the adjacent peritoneum, hepatic vasculature, biliary tree and hepatic lymph nodes to be evaluated in detail. 1
Where possible, it is usually preferable to fast animals waiting for an elective examination for 12 h prior to ultrasound to minimise the volume of ingesta and, in particular, gas within the gastrointestinal tract. Ultrasound cannot penetrate gas and hence structures deep to intestinal gas may be obscured. Water, on the other hand, should not be withheld and can actually improve organ visibility by providing an acoustic window. Some cats may be scanned while conscious. Nevertheless, sedation is preferable in most instances since it relaxes the abdominal wall muscles and helps to immobilise the patient. Preparation prior to scanning involves clipping the abdominal hair followed by the application of acoustic coupling gel to remove the air gap between the transducer surface and the skin.
Once the abdomen has been suitably prepared, the transducer is placed just caudal to the xiphisternum along the midline and orientated longitudinally relative to the long axis of the patient (Figure 1). Using a sweeping motion from left to right, the liver is initially scanned in the longitudinal plane. The transducer is then rotated by 90° and using the same sweeping action, but in a craniocaudal direction, the liver can be evaluated in the transverse plane.

The author’s preference when scanning the liver is to place the cat in right lateral recumbency. The transducer is then positioned on the midline and angled cranially under the rib cage with the head orientated longitudinally relative to the long axis of the cat. Rotation of the transducer through 90° allows the liver to be imaged in the transverse plane. A video showing the positioning and sweeping motion of the transducer when imaging the feline liver is available as supplementary material

Transducers used for feline abdominal ultrasound by the author. The transducer on the left is a microconvex type, easily recognised by its small, curved footprint. On the right, the linear transducer has a large, flat, rectangular footprint enabling it to provide excellent detail of superficial structures in the near field of the image

Normal appearance of the liver
The liver is located immediately caudal to the diaphragm, and cranial to the stomach and spleen on the left and the right kidney on the right. The interface between the diaphragm and the lung is seen as an echogenic, curvilinear line. 2 The feline liver is composed of a left lobe (subdivided into medial and lateral sublobes), a quadrate lobe, a right lobe (also subdivided into medial and lateral sublobes) and a caudate lobe (comprising caudate and papillary processes). 3
The normal feline liver has a uniform echogenicity, similar to that of the spleen (Figure 3) and right renal cortex, assuming the comparison is made at the same depth and using the same machine settings. There is a degree of individual variation between cats such that the liver can be slightly hyper- or hypoechoic to the renal cortex and even slightly hyperechoic to the spleen in some normal cats.1,2,4 It should also be noted that, in some normal cats, fat is deposited within the cortical tubular epithelium of the kidneys, causing an increase in renal cortical echogenicity on ultrasound (Figure 4). 5 This is more frequently observed in older, neutered male cats and can give the false impression of a hypoechoic liver if the liver and kidney are compared directly. 4

Ultrasound image comparing the echogenicity of the liver and the spleen. In this cat, both organs are similar in echogenicity. In the far field, the stomach is visible on the left and the colon, which contains gas, is on the right

Ultrasound image from an older, neutered cat. The kidney has a hyperechoic cortex (double arrow) resulting in enhanced corticomedullary definition. The cat had no evidence of renal disease and, therefore, one of the more likely differentials considered was fat deposition within the cortex
The feline liver has a coarse echotexture compared with the relatively smooth echotexture of the spleen. Cats often possess a large amount of fat within the falciform ligament, which has a coarser echotexture than that of normal liver. Falciform fat is typically isoechoic to hyperechoic relative to the liver parenchyma 2 (Figure 5), although obese (but otherwise clinically normal) cats may have a liver that is hyperechoic to falciform fat. 6 Failure to differentiate between hepatic parenchyma and fat within the falciform ligament can lead to a false diagnosis of hepatomegaly.


(a) Ultrasound image of the liver of an 11-year-old obese Siamese cat, produced with a microconvex transducer. The falciform fat is similar in echogenicity to the liver and could easily be mistaken for liver tissue. (b) Same image as (a) but with a dashed line to represent the junction between the liver and the falciform ligament. (c) Ultrasound image from the same cat produced with a linear transducer. The image resolution is improved and the liver is more readily distinguished from the falciform fat. (d) Normal liver in a 5-year-old male neutered domestic shorthair cat in normal body condition imaged with a linear transducer. The falciform fat is visible in the near field and can be distinguished from the liver by its relative hyperechogenicity
Portal and hepatic veins are visible throughout the liver in cats. As in the dog, portal vein wall composition is such that it appears echogenic when viewed from a wide range of beam–vessel angles (Figure 6). In contrast, the hepatic vein wall has a more distinct composition, rendering it a specular reflector; thus it only appears hyper-echoic when perpendicular to the ultrasound beam (Figure 7). 7 At non-perpendicular angles, the wall is no longer visible. Differentiation between the two types of vessel is also possible with the use of colour Doppler. Colour Doppler flow signal will depict flow directed towards the periphery of the liver in portal veins (Figure 6), and towards the centre of the liver in hepatic veins (Figure 7). Hepatic arteries and intrahepatic bile ducts are not normally visible unless pathologically dilated.

Normal ultrasonographic appearance of an intrahepatic portal vein. (a) B-mode ultrasound image showing the typical hyperechoic walls of a portal vein (arrows). (b) Colour Doppler confirms flow is towards the periphery of the liver (ie, from right to left)

Normal ultrasonographic appearance of intrahepatic veins. (a) The hepatic veins (arrowheads) are easily recognised by the absence of visible walls. However, as the vein on the right curves in a caudal direction, the walls become orientated perpendicularly to the direction of propagation of the ultrasound pulses. At this level the walls of the vein become visible (arrows). (b,c) A single hepatic vein is visible in the centre of the liver on B-mode and colour Doppler images, respectively. (c) Colour within the vessel confirms that the direction of flow is away from the transducer; ie, from the periphery towards the centre of the liver
Liver size
Assessment of liver size is subjective, although there is less variation in cats than in dogs due to their more uniform body size. 2 A liver that extends well beyond the costal arch or ventral to the right kidney is suggestive of enlargement. 2 Liver lobes should have smooth margins that taper to a sharp point; rounding is indicative of enlargement (Figure 8). 2 Microhepatica is uncommon in cats but may be inferred when there is a reduction in the volume of liver parenchyma between the diaphragm and the stomach, and also when the gall bladder appears abnormally large relative to the volume of liver tissue, although this is dependent on the absolute size of the gall bladder. 2

Rounding of the liver (arrows) in a cat with hepatomegaly
Abnormalities of the liver
Hepatic parenchymal lesions can be grouped into three categories – diffuse, focal and multifocal – and all have the potential to cause changes in liver size, shape and echogenicity.

Increased hepatic echogenicity
An abnormal increase in hepatic echogenicity may be suspected if the liver is at least moderately hyperechoic relative to the spleen (Figure 9) and/or falciform fat, and portal vein walls are poorly visible. A moderate to marked increase in echogenicity relative to the renal cortex may also raise suspicion for an abnormally echogenic liver. Differentials for a diffusely hyperechoic liver with preservation of normal hepatic architecture include hepatic lipidosis, chronic hepatitis/cholangio-hepatitis, fibrosis and lymphoma.2,8-12

This liver is markedly echogenic relative to the spleen. Note also the presence of sludge within the gall bladder (arrows)
Hepatic lipidosis is the most commonly diagnosed disease affecting the feline liver.12,13 Cats at greatest risk of developing the condition are those with a high body condition score that become anorexic. 14 Typical features on ultrasound include an enlarged, diffusely hyper-echoic liver with an echogenicity greater than that of falciform fat, poor visibility of intrahepatic portal vein walls and increased attenuation of sound by the liver (Figure 10). 8 Hyper-echogenicity of the liver relative to the falciform fat has been reported to be the best criterion for diagnosis, with a sensitivity of 91% for the detection of severe hepatic lipidosis in cats. 8

Typical ultrasonographic appearance of hepatic lipidosis in a cat. The liver is markedly enlarged and almost fills the entire image. Intrahepatic portal vein walls are difficult to identify due to a diffuse increase in echogenicity of the liver parenchyma. Courtesy of Jeremy Mortier, University of Liverpool, UK
Interestingly, steroid hepatopathy and cirrhosis, which are relatively common conditions associated with a diffuse increase in hepatic echogenicity in the dog, are rarely reported in the cat.15,16 A diffuse increase in hepatic echogenicity has also been reported in dogs with mast cell infiltration of the liver. 17 To the author’s knowledge, this specific finding has not been reported in cats. However, it is known that cats with hepatic mast cell neoplasia can have an ultrasonographically normal liver and it follows that an apparently normal liver on ultrasound does not exclude the possibility of mast cell infiltration in the cat. 18
Decreased hepatic echogenicity
A diffuse reduction in echogenicity of the liver may be suspected if portal vein walls appear more prominent than usual and can be seen extending to the very periphery of the liver, and also if the hepatic parenchyma is moderately less echogenic than the renal cortex (Figure 11). 2 A diffusely hypoechoic liver is a relatively uncommon finding and differentials include acute suppurative hepatitis, passive congestion, lymphoma, mast cell neoplasia and amyloidosis, all of which can also result in an enlarged liver.10,11,19-21

A hypoechoic liver in a 6-year-old female spayed domestic shorthair cat. The walls of the portal veins (arrowheads) appear abnormally prominent
Passive hepatic congestion is usually associated with hepatomegaly, dilation of the caudal vena cava and hepatic veins, and ascites. 11 It is, however, rarely observed since the most common causes of passive congestion in dogs, such as right-sided cardiac failure and large pericardial effusions, are uncommon in the cat.
Heterogeneous hepatic echogenicity
A heterogeneous liver typically has a hyper-echoic parenchyma, dispersed throughout which are multiple poorly defined hypoechoic nodules, although hyperechoic nodules are also possible. 2 Diagnostic differentials for a liver with a diffusely mixed echogenicity include hepatic lipidosis in association with benign nodular hyperplasia, extramedullary haematopoiesis, cholangitis/cholangiohepatitis, toxic hepatopathy, hepatic necrosis and cirrhosis, lymphoma, mast cell neoplasia, metastatic disease and amyloidosis.1,20-22
Amyloidosis is a rare condition to which young Abyssinian and Siamese cats, among other oriental breeds, have a predisposition. Cases have also been reported in domestic shorthair cats and in a Devon Rex.16,23 The main target organ in Abyssinian cats is the kidney; in Siamese, the liver is more commonly affected. 24 Large amounts of amyloid protein are deposited in the liver, resulting in hepatomegaly and disruption of normal hepatic function. The ultrasonographic appearance is that of a heterogeneous and diffusely enlarged liver with irregular borders that may contain both highly echogenic (‘sparkling’) areas and hypoechoic foci (Figure 12). 23 In severe cases, the liver can become highly friable, resulting in spontaneous liver rupture and potentially fatal haemoabdomen. 23

Ultrasound images of confirmed hepatic amyloidosis in three cats. (a,b) Liver of a 5-year-old female Chantilly-Tiffany cat that was presented with anorexia, lethargy, anaemia and increased alanine aminotransferase. The liver is markedly enlarged and heterogeneous throughout. Free peritoneal fluid is visible in the bottom left corner of image (b) (arrow) and was confirmed to be blood following abdominocentesis. (c) Caudal portion of the liver in a 9-year-old female neutered Oriental Shorthair cat that was presented with inappetence, lethargy and severe anaemia. The lobe is markedly hypoechoic and rounded, indicating enlargement. At the time of scanning, the liver could be seen extending into the mid-abdomen. Although not shown here, swirling echogenic peritoneal fluid was also visible, which was confirmed to be haemorrhage following abdominocentesis. (d,e) Liver of a 3-year-old female neutered Oriental Shorthair cat that was referred for investigation of anaemia and suspected haemoabdomen. The liver is enlarged and markedly heterogeneous due to the presence of both hyper- and hypoechoic areas of tissue. A small volume of peritoneal blood (asterisk) is also visible between liver lobes in (d). Images (a) and (b) courtesy of Luis Mesquita, Willows Veterinary Centre and Referral, UK
The cholangitis/cholangiohepatitis complex represents the second-most common hepatic disease in cats and the most common feline inflammatory liver disease.25,26 The condition can be associated with a liver of normal, increased, decreased or heterogeneous echogenicity (Figure 13).1,27 Increased echogenicity may be the result of fibrosis during the chronic stage of the disease and/or concurrent lipidosis. The liver may have a uniform or heterogeneous nodular echotexture 9 and, although often normal in size, may be enlarged in some cases. 27 Abnormalities of the biliary tree are frequently observed with this disease and will be discussed in detail in a forthcoming review in this series.

(a) Ultrasound image of a heterogeneous liver in a 14-year-old female neutered domestic shorthair cat with neutrophilic cholangiohepatitis. (b) Ultrasound image of the liver of a 7-year-old female neutered domestic shorthair cat with confirmed cholangiohepatitis. Again, note the marked heterogeneity of the liver parenchyma

Nodular hyperplasia
Nodular hyperplasia is a benign proliferative disorder of the liver that is frequently identified in older dogs and is of no clinical significance. 16 In contrast, there is little information available relating to cats, presumably due to its low incidence in this species. 16 The presence of multiple hepatic nodules in a cat on histopathology, resembling focal nodular hyperplasia in man, has been reported. 28 However, to the author’s knowledge, the ultrasonographic appearance of nodular hyperplasia in the cat has not been described.
Neoplasia
Primary hepatobiliary tumours can arise from hepatocytes (hepatocellular adenoma or carcinoma), bile duct epithelium (biliary adenoma or carcinoma), stromal cells (sarcomas) and neuroendocrine cells. 29 In contrast to dogs, primary hepatobiliary tumours are more common than metastatic disease in cats. 30
Biliary cystadenomas are the most common hepatobiliary tumour recognised in the cat.31,32 They are benign focal or multifocal cystic tumours that usually affect cats 10 years of age and older.33-35 Alternative names include bile duct adenoma, cholangiocellular adenoma, cystic cholangioma and hepatobiliary cystadenoma. 25
The ultrasonographic appearance of biliary cystadenomas is typically that of a multilocular mass containing numerous thin-walled cysts that can vary in diameter from 1 mm to 8 cm or a hyperechoic or mixed echogenicity mass with a cystic element (Figure 14). 33 The hyperechoic component of these masses is likely to be due to a combination of fibrous stroma and the presence of multiple acoustic interfaces associated with a large number of very small cysts, resulting in increased sound reflection. 33 Cystic contents are usually an-echoic, although internal echoes may be recognised, 33 and masses are typically associated with distal acoustic enhancement due to the presence of fluid trapped within the cysts. 33

(a–c) Ultrasound images showing the variable appearance of cystadenomas (arrows) in three cats. Note the acoustic enhancement distal to the mass in (a) due to the presence of fluid within the cysts
These tumours can grow to large proportions and cystadenomas measuring up to 12.5 cm have been described in the cat. 33 While they are generally considered to be incidental findings, they can occasionally become so large that they compress nearby structures, such as the stomach, resulting in clinical signs. It should be noted that, although the ultrasonographic appearance of a biliary cystadenoma is relatively characteristic, a mast cell tumour presenting as a large cystic mass on ultrasound has been reported in a cat. 18
Biliary cystadenocarcinomas are the malignant form of biliary cystadenomas and the second-most common hepatobiliary tumour in the cat. 32 In humans they have been reported to arise from malignant transformation of biliary cystadenomas and can only be differentiated from the latter with histopathology due to a significant overlap in the appearance of the two tumours on ultrasound.36,37
The ultrasonographic appearance of other forms of hepatic neoplasia in cats is highly variable, ranging from focal and multifocal nodules or masses (Figure 15), to diffuse changes in echogenicity. Occasional reports have described the ultrasound findings in cats with particular tumour types such as mast cell tumours (see earlier) and lymphoma. Hepatomegaly, diffuse hyper- or hypoechogenicity and hepatic nodules have all been found in association with feline hepatic lymphoma (Figure 16). 21 Furthermore, round cell neoplasia may produce no abnormalities on ultrasound and, therefore, the absence of changes on ultrasound does not rule out the possibility of neoplasia (Figure 16). 19
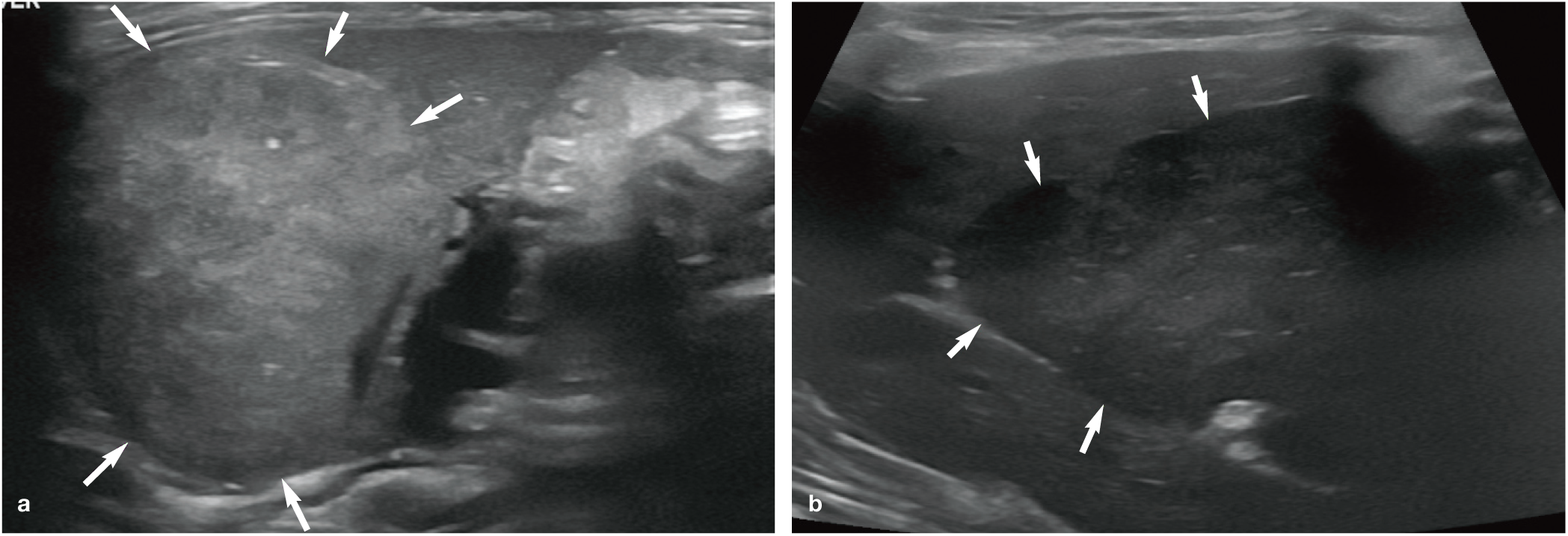
(a,b) Ultrasound images showing the highly variable appearance of hepatocellular carcinoma (arrows) in two cats

(a) A highly heterogeneous liver containing multiple hypoechoic masses that are causing complete effacement of normal hepatic architecture in a 4-year-old male neutered Siamese cat with lymphoma. (b) Hepatomegaly and an otherwise unremarkable liver in a 10-year-old male neutered domestic shorthair cat with lymphoma. Hepatic involvement was confirmed by cytology of fine-needle aspirates in both cases
Abscessation
Hepatic abscesses are rare in cats and frequently associated with vague clinical signs and a high mortality rate.38,39 Extrahepatic sites of infection may be present concurrently and the formation of abscesses secondarily to necrosis of hepatic neoplasia has been reported.38,40 Ultrasonographic findings are similar to those observed in the dog. Abscesses may be solitary, multifocal or microscopic. 38 The typical appearance is that of an irregular, thick-walled, hypo- or hyperechoic cavitary mass, possibly with evidence of sedimentation of luminal contents and distal acoustic enhancement (Figure 17).38,39 The presence of intralesional gas may be suspected if hyperechoic foci associated with reverberation artefact are present. Surrounding fat and/or hepatic parenchyma can be echogenic due to inflammation, and a localised peritoneal effusion and regional lymphadenopathy may also be present. 38

Typical ultrasonographic appearance of an abscess within the liver. Note the thick irregular walls and echogenic material within the lumen
Ultrasound-guided aspiration can be performed to confirm the diagnosis and to obtain a sample for culture and sensitivity testing. Successful percutaneous drainage of abscesses under ultrasound guidance in five dogs and one cat has been reported with no complications. 39 The author likewise has not experienced complications associated with the procedure.
However, owners should be made aware of the potential risks, which include the possibility of purulent material leaking from the abscess after the needle is withdrawn and subsequent peritonitis. The risk of leakage occurring is substantially reduced by ensuring that the abscess is completely drained. Additionally, as with any interventional procedure, there are the risks of inadvertent puncture of a blood vessel resulting in haemorrhage or unintentional puncture of a structure other than the target. In humans, accidental puncture of the intestine, stomach, liver and spleen have all been reported. 41 Such complications are usually avoidable with careful attention to the path of the needle and by ensuring the tip of the needle remains visible at all times.
Granulomas
Hepatic granulomas and pyogranulomas may appear ultrasonographically as one or more well-defined hyperechoic nodules of variable size within the hepatic parenchyma.20,42 While relatively uncommon, they may be present in certain conditions such as feline infectious peritonitis (FIP), feline eosinophilic fibroplasia and mycobacterial infection.43,44
Haematomas
To the author’s knowledge, the ultrasonographic appearance of hepatic haematomas has not been described in the cat. The expected appearance based on information published in dogs is that of a focal, irregularly marginated area of mixed echogenicity within the liver.20,45 The appearance of a haematoma will vary over time as it ages, becoming gradually more hypoechoic and more clearly defined. 2
Lobar torsion
Liver lobe torsion causes lobar congestion and necrosis. The condition is rare in the cat and, to date, only three cases have been described.46-48 In two cats, the torsed liver lobe presented on ultrasound as a hypoechoic mass adjacent to and continuous with the liver.46,47 Cavitation was present within one of the masses and colour flow Doppler was used to confirm a lack of blood flow within the affected lobe. In both cases, the left lateral liver lobe was involved and the mass effect was considered to be secondary to the torsion and subsequent congestion. A small volume of almost anechoic peritoneal effusion was also identified in one of the cats. The third case of torsion involved the right medial liver lobe of a cat, which contained a ruptured hepatocellular carcinoma, but no ultrasound findings were documented. 48
Sampling the liver
Even when taking into account multiple ultrasonographic criteria such as size, shape and echogenicity, the information gathered is often insufficient to discriminate accurately between different diseases of the liver. 22 Therefore, sampling (fine-needle aspiration [FNA] or core needle biopsy) is usually necessary to confirm the presence and nature of suspected hepatic disease.


(a) A 16 G semi-automatic core biopsy needle suitable for ultrasound-guided biopsy of the liver. (b) Tip of the needle showing the outer cannula and inner shaft. On firing the device, the outer cannula slides rapidly over the shaft, trapping a specimen of tissue

Ultrasound image acquired during Tru-cut biopsy of the liver. By ensuring the needle remains within the plane of the ultrasound beam, it is easily recognised within the image and non-target structures are avoided
The main disadvantage of FNA is the small sample size obtained and the limited diagnostic utility of the technique with regards to inflammatory liver disease, such that it is not considered appropriate for diagnosing lymphocytic cholangitis.49,51,52 In a report on the accuracy of FNA of the liver in 41 cats, there was agreement between the histopathological results and cytological diagnosis in only 21 (51.2%) cats. 51 A different study highlighted the issue of misleading results from FNA of the liver in four cats; 53 cytology of FNA samples was indicative of hepatic lipidosis in each case whereas histology of tissue samples obtained by Tru-cut or wedge biopsy was consistent with inflammatory or neoplastic disease. 53 FIP may be an exception to this, with one study reporting that FNA of the liver had a higher diagnostic sensitivity (82%) for FIP than core biopsy (64%). 54
The main advantage of the core needle technique over FNA is that a substantially larger tissue biopsy can be procured and hence there is a greater likelihood of obtaining a representative sample for diagnosis. Nevertheless, sampling errors can arise if lesions are distributed unevenly throughout the liver and are missed during biopsy. 55 In humans, it is recommended that biopsy specimens are >15 mm to achieve an acceptable degree of accuracy in the histological diagnosis. 56 In some circumstances, such as when differentiation between acute and chronic hepatitis is necessary, biopsy specimens >25 mm in length may be required and even this may not always be sufficient for an accurate diagnosis. 56 In one study, median biopsy specimen length from the liver following needle core biopsy was >15 mm in only 2/26 cats. 55 This is perhaps not unexpected given the liver of a cat is much smaller than that of an adult human. However, it does mean that the low number of portal triads present in each specimen may be insufficient for accurate morphological characterisation of diffuse and multifocal hepatic disease. 55 The authors of this study concluded that needle biopsy results should be interpreted with caution since they found that they were not as accurate as wedge biopsy specimens for determining a definitive diagnosis. 55 Histopathology should still, therefore, be considered the gold standard for the diagnosis of most hepatobiliary diseases in the cat. 55
Owing to the use of a much larger diameter needle, core biopsies carry a higher risk of complications such as haemorrhage, bile peritonitis, abscessation, pneumothorax and death. A small volume of haemorrhage is not uncommon following the procedure and can be monitored with ultrasound. It is advisable to check clotting function and platelet count prior to biopsy. In one large study, major complications were reported in eight cats with coagulation deficiencies following biopsy of the liver with an 18 G Tru-cut-like biopsy needle. 57 A major complication was defined as either the requirement for intervention in the form of a transfusion of blood products or resuscitative fluids to address haemodynamic instability, or death as a result of haemorrhage. 57 The authors of that study found that cats with a prolonged activated partial thromboplastin time (aPTT), or marked thrombocytopenia, were more likely to have complications than cats with normal values. Furthermore, core needle biopsy of the liver is contraindicated in cats with microhepatica, a large peritoneal effusion, cavitary hepatic lesions such as abscesses or cysts, or lesions that are too close to large bile ducts or blood vessels for the procedure to be performed safely. 58

Readers should also be aware that the use of an automatic Tru-cut biopsy gun has been linked to fatal shock reactions in five cats. 59 Death was attributed to a pressure wave created by the strong spring mechanism of the device that, in turn, caused intense vagotonia and shock. 59 Such automated devices are thus inappropriate for use in cats. No similar major adverse effects have been reported in association with semi-automatic devices. 59
Key Points
Sedation for abdominal ultrasound is preferable in most cases (where safe to perform) and will improve the quality of the ultrasound examination.
Normal liver parenchyma has a relatively coarse echotexture and is similar in echogenicity to the spleen.
Focal and multifocal hepatic lesions are usually more readily identifiable with ultrasound than diffuse hepatic disease.
Biliary cystadenomas are the most common hepatobiliary tumour in the cat and typically present as a cystic mass within the liver parenchyma.
Ultrasonographic abnormalities in cats with cholangiohepatitis include a liver that has increased, decreased or heterogeneous echogenicity.
FNA is often diagnostic in cases of hepatic lipidosis and lymphoma but less useful in the presence of inflammatory hepatic disease. Core needle biopsy provides a larger sample of tissue, although the procedure may need to be delayed in cats with a prolonged aPTT and/or thrombocytopenia due to an increased risk of clinically significant haemorrhage.
Footnotes
Conflict of interest
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.