
Abstract
Objectives
The aim of this study was to evaluate a feline coronavirus (FCoV) reverse transcriptase quantitative PCR (RT-qPCR) on fine-needle aspirates (FNAs) from mesenteric lymph nodes (MLNs) collected in sterile saline for the purpose of diagnosing non-effusive feline infectious peritonitis (FIP) in cats.
Methods
First, the ability of the assay to detect viral RNA in MLN FNA preparations compared with MLN biopsy preparations was assessed in matched samples from eight cats. Second, a panel of MLN FNA samples was collected from a series of cats representing non-effusive FIP cases (n = 20), FCoV-seropositive individuals (n = 8) and FCoV-seronegative individuals (n = 18). Disease status of the animals was determined using a combination of gross pathology, histopathology and/or ‘FIP profile’, consisting of serology, clinical pathology and clinical signs.
Results
Viral RNA was detected in 18/20 non-effusive FIP cases; it was not detected in two cases that presented with neurological FIP. Samples from 18 seronegative non-FIP control cats and 7/8 samples from seropositive non-FIP control cats contained no detectable viral RNA. Thus, as a method for diagnosing non-effusive FIP, MLN FNA RT-qPCR had an overall sensitivity of 90.0% and specificity of 96.1%.
Conclusions and relevance
In cases with a high index of suspicion of disease, RT-qPCR targeting FCoV in MLN FNA can provide important information to support the ante-mortem diagnosis of non-effusive FIP. Importantly, viral RNA can be reliably detected in MLN FNA samples in saline submitted via the national mail service. When applied in combination with biochemistry, haematology and serological tests in cases with a high index of suspicion of disease, the results of this assay may be used to support a diagnosis of non-effusive FIP.
Keywords
Introduction
Feline coronavirus (FCoV) is an alpha-coronavirus that is ubiquitous among populations of Felidae. FCoV and other viruses within this family are associated with enteric disease, such as ferret coronavirus, canine coronavirus and transmissible gastroenteritis virus of pigs. 1 In addition to its primarily enteric pathogenesis, FCoV is associated with a progressive disease named feline infectious peritonitis (FIP). 2 In the majority of cases, FCoV infection is not accompanied by overt clinical signs. A proportion of cats exposed to the virus exhibit signs of mild enteric disease, usually manifesting as transient diarrhoea, sometimes with vomiting. 3 In around 5% of cases 4 the virus elicits an aberrant immune response in the host, resulting in an almost invariably lethal pyogranulomatous perivasculitis, a consequence of extravasation of FCoV-infected monocytes. 5 FIP is considered to consist of a spectrum of presentations, with an effusive form at one end and a non-effusive form at the other. 6
In recent years, great strides have been made in the diagnosis of effusive FIP. Collection of effusion samples from the body cavities is a minimally invasive veterinary intervention. Recent studies have shown that the detection of FCoV by RT-qPCR, using template RNA from the effusion, is highly supportive of a diagnosis of effusive FIP,7–10 although two recent studies did find low amounts of FCoV RNA in effusions of 1/29 and 1/47 cats in their control groups of cats without FIP.7,11,12 However, as a minimally invasive sampling technique has not been described for non-effusive FIP, confirmation is often achieved only at the time of post-mortem examination. A major difficulty in the diagnosis of FIP is the vast and variable range of clinical signs associated with the disease. Although haematological, biochemical and serological parameters may be measured to provide an index of suspicion of FIP, these cannot be used to confirm a diagnosis.
Cats are frequently subjected to invasive biopsy procedures, which often do not result in a conclusive diagnosis. Kipar et al 13 described one manifestation of non-effusive FIP primarily presenting as enlargement of the mesenteric lymph nodes (MLNs), similar to a manifestation of coronavirus-induced pyogranulomatosis reported in the ferret, 14 and frequently mistaken for tumours in both species.13,15 In one study, pyogranulomatous lesions were found in the MLNs in 8/24 (33%) cats with FIP, 16 while in another, mesenteric lymphadenopathy was noted by ultrasound in 9/16 cats with FIP. 17 It should be appreciated that other conditions, such as toxoplasmosis, can also present with enlarged MLNs. 18
Histopathological identification of FIP lesions in biopsies is currently the only method to confirm a diagnosis of non-effusive FIP. However, histopathology of the lymph node in FIP can reveal non-specific pyogranulomatous inflammation, which has many possible causes. In such cases, immunohistochemistry (IHC) to detect FCoV-specific proteins may be performed. The reliability of IHC depends on the specificity of the assay. A poorly designed assay, such as one with no negative control antibody run for every section of tissue on which the anti-FCoV antibody is run, will fail to identify non-specific adherence of antibodies to some feline tissues, causing false-positive results (unpublished observation). IHC can also lack sensitivity, as it depends on the surgeon submitting an area of the organ in which virus-infected cells were present.
In non-effusive FIP there may be few lesions and in order to obtain an accurate biopsy an exploratory laparotomy is usually required. Laparotomy for the collection of biopsy material is an invasive, potentially stressful and risk-associated intervention, which may adversely affect an already sick cat in which FIP is suspected. It has been shown that cats with FIP often have a history of stress,19,20 although it is unknown whether experiencing further stress after FIP has developed affects the outcome. Moreover, immunosuppressive doses of corticosteroids, routinely used for FIP treatment, are contraindicated in cats that have undergone recent surgery, as they hamper the healing process. In contrast, ultrasound-guided collection of fine-needle aspirate (FNA) material is a far less invasive procedure.
The detection of viral RNA in faeces or blood or the detection of anti-FCoV antibodies in the blood is not diagnostic of FIP. Combinations of all three findings may be present in FCoV-infected cats that are healthy, or that are sick as a result of non-FIP diseases. 6 As a considerable proportion of the feline population may be positive for FCoV antibodies, up to 26% in the UK, 21 a major challenge for the clinician is the diagnosis of FIP in the FCoV-seropositive cat that the presence of antibodies may either be incidental or may be associated with FIP. The predictive value of a negative FCoV antibody test for ruling out FIP has been calculated as 97%, 22 and therefore a seronegative result usually excludes FIP provided that a sufficiently low initial serum dilution is used, such as 1:20. 23
Previous studies have shown results consistent with a diagnosis of non-effusive FIP can be observed through microscopic examination of smear preparations from FNAs or Tru-cut biopsies of the liver and/or kidney. 24 However, in many cases such samples provide inadequate material for analysis owing to the destruction of cellular morphology, thus reducing test sensitivity. 24 We hypothesised that the problem of cellular damage could be avoided by using reverse transcriptase quantitative PCR (RT-qPCR) to detect FCoV in FNA samples derived from MLN. Such a technique has the potential to be a minimally invasive diagnostic test for non-effusive FIP.
The aim of the present study was to therefore evaluate the diagnostic potential of MLN FNAs combined with FCoV RT-qPCR. As an initial step, the sensitivity of this method was compared with RT-qPCR of MLN biopsies (MLNBs). In a prospective study, the specificity of MLN FNA FCoV RT-qPCR was then analysed using samples from groups of cats that were: (1) FCoV seronegative; (2) seropositive but without signs indicative of FIP (or had confirmation of other diseases/causes of death); and (3) FIP cases. MLN FNA samples submitted to the Veterinary Diagnostic Service (VDS) at the University of Glasgow were also evaluated to determine if non-preserved (ie, saline) samples submitted from field clinics would be suitable, thereby assessing if transit to the laboratory adversely affected test sensitivity. A full assessment of the sensitivity, specificity and diagnostic accuracy of the method was performed.
Materials and methods
Ethical approval
The study was approved by the Ethics and Welfare Committee at the University of Glasgow, School of Veterinary Medicine.
Sources of clinical samples
Samples from eight FIP cases were used for an initial study (group T). The main study then included a group of twenty cats with non-effusive FIP (group D), a control group of eight seropositive cats without FIP (group P) and a second control group of 18 seronegative cats (group N) also without FIP; details of the source of samples for these three groups are provided in Table 1. A proportion of these samples (n = 25) was collected from cats in the post-mortem room at the School of Veterinary Medicine, University of Glasgow, that had been submitted for post-mortem examination from veterinary practices throughout the UK. The remainder of samples came directly from referring veterinary surgeons across the UK, including MLN FNAs collected in vivo and submitted in a small amount of sterile saline in a plain tube (n = 13), MLNB material collected in vivo (n = 1) and MLNBs collected post mortem (n = 7) by the referring veterinary surgeon and submitted to the laboratory by first class post. Samples received in the laboratory were stored at 4ºC until processed. The time from sample collection to processing ranged from 24 h to 7 days, with most samples being processed between 48 h and 72 h post-collection.
Mesenteric lymph node (MLN) fine-needle aspirate (FNA) sample source and classification

Non-specific signs including, but not limited to, pyrexia, lethargy, inappetence and icterus
✓ indicates that clinical sign is present/test results support a diagnosis of feline infectious peritonitis (FIP)
✗ indicates that test results do not support a diagnosis of FIP
FCoV = feline coronavirus; MLNB = mesenteric lymph node biopsy; IHC = immunohistochemistry; ABCD = European Advisory Board of Cat Diseases; UniPM = MLN FNA collected by University of Glasgow pathologist; Field = MLNB or MLN FNA collected by referring veterinary surgeon; NR = not recorded; NAD = no abnormality detected; RTA = road traffic accident; FIV = feline immunodeficiency virus
Preparation of samples
Collection of MLNB material
MLNBs were collected post mortem by the University of Glasgow post-mortem room pathologist (supplementary material 1) or in vivo by the submitting veterinary surgeon during exploratory laparotomy or post-mortem examination. Samples were placed in sufficient sterile saline to cover the biopsy material for transit to the laboratory.
MLN FNAs
MLN FNA samples were collected either in vivo at participating veterinary practices or in situ at the University of Glasgow during post-mortem examination or extra corpus in the laboratory from excised lymph nodes. In vivo MLN FNA samples collected by ultrasound guidance or at exploratory laparotomy were expelled into 0.2–0.5 ml sterile saline in plain tubes and then mailed to the laboratory by first-class post, without refrigeration. Post-mortem samples were collected in situ using a 21 G needle and a 2 ml syringe; MLNB was also collected to be stored as a back-up. Extra corpus FNAs were performed on either MLNBs or whole MLN collected ante mortem (n = 1) or during post-mortem examination (n = 7). Paired FNA samples were prepared using a 21 G needle and a 2 ml syringe; one was expelled into 0.5 ml sterile saline and the other expelled into 0.5 ml RNAlater (Ambion) to inactivate RNAses and maintain the integrity of RNA therein during long-term storage. FNAs collected into RNAlater and any remaining MLNBs (approximately 0.5 cm cubed/0.5 ml RNAlater) were stored in our biobank.
FIP diagnosis
Diagnosis of FIP was confirmed by histopathology where suitable sample material was available. Sufficient blood and tissue samples for virology, clinical pathology and histopathology had been collected in these cases to acquire a diagnosis. Tissue samples for histopathology were collected in 10% formal saline, including MLN and one or more of the following: kidney, liver, lung, spleen, omentum and any others deemed relevant for diagnosis.
Where histopathology was unavailable or inconclusive, FIP diagnosis was based on the laboratory testing steps of the European Advisory Board of Cat Diseases (ABCD) FIP diagnosis algorithm, 6 as performed under the VDS laboratory ‘non-effusive FIP profile’. This commercial test profile comprises the following suite of blood tests: FCoV antibody titre, alpha-1 acid glycoprotein measurement,25,26 albumin:globulin ratio, haematocrit and lymphocyte count.
In group D (non-effusive cases, n = 20), 10 cases were confirmed by histopathology/IHC, one by gross pathology and the remainder were highly suspected of FIP on the basis of FIP profile. In the control groups, FIP was ruled out by a combination of histopathology and gross post-mortem examination in the seropositive group (P) in 7/8 cats and in the seronegative group (N) in 17/18 cats. A negative FIP profile was used to rule out FIP in a single case in each of the control groups (Table 1).
RNA extraction
RNA extraction from both MLNB and MLN FNA samples was performed using the RNAqueous 4-PCR extraction kit (Ambion). All materials form part of the RNAqueous 4-PCR kit unless otherwise stated. All equipment was wiped with RNAse ZAP (Ambion). Tubes and pipette tips (Sarstedt) were RNAse and DNAse free. MLNB samples were cut into portions not larger than 0.075 g, added to a gentleMACS M tube (Miltenyi Biotech) with 700 µl lysis buffer and homogenised by a gentleMACS Dissociator (Miltenyi). The M tube was centrifuged at 100 g at 4ºC for 10 mins, to ensure all material was lysed, and this step was repeated if required. RNAse-free and DNAse-free phosphate buffered saline solution (Sigma) at 4ºC was added to the MLN FNA sample in saline and centrifuged at 100 g at 4ºC. The resulting supernatant was discarded and the pellet resuspended in 250 µl lysis buffer. Lysed MLNB and MLN FNA samples were kept on ice at all times. The extractions were performed as per the manufacturer’s instructions, followed by DNAse treatments to remove contaminating DNA. The RNA extract was transferred to a 1.5 ml tube (Sarstedt) and stored at −80ºC. The RNA extract underwent quantification and quality analysis using a Nanodrop 2000 (Thermo Fisher Scientific).
RT-qPCR
The quantitative FCoV RT-qPCR assay was modified from the method of Gut et al, 27 based on the conserved 3′ untranslated region of the FCoV genome. This assay is capable of detecting both type I and type II FCoV.
RT-qPCR was performed using the Superscript III Platinum One Step RT-PCR System (Invitrogen). Unless otherwise stated, reagents were sourced from Invitrogen. Primer and probe sequences are detailed in Table 2. Each reaction consisted of nuclease-free PCR-grade water (Hyclone; GE Healthcare Life Sciences/Qiagen), reaction mix containing dNTPs, 500 nM FCoV forward primer (Eurofins MWG Operon), 1 µM FCoV reverse primer (Eurofins MWG Operon), 200 nM FCoV probe (Eurofins MWG Operon), 25 mM ROX passive reference dye and Superscript Platinum III. In total, 17 µl master mix was loaded into each well of a 96-well plate (Applied Biosystems) and 3 µl RNA extract or assay control was added as required. The plate was then centrifuged briefly to eliminate air bubbles before RT-qPCR was performed using the 7500 RT-PCR System (Applied Biosystems). A reverse transcriptase step was performed at 48ºC for 30 mins, followed by a denaturing step at 95ºC for 2 mins. Thereafter, 40 cycles consisting of 95ºC for 15 s and 60ºC for 1 min were performed.
Samples were run in duplicate; no samples were found to produce conflicting results. Samples in which an amplicon was not detected by cycle 40 were deemed to be negative. The Ct value for each reaction was recorded, with a lower Ct value resulting from greater template RNA in the reaction mixture. Glyceraldehyde phosphate dehydrogenase (GADPH) RT-qPCR was also performed on each sample; this was particularly important for FCoV RNA-negative samples to demonstrate that there was sufficient RNA in each reaction. The protocol was the same as that of the FCoV RT-qPCR described above, with the primers and probe substituted for GAPDH specific primers and probe (see Table 2).
Primers and probe sequences used in the RT-PCR assay
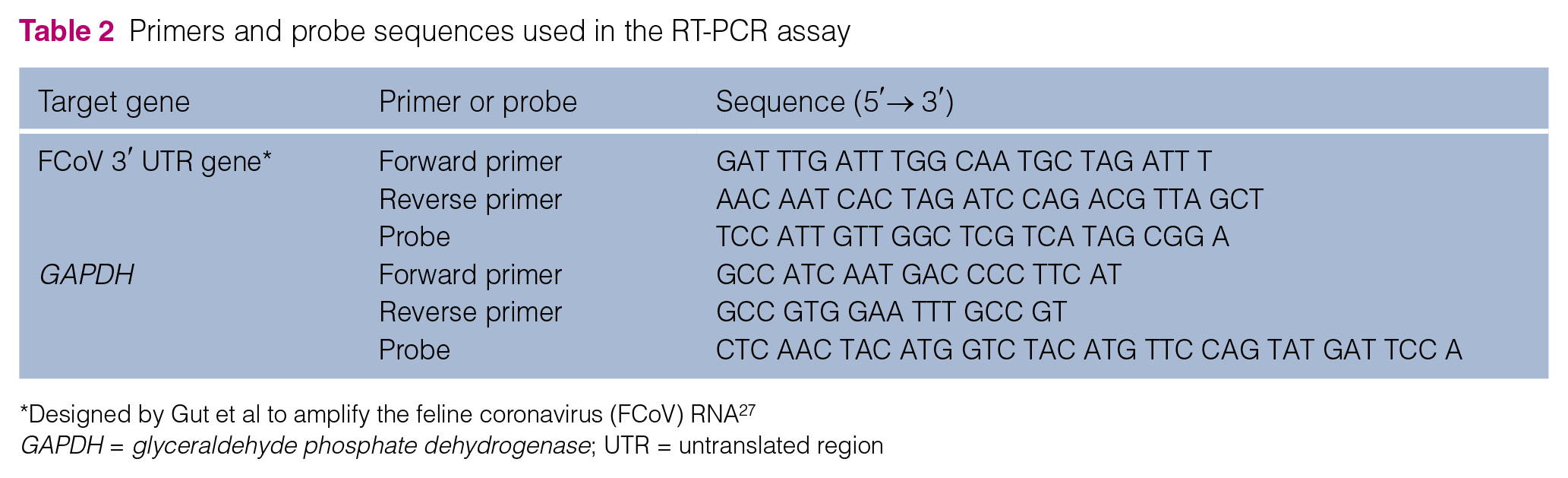
Designed by Gut et al to amplify the feline coronavirus (FCoV) RNA 27
GAPDH = glyceraldehyde phosphate dehydrogenase; UTR = untranslated region
FCoV indirect immunofluorescent antibody test
The FCoV indirect immunofluorescent antibody test was performed as previously described. 28
Statistical analysis
Fisher’s exact test (two-tailed) and the Pearson correlation coefficient (r) were calculated using the core ‘stats’ package in R. 29 Scatter plots were generated using ‘ggplot2’ in R.29,30 Inter-rater agreement was determined using a 2 × 2 contingency table and the kappa statistic (κ) with 95% confidence intervals (CIs) calculated using the ‘fmsb’ package in R.29,31
Results
Viability of MLN FNAs for FCoV qRT-PCR assays
A panel of matched MLN FNAs and MLNBs was assembled from a total of eight cats with a confirmed diagnosis of FIP (T01–T08). The quantity of RNA recovered from FNA preparations varied between 3 and 199 ng/µl, while that recovered from the MLNB preparations varied between 178 and 1855 ng/µl (supplementary material 1). On average, a 35-fold lower concentration of RNA was recovered by FNA than by MLNB preparation, although this varied widely.
RT-qPCR was performed to evaluate the presence of host (GAPDH) and viral RNA in both the FNA and MLNB preparations. FCoV RNA was detected in each FNA and MLNB preparation, as was the presence of host-encoded RNA. Overall, slightly higher Ct values were noted for both host and viral genes for the MLN FNA reactions, indicating a lower level of template nucleic acid. MLN FNA FCoV Ct values ranged from 19.4–36.1, whereas for MLNB FCoV the range was 18.0–28.1, with lower MLNB FCoV Ct values recorded in each of the paired samples. The relationship of FCoV Ct values between sample types is illustrated in Figure 1. For the MLN FNA preparations, a strong negative correlation existed between the GAPDH Ct value and the concentration of total RNA (r = −0.87, P <0.01), as expected. However, only a moderate correlation, which was not statistically significant, existed between the FCoV Ct value and total RNA concentration (r = −0.61, P = 0.11), and therefore it could not be concluded that the level of template viral RNA (ie, viral load) was fully dependent on the concentration of total RNA, the majority of which is host-encoded.
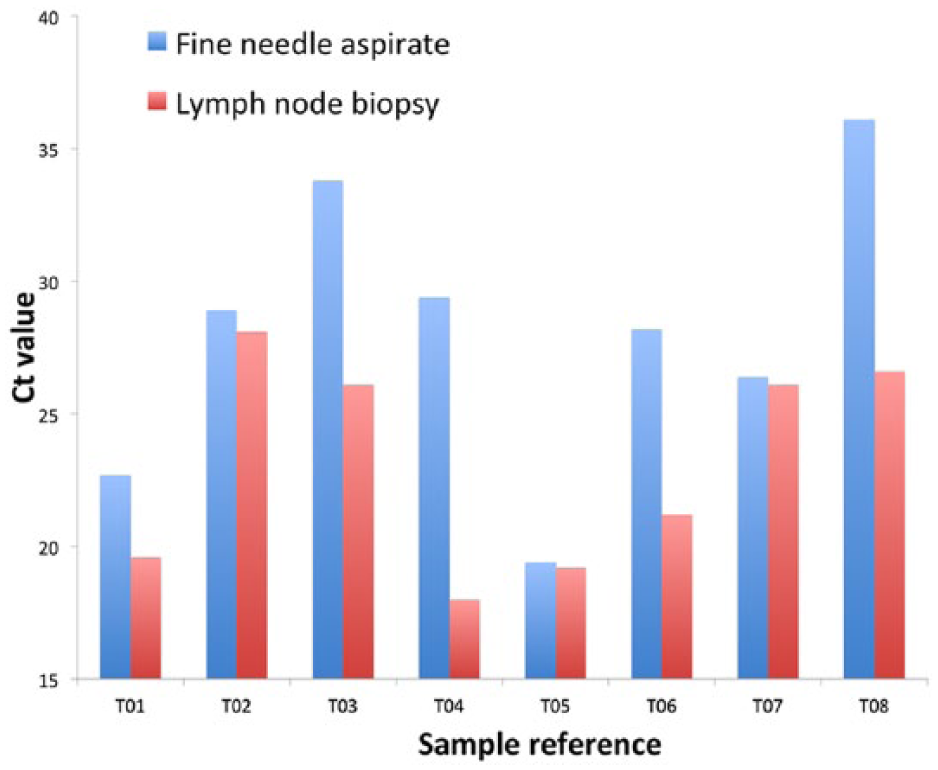
Bar chart illustrating the relationship between feline coronavirus RT-qPCR Ct values from matched mesenteric lymph node (MLN) biopsy (MLNB) and fine-needle aspirate (FNA) samples. The Ct values from MLNBs were generally lower than those from MLN FNAs, indicating higher virus loads in the MLNB pieces than in FNAs. However, three samples produced MLNB and MLN FNA Ct values that were almost identical
Viability of RNA in MLN FNAs collected in the field
As GAPDH RT-qPCR Ct values were shown to strongly correlate with RNA concentration and are dependent on viable host RNA, these values were used as an index for RNA sample quality, in terms of both quantity and intactness. GAPDH Ct values of 32 MLN FNA samples prepared/collected at the university were compared with 12 samples submitted by mail from external veterinary practices, in order to check for potential RNA deterioration while in transit (supplementary material 2). The median in-house Ct value was 25.8, while that from external samples was only marginally higher at 28.4 and so it can be concluded that a similarly high level of RNA was found in fresh samples and in those that had been sent by post.
Sensitivity and specificity of the MLN FNA FCoV RT-qPCR assay
FCoV was detected by RT-qPCR in 18/20 cats with non-effusive FIP (group D). Two extracts contained no detectable FCoV RNA, although both contained ample reference gene RNA, and therefore the test sensitivity was 90%. Interestingly, these samples represented the only neurological cases of FIP in this group and this association was found to be statistically significant (P = 0.0053, Fisher’s exact test). FCoV Ct values varied between 22.7 and 38.2 and these showed a moderate correlation with GAPDH Ct values (r = 0.72, P <0.01). This relationship is illustrated in Figure 2.

Relationship between feline coronavirus (FCoV) and GAPDH Ct values for non-effusive feline infectious peritonitis samples where FCoV was detected. A moderate positive correlation (r = 0.72, P <0.01) was detected between Ct values of the ‘test’ gene, FCoV, and the reference host control gene, GAPDH. Thus, broadly, the lower level of host RNA detected, the lower level of FCoV detected
Of the 26 cats in the study that did not have FIP (control groups P and N), FCoV was detected in only one cat and thus the overall test specificity was 96.1%. In practice, an FCoV seronegative status would tend to rule out a diagnosis of FIP and therefore this assay has particular relevance to the cohort of non-FIP seropositive cats; the specificity with respect to this group was 87.5%. The positive sample, with a Ct value of 23, was from cat P04, which was subsequently diagnosed with suppurative bronchopneumonia. Sections from kidney, lung, liver and spleen were analysed by immunohistochemistry, but FCoV antigen was not detected in any of the tissues examined. A 2 × 2 contingency table was generated to evaluate the performance of the MLN FNA RT-qPCR assay compared with standard diagnostic tools for FIP. The results demonstrated a high inter-rater agreement, which was almost perfect (κ = 0.88; 95% CI 0.75–1.0).
Discussion
A sensitive, specific and minimally invasive method for supporting or refuting a diagnosis of non-effusive FIP is currently required. A PCR and sequencing-based method has recently been developed, which targets a mutated form of FCoV.7,12,32 Although a positive result may be supportive of FIP, the assay suffers from unacceptably low sensitivity (6.5%) when applied to blood samples, 32 and a recent study concluded that gene mutation analysis does not substantially improve the ability to diagnose FIP as compared with detection of FCoV alone. 12 This leads to the supposition that an alternative approach, the use of a PCR protocol capable of detecting the virus in a key anatomical site, ie, mesenteric lymph node tissue, may have more diagnostic utility for suspect cases of non-effusive FIP.
Laparotomy for the collection of biopsy material is a potentially stressful and risk-associated intervention. In contrast, sample collection by ultrasound-guided FNA is a far less invasive procedure and therefore an opportunity exists to develop a novel assay for FIP diagnostics using this methodology.
While cytology of effusions in FIP is useful in establishing alternative diagnoses such as neoplasia or bacterial peritonitis, cytology of enlarged MLN FNA often provides limited clear diagnostic information, with cytology often described as consistent with reactive hyperplasia (unpublished observation). Norris et al described reactive hyperplasia in 4/5 cases of confirmed FIP where cytology had been performed on MLN FNA and 1/5 cases as pyogranulomatous inflammation. 33 In all cases, these observations are non-specific characteristics that are merely suggestive of FIP, and add no solid support.
A PCR-based assay, however, offers the potential of improved performance and so the present study set out to investigate whether detecting viral RNA in FNAs of MLNs could be used to support a diagnosis of FIP. As a first step, we demonstrated that both host and FCoV RNA can be reliably detected in samples from MLN FNAs, as well as in MLNBs. The results of the GAPDH RT-qPCR control assay confirmed that sufficient quantities of host RNA can be recovered from MLN FNA samples. Importantly, a very similar level of RNA was recovered from fresh MLN FNA samples prepared in the laboratory and MLN FNA samples that had been collected by submitting veterinary surgeons and sent via the postal system, without any form of preservative. This means that the samples submitted without the use of nucleic preservatives or refrigeration are suitable for use with this assay.
Enlarged MLNs are frequently observed in FIP cases; in all five FIP cases in the present study, where lymph node size was recorded in the clinical history, it was described as enlarged. It is from such enlarged MLNs that we would advise taking FNAs. However, if MLNs are of normal size, even using ultrasound guidance, then accessibility and stabilisation of the lymph node are likely the most important factors to allow aspiration of adequate material to test. Other studies suggest sampling from the kidney, and although this organ may be easier to sample, experimental infections provide evidence of lower viral load in these tissues. 34 Our study, focusing on sampling enlarged MLNs, builds on the work of Kipar et al, 35 who detected FCoV viral RNA by RT-PCR in the MLN of 13/15 (87%) of cats with FIP. However, as FCoV is primarily an enteric pathogen, its presence in lymph nodes draining the gastrointestinal tract may also be anticipated in FCoV-infected cats without FIP. 35 Thus, the study was designed to address two issues: whether, in principle, RT-qPCR could detect the virus in MLN FNA RNA preparations and, if so, whether it could be a sensitive and specific diagnostic method for FIP investigation.
Samples representing 25/26 (96.1%) seronegative or seropositive cats without FIP did not generate a PCR product, and thus a diagnosis of FIP was not supported in these cases. FCoV RNA was detected in only one seropositive kitten, P04, which presented with diarrhoea, dyspnoea, a pleural effusion and a highly elevated white cell count. On the basis of histopathology, this cat was subsequently diagnosed with suppurative bronchopneumonia, although no bacteria were recovered from the biopsy material. While lesions typical of FIP were not detected by histopathology, the possibility that this cat suffered concurrently from FIP cannot be excluded.
This sample demonstrates that FCoV may be detected in the MLN of a small proportion of cats that do not have FIP. Notably, P04 had an intermittent history of diarrhoea, which increased in severity shortly before its death, although it is unknown whether this was associated with FCoV or not. The MLNs are the local draining lymph nodes for the intestinal tract and it is to be expected that at some point during enteric infection by FCoV there will be a transient viral presence in those nodes, following transport by macrophages. It may be hypothesised that, in terms of FIP diagnosis, there is the risk of a false-positive result if the animal is tested in this early period of infection. However, it should be appreciated that, in practice, this diagnostic test should only be applied when there is a strong index of suspicion of FIP, based on clinical presentation and other laboratory test parameters. This test is not designed to be a screening assay for healthy cats and its application would not be indicated in cases of enteric infection where diarrhoea is the principal clinical sign.
However, there remains the potential risk of detecting FCoV in cats experiencing an early FCoV infection, but which have nevertheless been tested because of a concurrent illness, presenting with clinical signs suggestive of FIP. A group of particular concern would be FCoV carrier cats. These individuals are persistently infected with FCoV in the gut and continually shed virus in the faeces; however, they rarely develop FIP. 36 We can report that MLN biopsy samples from two carrier cats persistently infected with FCoV, collected during the course of a previous study, 37 were found to be FCoV RNA negative (unpublished data).
In most instances, the first step in FIP diagnosis is to perform haematology, biochemistry and FCoV serology in order to assess the likelihood of the disease. The MLN FNA assay is likely to be most useful in cases where standard non-invasive diagnostic tests produce equivocal results or to further support a diagnosis in cases where FIP is strongly suspected. Eighteen of 20 (90%) cases were correctly classified as having FIP by the MLN FNA assay.
Two samples, D12 and D13, had been diagnosed histopathologically with neurological FIP and tested negative on FCoV RT-qPCR. This association was found to be statistically significant and was not a wholly unexpected finding. FIP is commonly subdivided into effusive and non-effusive forms. On the basis of these results, and those of others,19,38,39 further classification of non-effusive cases may be useful with respect to determining appropriate diagnostic approaches. In the neurological manifestation of FIP, the virus may have been sequestered in the neural tissues, and thus absent from the MLNs. In one of these two cases, D13, FCoV was detected by RT-qPCR in the cerebrospinal fluid. Similarly, in cases of suspected FIP-associated uveitis, the virus may be detected in aqueous humour (unpublished observation). Further data are required in FIP cases with neurological manifestations of FIP, and it is possible that among cases of this type the sensitivity of this assay may be limited. Additionally, further studies with larger numbers of non-FIP, FCoV-seropositive cats are required to more accurately measure the specificity of MLN FNA FCoV RT-qPCR for this presentation of FIP.
The overall sensitivity of the assay was 90% (FCoV detected in 18/20 FIP cases) and the specificity was 96.1% (FCoV not detected in 25/26 controls). Very good agreement was demonstrated between the MLN FNA assay and the standard diagnostic tools, with an inter-rater agreement (κ) of 0.88. Thus, overall, the results of the study suggest that presence of FCoV in the MLN of systemically ill cats is associated with a diagnosis of FIP. Therefore, this test has value aiding the diagnosis of FIP in cats with a high index of suspicion of disease. This assay is not proposed as a standalone method to diagnose FIP and should be used to complement the standard suite of haematological, biochemical and serological tests currently in use.
Conclusions
The results of this study are encouraging: FCoV RT-qPCR of FNA of the MLN is a useful tool to aid the diagnosis of non-effusive FIP. This assay can detect FCoV in MLN FNAs from confirmed FIP cases while not detecting FCoV in samples from seronegative cats and the majority of FCoV-seropositive cats without FIP. While having limited power to identify neurological cases of FIP, the test is highly sensitive when applied to suspect ‘classic’ systemic FIP cases. As the technique is far less invasive than traditional biopsy and provides useful diagnostic information, it represents a useful addition to the suite of current diagnostic methods for FIP.
Supplemental Material
Supplementary Material 1
RNA quantification and RT-qPCR results for matched MLN FNA and MLN biopsy RNA preparations in a pilot study.
Supplemental Material
Supplementary Material 2
RNA quantification and RT-qPCR results for MLN FNA and MLN biopsy RNA preparations.
Footnotes
Acknowledgements
We would like to thank the diagnostic teams within the Veterinary Diagnostic Service at the University of Glasgow for their efforts in the collection and analysis of the samples processed in this study. We are grateful to Dr Marina Meli for aiding us in setting up the FCoV RT-qPCR assay. We are grateful to Dr Pablo Nart for perfecting the protocol for extracting FCoV RNA from tissue samples using the gentle MACS M tube. Above all, we sincerely thank the many people who, despite their grief, generously donated the remains of their deceased pet for post-mortem examination for this project, enabling us to eschew the use of experimental cats, and we thank their veterinary surgeons for sending the pet samples to us.
Supplementary material
The following files are available online:
Supplementary material 1: RNA quantification and RT-qPCR results for matched MLN FNA and MLN biopsy RNA preparations in a pilot study.
Supplementary material 2: RNA quantification and RT-qPCR results for MLN FNA and MLN biopsy RNA preparations.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The Angelica Trust funds FIP research at the University of Glasgow. The John Robertson Bequest (University of Glasgow) and the BBSRC REP funded the studentship of Wendy Kwok.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.