
Abstract
Case series summary
Mediastinal cysts were diagnosed as incidental findings in six cats evaluated for non-thoracic disease, including staging for historical bladder leiomyosarcoma, flea dermatitis and hairballs, and hyperthyroidism. Radiographically, the cysts appeared as soft tissue opacities cranial to the heart. Ultrasound revealed the masses to be thin-walled, single lumen, anechoic, fluid-filled structures. One cat also had thoracic and abdominal CT performed for cancer staging; the CT revealed a well-defined, fluid-attenuating mass without peripheral contrast enhancement in the cranial mediastinum. Fine-needle aspiration confirmed acellular fluid consistent with a cyst in five cases; in one case the cyst ruptured during aspiration and no fluid was obtained. Post-aspiration, all masses were no longer visible with ultrasound or radiographs. No treatment was recommended for the cysts. Long-term follow-up (2–9 years post-diagnosis) was available in all six cats. The cysts recurred in five cats but were never associated with clinical signs.
Relevance and novel information
Mediastinal cysts are an important benign differential for cranial mediastinal masses in cats. Treatment for the cysts does not appear to be indicated. This series also includes the first CT description of this clinical entity.
Introduction
Cranial mediastinal masses may be caused by a range of conditions.1–3 Neoplasia is the most frequent cause of such masses in the cat, with differentials including lymphoma, thymoma (including cystic thymoma), ectopic thyroid tissue, heart-based tumors and metastatic neoplasia.1,3 Non-neoplastic conditions causing a mediastinal mass are rare and include abscess or granuloma, benign thymic hyperplasia, hemorrhage and cysts.2,3
The origins of the few reported cysts causing cranial mediastinal masses in the cat include thymic, branchial, parathyroid, pericardial and mediastinal.1–14 The first description of a benign cyst of mediastinal origin was in a case report of a cat with oral squamous cell carcinoma. 11 A 5 cm × 3 cm × 3 cm mass was noted in the cranial mediastinum on radiographs. Aspiration under fluoroscopic guidance revealed 25 ml of clear, colorless, acellular fluid with a specific gravity of 1.005 and a protein content <2.5 mg/dl. The mass could not be visualized on radiographs after aspiration. The cat was euthanized owing to the oral tumor. Post-mortem examination revealed a thin-walled cystic structure adherent to the external surface of the cranial left mediastinum. The cyst was unilocular and lined by non-ciliated simple to pseudostratified, low cuboidal cells. Histologically, the cyst resembled mediastinal pleura and was thus called an idiopathic mediastinal cyst.
Three other mediastinal cysts presumed to be such based on ultrasonographic appearance and cystic fluid cytologic analyses, were later reported in a series of non-cardiac thoracic ultrasound cases. 1 None of these cats had long-term follow-up. A retrospective study of nine cats diagnosed with cranial mediastinal cysts was reported in a veterinary radiology journal over a decade ago. 12 In this paper, follow-up thoracic imaging was available in less than half of the cats, with a follow-up of 1–40 months.
This report describes six cases of feline mediastinal cysts with long-term follow-up ranging from 2–9 years. Additionally, CT scan findings of a mediastinal cyst are described for the first time in the literature. This benign condition does not require intervention and carries an excellent prognosis.
Case series description
Six cats were identified with incidental diagnoses of a mediastinal cyst. The cats ranged in age from 9–17 years (mean 13 years, median 13.5 years). Four were female spayed and two were male castrated. Five were domestic shorthaired cats and one was a Norwegian Forest cat. Five cats were presented to their primary care veterinarian for a wide range of concerns, including chronic nasal discharge, flea infestation and decreased appetite, acute onset of vomiting and diarrhea, chronic vomiting and weight loss with polyphagia, and weight loss after having been missing from home. All cats were referred after thoracic radiographs revealed a cranial mediastinal mass of soft tissue opacity. The remaining cat was being monitored for metastasis with radiographs and abdominal ultrasound every 4 months after a bladder leiomyosarcoma resection 1.5 years previously. None of the cats had clinical signs related to the cranial mediastinal mass.
Imaging performed on all cases at the referral hospital included thoracic radiographs and cranial mediastinal ultrasounds. All thoracic radiographs revealed a soft tissue opacity round-to-oval mass cranial to the heart, the longest diameter of which ranged from 1.3–4.4 cm (mean 2.4 cm, median 2 cm). Cranial thoracic ultrasound confirmed a rounded, anechoic structure cranial to the heart in all cases. Ultrasound-guided fine-needle aspiration was performed with a 6 cc syringe and a 22 G ¾ inch needle in all cats. Five of the aspirates obtained clear fluid, with the volume ranging from 1–6 ml (mean 2.9 ml, median 3 ml). Fluid analysis of the five samples revealed colorless fluid with a specific gravity <1.005–1.007, protein <1.0g/dl and cells ranging from 0–92 (red blood cells) cells/μl (mean 20 cells, median 0 cells). In the remaining cat, aspiration did not provide a sample. After aspiration, none of the lesions could be seen with ultrasound, consistent with drainage and/or rupture of a cyst.
The cats were infrequently re-evaluated based on their primary disease process. Recurrence of the cyst was noted on thoracic films in five of the cats, at a time point ranging from 9 months to 3 years post-diagnosis. In the one cat without cyst recurrence, the only imaging recheck was radiographs taken 9 months after aspiration, and no recurrence was noted at that time.
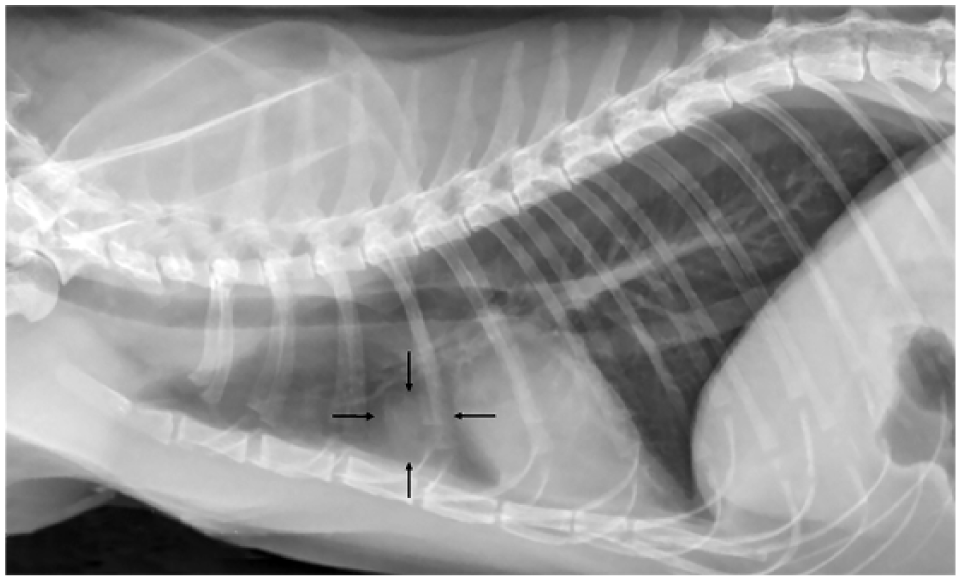
The only cat that had serial thoracic imaging performed was the cat with the previously excised bladder leiomyosarcoma; radiographs in this patient were made every 4 months. When first identified, the cyst was 1.3 cm × 1.3 cm (Figure 1) and was aspirated, at which point repeat radiographs showed no evidence of the mass. Nine months later, thoracic radiographs revealed recurrence of the mediastinal cyst; ultrasound showed the mass to be 1.65 cm × 0.75 cm (Figure 2). Four sets of thoracic radiographs taken over the following 2 years revealed slow growth of the mediastinal cyst, with a 50% increase in size (Figure 3). No clinical signs were noted. Six years after the initial mediastinal cyst diagnosis, the cat was evaluated for a mass in the left horizontal ear canal. A full-body CT was performed for surgical staging; a 3 cm × 4 cm fluid-attenuating mass in the cranial mediastinum was seen (Figure 4). The mass had no evidence of peripheral contrast enhancement, or ‘ring effect’, and was not causing displacement of any intra-thoracic structures. No other abnormalities, such as enlarged or irregular lymph nodes, were noted. The ear canal mass was inflammatory on biopsy and resolved with prolonged topical medical management.
Left lateral thoracic radiograph showing soft tissue opacity structure cranial to the heart (arrows)

Transverse parasternal ultrasound image of the mass cranial to the heart (cranial is to the right); distal enhancement can be seen, consistent with fluid

Left (a) lateral and (b) ventrodorsal radiographs showing enlarged soft tissue opacity mass cranial to the heart (arrows)
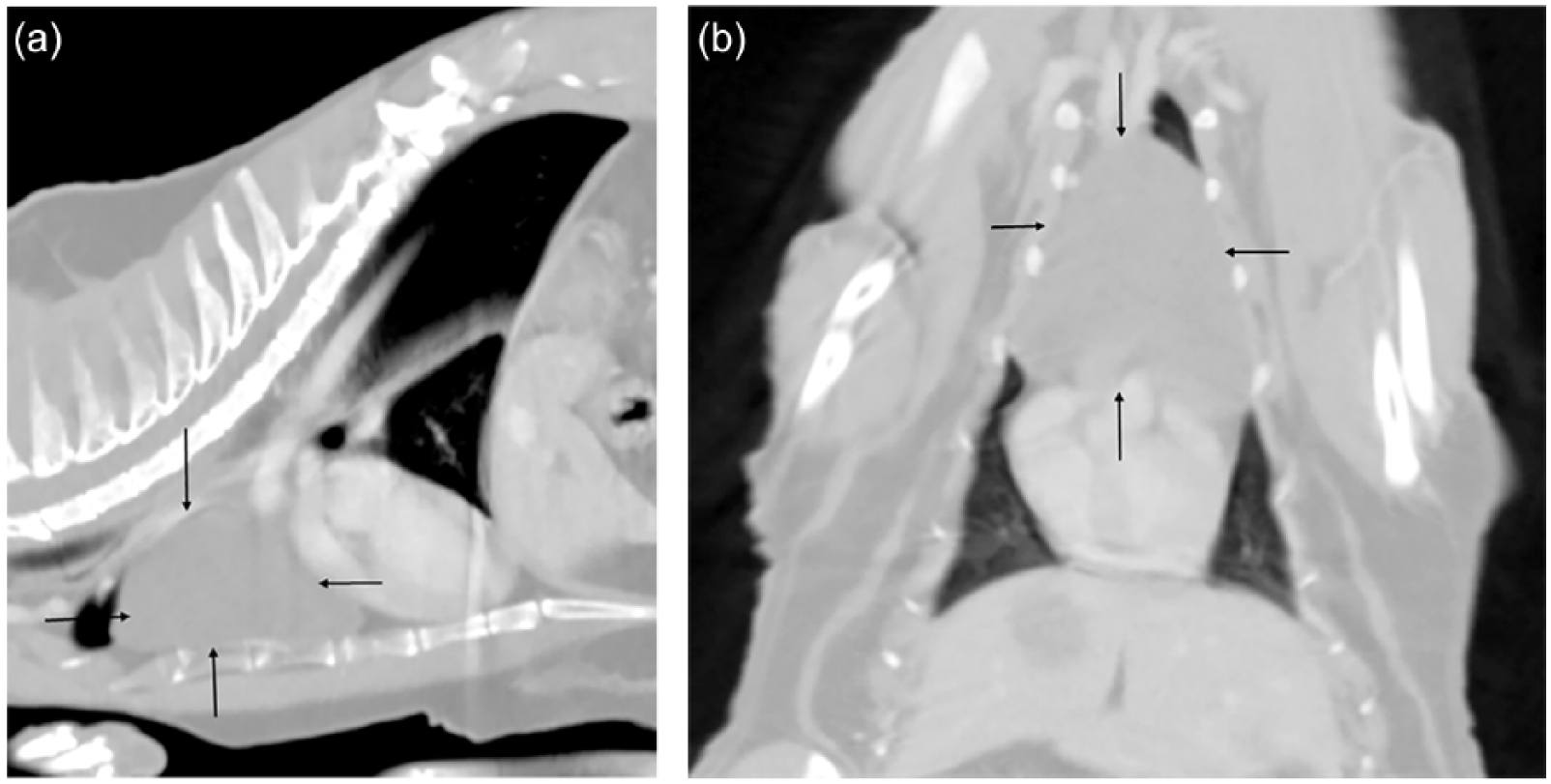
CT post-contrast (a) sagittal and (b) dorsal views of fluid attenuating non-ring enhancing mass cranial to the heart (arrows)
None of the cats developed signs related to the mediastinal cysts. Two cats were lost to follow-up at 2.5 and 4 years post-cyst diagnosis, two cats were euthanized owing to unrelated problems (methimazole bone marrow toxicity and chronic kidney disease) at 2.5 and 7 years post-diagnosis, and, at the time of writing, two cats were alive at 4 and 9.5 years post-diagnosis.
Discussion
Cranial mediastinal masses in cats are most frequently associated with neoplasia and generally carry a poor to grave prognosis. It is important to also consider non-neoplastic causes for masses in this area, as the often improved prognosis for such etiologies may greatly change the approach to case management. In a review of thymic pathology in 30 cats, six were found to have non-neoplastic diseases. 4 One had a cystic thymus previously described in a case report, where ultrasound showed well-defined solid tissue with interspersed multi-locular cysts. 5 Fluid aspirated from the mass was pink, cloudy, and with a predominance of lymphocytes. The remaining five cases did not report laboratory or imaging results. Of these, four had conditions that may have caused a mass effect on radiographs, including: two thymic hyperplasia; one thymic amyloidosis, causing enlargement of the thymus on post-mortem examination; and one thymic and mediastinal hemorrhage. Histopathology of these cases showed the majority of the thymus to be of cellular density, not cystic.
Thymic, branchial, parathyroid, pericardial and mediastinal cysts have been previously reported in the cat.1–14 Branchial cysts develop from remnants of the second pharyngeal pouch, 6 and have been definitively reported in three cats: one in the ventral cervical region and two in the cranial mediastinum, associated with the thymus.7,8 Cats affected with thymic branchial cysts had pleural effusion and were dyspnic. One died of respiratory failure and the other was euthanized. At necropsy, the branchial cysts were multi-lobulated and contained proteinaceous, mucinous material.A mediastinal parathyroid cyst found incidentally on radiographs has been described. 9 Surgical excision with histopathology revealed a multi-loculated mass lined by cuboidal-to-columnar ciliated epithelium and containing eosinophilic proteinaceous fluid.Pericardial cysts have very rarely been reported in cats. Pericardial cysts in humans typically arise in the cardiophrenic angle, adjacent to the diaphragm. Such cysts are usually attached to the pericardium, and 20% communicate with the pericardial sac. 15 The only reports of histologically confirmed spontaneous pericardial cysts in small animals are in dogs, all of which had cysts within the pericardial sac. 16 Affected animals were young, consistent with what is seen in congenital pericardial cysts of humans, presented with cardiac tamponade, and had bloody, brown-tinged fluid within the cysts. A recent case report described a 2-year-old Maine Coon cat with a pericardial cyst that developed secondary to a surgical repair of a peritoneopericardial diaphragmatic hernia. 13
Feline infectious peritonitis presenting as a cystic mass in the mediastinum was described in an 8-month-old Maine Coon cat with a 10 day history of anorexia and lethargy. 14 On physical examination, the cat was tachycardic, tachypneic and dyspneic. Severe hyperproteinemia (104 g/l; reference interval 54–78 g/l) was documented. CT scan revealed a 78 mm × 50 mm × 37 mm cyst-like structure in the left thorax, which was associated with severe right displacement of the mediastinum and atelectasis of the right middle and caudal lung lobes. Post-contrast, the cyst showed peripheral contrast enhancement, or ‘ring effect’. Enlarged cranial mediastinal lymph nodes had moderate enhancement. Fine-needle aspiration yielded a frothy, straw-colored modified transudate with a high protein content (6.6 g/ dl) and low cell count (<1000/μl). Euthanasia was performed and necropsy confirmed a fluid-filled cyst-like structure arising from the mediastinum, occupying a large portion of the left thorax. Severe, diffuse, pyogranulomatous inflammation of the pleura, pericardium, lung and kidney was also noted. Immunohistochemistry of the cyst wall and pulmonary and renal lesions were positive for feline coronavirus antibody.
Few reports exist in the literature of mediastinal cysts. The first description of this condition was most likely in a case report of a pericardial cyst in a cat. This cyst was in the mediastinum, not the pericardial sac, and was noted as an incidental finding in a hyperthyroid cat. 10 The cyst was similar to the cases in the current report both in radiographic and ultrasonographic appearance, as well as on fluid analysis. The cyst could no longer be seen on radiographs immediately after fine-needle aspiration, and recurrence was noted at a 6 month recheck. Owing to the difference in presentation of this cat from both humans and dogs with pericardial cysts, it seems likely that the cyst was actually of mediastinal origin. The following year, the term idiopathic mediastinal cyst was applied in the case of the cat with oral squamous cell carcinoma and an incidental cranial mediastinal mass, which, on necropsy, was diagnosed as a cyst resembling mediastinal pleura. 11 Since then, 12 cases of mediastinal cysts have been described in two papers.1,12 Only three of the cats had long-term follow-up exceeding 15 months, with the majority having no follow-up reported. None of the cases had CT imaging described.
In this series of six cats with mediastinal cysts, the cysts were incidental findings, they radiographically appeared as soft tissue opacities cranial to the heart, they were unilocular on ultrasonographic examination, and they contained clear, acellular fluid with a low specific gravity and protein. The CT of the cyst in one cat revealed a well-defined, fluid-attenuating mass in the cranial mediastinum, without evidence of ring-enhancement after contrast administration. This is the first description of the CT findings of a mediastinal cyst. All six of the cats in this report had long-term follow-up, ranging from 2–9 years. Five of the cats showed radiographic evidence of cyst recurrence, ranging from 9 months to 3 years post-diagnosis, and none of these patients demonstrated clinical signs related to the cysts.
Conclusions
Despite recurrence in the majority of cases, all of the cats in this series had long-term follow-up and remained asymptomatic. Some authors have recommended surgical resection of cysts in the cranial mediastinum if they recur following drainage. 3 Based on extended follow-up in this series of cases, drainage or excision of mediastinal cysts does not appear to be indicated. Mediastinal cysts need to be considered as a benign differential in cats with a cranial mediastinal mass; on CT the cyst will appear as a well-defined, fluid-attenuating mass without evidence of contrast ring-enhancement. These cysts carry an excellent prognosis.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.