
Abstract
Objectives
The aims of the study were to identify the ultrasonographic findings in cats with acute kidney injury (AKI) and to assess whether they had prognostic value.
Methods
This was a descriptive case series. A search of the computerised records of the Queen Mother Hospital for Animals (Hatfield, UK) was performed for cats presenting with AKI between 2007 and 2016. Patients were excluded if they had historical data consistent with chronic kidney disease. Ultrasound images were reviewed for the presence of six renal ultrasonographic abnormalities: nephromegaly, cortical and medullary echogenicity, pyelectasia, and retroperitoneal and peritoneal fluid. Ultrasonographic findings were assessed individually and cumulatively to give an ultrasound score out of 6. Ultrasonographic findings were assessed for association with oligouria/anuria and survival.
Results
Forty-five cats with AKI fulfilled the inclusion criteria. In total, 6.7% (3/45) of cats had normal renal size and architecture. The most common renal ultrasonographic findings were nephromegaly, pyelectasia and increased renal echogenicity. The presence of retroperitoneal fluid was associated with oligouria/anuria. Total ultrasound score (out of 6) was significantly associated with oligouria/anuria and 6 month survival.
Conclusions and relevance
Ultrasonographic findings are common in cats presenting with AKI. The increasing number of renal ultrasonographic abnormalities and the presence of retroperitoneal fluid alone are associated with oligouria/anuria and a higher ultrasound score may suggest a poorer long-term prognosis.
Introduction
Acute kidney injury (AKI) is defined as an acute and abrupt decrease in renal function resulting in abnormal glomerular filtration rate, tubular function and urine output, and can be graded to encompass a continuum of functional and parenchymal damage. 1 The International Renal Interest Society (IRIS) has developed guidelines for the diagnosis of AKI. 1 These guidelines include ‘imaging findings suggestive of AKI’ as a diagnostic criterion, but there is no guidance given regarding what findings are expected.
Ultrasonography is a non-invasive procedure that can be performed in the majority of unstable patients, making it a useful first-line tool in the investigation of AKI. It can be used to assess renal dimensions, characterise the pelvis and parenchymal echogenicity, and may have a role in identifying the causal mechanism of kidney injury. 2 Information relating to renal size and renal echogenicity are suggested to be the most valuable in diagnosis and decision-making when managing renal disease in humans.3,4
Published ultrasonographic findings in dogs and cats with AKI include increased renal size, increased cortical echogenicity, the presence of perirenal fluid, medullary rim sign, pyelectasia, increased echogenicity of the perirenal fat and abnormal echogenicity of the urine present in the pelvis.5,6 Some of these findings have been suggested to be associated with a particular aetiological cause and prognosis.7–10 A recent study comparing azotaemic cats with non-azotaemic cats found that perirenal fluid was the ultrasonographic finding most associated with azotaemia. 11
The aims of this study were to identify the ultrasonographic findings in cats with AKI and to assess whether any specific findings had a prognostic value. The hypotheses were that most feline AKI patients would have renal ultrasonographic abnormalities and some findings would be associated with increased mortality.
Materials and methods
The clinical records of the Queen Mother Hospital for Animals (Hatfield, UK) were searched using a computerised search for cats with a diagnosis of AKI of between 2007 and 2016. For patients to be included in the AKI group they should have satisfied the following criteria based on the IRIS (2013) guidelines for the diagnosis of azotaemic AKI: creatinine ⩾141 μmol/l or above the reference interval of the individual analyser; and one or more of the following: urine analysis compatible with AKI (glucosuria, proteinuria with an inactive sediment or renal casts) or persistent, documented clinical oliguria or anuria (<1 ml/kg/h). Clinical oligouria/anuria was determined retrospectively based on the use of furosemide or continuous renal replacement therapy. Patients were excluded if they had any historical or clinical findings or clinicopathological data consistent with chronic kidney disease (chronic polyuria or polydipsia, body condition score <2/9 or the presence of a non-regenerative anaemia).
Static ultrasound images were retrieved from the Picture Archiving and Communication System (PACS) server (Osirix) and were reviewed in a randomised manner by a board-certified radiologist blinded to the patient diagnosis. Ultrasound images of the kidneys were assessed for the following parameters: nephromegaly (defined as kidney length >4.4 mm in the maximal sagittal view), 5 cortical and medullary echogenicity (hyper-, iso- or hypoechoic to the liver and spleen)5,6 and pyelectasia (measured from the pelvic crest to the beginning of the ureter). Additional findings, including the presence of uroliths and the presence of a hypo- (halo sign) or hyperechoic (medullary rim sign) echogenicity at the corticomedullary junction, were also recorded. Normal renal architecture was identified by three findings in the sagittal view: bright central echo complex (the renal sinus and peripelvic fat), a hypoechoic region surrounding the pelvis (the medulla) and a peripheral zone of intermediate echogenicity (the renal cortex). 12
The degree of pyelectasia was evaluated as follows: if the shape of the pelvis was still triangular (⩽4 mm) pyelectasia was considered mild (Figure 1a), if the pelvis was oval shaped (5–10 mm) pyelectasia was considered moderate (Figure 1b) and if there was reduction in cortical size (pelvis >10 mm) pyelectasia was considered severe (Figure 1c). Significant pyelectasia was defined as renal pelvis measurement of >4 mm.

Pyelectasia: (a) mild, (b) moderate and (c) severe
An ultrasound score out of 6 was given to each patient. This score was comprised of 1 point for each of the six ultrasonographic findings: nephromegaly, increased cortical echogenicity, increased medullary echogenicity, pyelectasia, the presence of retroperitoneal fluid and the presence of peritoneal fluid.
The need for furosemide or continuous renal replacement therapy was documented in order to classify a patient as oligouric/anuric. The suspected aetiology of the AKI and survival to discharge were also documented.
A Shapiro–Wilk test was used to assess the data for normality. For normally distributed data the mean and SD were calculated, whereas for non-normally distributed data the median and range were calculated. Descriptive statistics on the population of cats was performed using a commercial statistical application (SPSS Stasitics, Version 22.0; IBM). Binary univariable and multivariable logistic regression analysis was used to evaluate associations between ultrasonographic findings and survival, and presence of oligouria/anuria. Independent ultrasound variables included in the logistic regression analysis were nephromegaly, increased cortical echogenicity, increased medullary echogenicity, pyelectasia, presence of retroperitoneal fluid and the presence of peritoneal fluid. Univariable logistic regression was used to evaluate the association between ultrasound score and survival to discharge, survival at 6 months and the presence of oligouria/anuria. P values were computed for each predictor in each regression analysis, alongside an odds ratio (OR) and 95% confidence intervals (CIs). A P value of <0.05 was considered significant.
Results
Forty-five cats with AKI fulfilled the inclusion criteria. The median age of the cats was 42 months (range 2–154 months). There were 29 domestic shorthair cats, four domestic longhairs and 12 pedigrees. Twenty-two cats were male neutered, 19 female neutered and four were male entire. The median weight of the cats was 4.18 kg (0.9–8.2 kg, n = 42). The median creatinine of the cats was 864 μmol/l (range 182–2576 μmol/l; n = 39).
The cause of AKI was identified in 29/45 cats. Based on historical exposure to toxins and supporting biochemical findings ethylene glycol toxicity was diagnosed in 4/45 cases, lily toxicity was reported in 2/45 cases and other toxins were suspected in 8/45 cases. Furthermore, 6/45 cases had a recent history of non-steroidal anti-inflammatory drug (NSAID) administration and 4/45 cases had a history of trauma. Identification of a ureterolith and ureteral obstruction on ultrasound was reported in 5/45 cases.
Nephromegaly was present in 68.9% (31/45) of cats with AKI and, of these, 35.5% (11/31) had unilateral nephromegaly. Median renal length for all cats was 4.5 cm (range 2.7–5.4 cm). Pyelectasia was present in 57.8% (26/45) of cats with AKI and this was unilateral in 11.5% (3/26) of cats; the median pelvic dimension was 2.5 mm (range 0.5–15 mm). Pyelectasia was considered mild in 79.6% of cases (39/49), moderate in 12.2% of cases (6/49) and severe in 8.16% of cases (4/49). All cats had received intravenous fluid therapy prior to ultrasound. Of the 26 cats with pyelectasia 26.9% (7/26) of cats were documented to have uroliths, of which 3/7 had ureteroliths only, 2/7 had both ureteroliths and nephroliths, and 2/7 had only nephroliths (Figure 2a). In total, 75% (3/4) of patients with severe pyelectasia were documented to have ureteroliths. Overall, the presence of uroliths in AKI cats was 15.6% (7/45). Increased cortical and medullary echogenicity was documented in 40% (18/45) and 51.1% (23/45) of cats, respectively. All cats with increased cortical echogenicity had increased medullary echogenicity (Figure 2b). A halo sign was detected in single cat. In total, 33.3% (15/45) of the cats had retroperitoneal fluid (Figure 2c) and 46.7% (21/45) of the cats had peritoneal fluid. The total ultrasound score ranged from 0–6.

Ultrasonographic findings in cats with acute kidney injury. (a) Nephrolith, (b) increased cortical and medullary echogenicity and (c) retroperitoneal fluid
Nephromegaly was identified in 100% (2/2) of cases of lily toxicity, 75% (3/4) of cases of ethylene glycol toxicity, 75% (3/4) of trauma cases, 60% (3/5) of cats with ureteroliths and 50% (3/6) of cats with NSAID toxicity. Cortical and medullary increased echogenicity was identified in 75% (3/4) of cats with ethylene glycol toxicity, and in 50% (2/4 and 1/2) of those cats with history of trauma and lily exposure. Significant pyelectasia was seen in 100% (5/5) of cases with confirmed ureteroliths and 75% (3/4) of trauma cases. Retroperitoneal fluid was seen in 50% (1/2) of reported lily intoxication and between 16.67% and 25% for other causes. Peritoneal fluid was present in 50% (2/4) of cases of ethylene glycol toxicity and in 40% of cases of ureteroliths (Table 1).
Ultrasonographic findings and cause of acute kidney injury
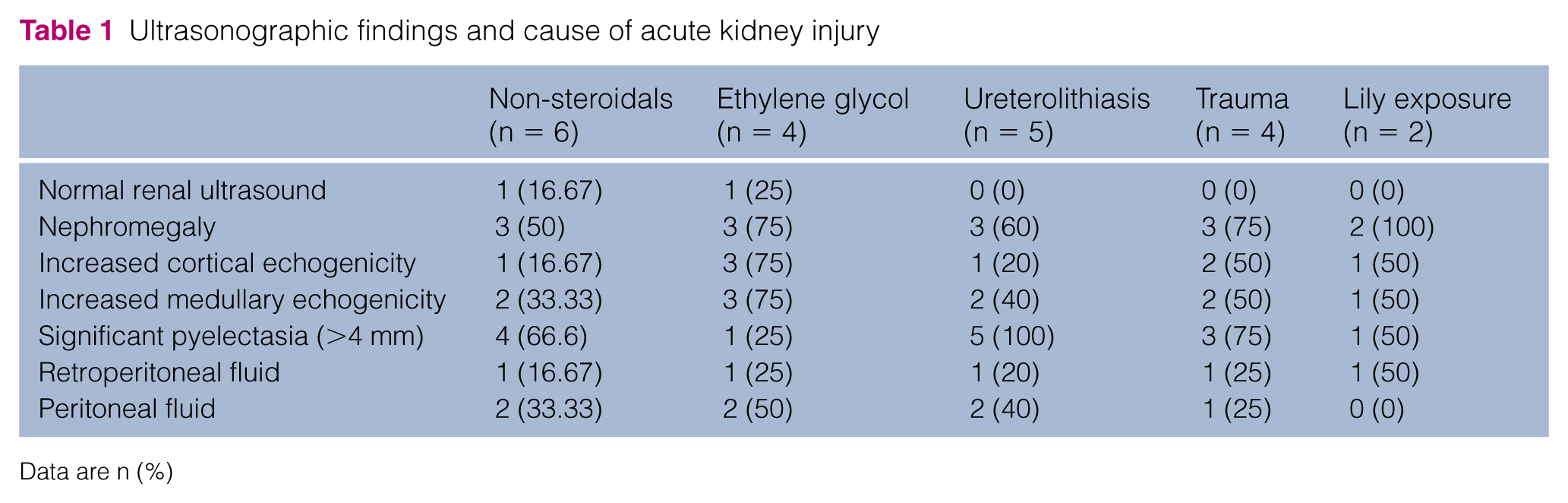
Data are n (%)
Out of the 45 cats with AKI, 42.2% (19/45) survived to discharge and 35.6% (16/45) were alive at 6 months. All patients that died were euthanased as a result of their disease.
Univariable and multivariable logistic regression showed that no single ultrasonographic finding or total ultrasound score was statistically associated with the survival to discharge (Table 2). However, there was a statistically significant association between the total ultrasound score and 6 month survival time (P = 0.029, OR 0.628, 95% CI 0.415–0.953).
Univariable logistic regression analysis for ultrasonographic findings associated with survival to discharge in cats with acute kidney injury

There was a statistically significant association between the total ultrasound score and the presence of oligouria/anuria (P = 0.04, OR 1.507; 95% CI 1.02–2.229) and, when considering the individual ultrasonographic findings, there was a statistically significant association between the presence of retroperitoneal fluid and oligouria/anuria (P = 0.006, OR 8; 95% CI 1.8–34.9) in both univariable and multivariable analysis (Table 3).
Univariable and multivariable logistic regression analysis for ultrasonographic findings associated with the presence of oligouria/anuria

Data in bold are statistically significant
Discussion
This retrospective study illustrates that abnormalities in ultrasonography are common in cats with AKI. Renal and perirenal ultrasonographic abnormalities were reported in >90% of cases, and >50% of cases had at least three ultrasonographic abnormalities of the recorded study parameters, suggesting the more renal/perirenal abnormalities with compatible history and physical examination findings there are, the more likely the patient is to have AKI.
Nephromegaly is the most commonly cited abnormality in AKI and this study supports this, with approximately 70% of patients with AKI having nephromegaly. 5 This is similar to the reported findings in dogs with leptospirosis and renal lymphoma; 50% (10/20) and 80% (8/10), respectively.8,10
The second most common ultrasound finding in our study was pyelectasia, reported in approximately 60% of cases. Pyelectasia is considered a non-specific finding and should be interpreted with caution as it has been reported that feline patients with clinically normal renal function with evidence of diuresis have recorded pelvic diameters up to 3.4 mm. 13 All patients had been referred and therefore had intravenous fluid administration for an unknown period of time prior to ultrasound, which may be the cause of mild pyelectasia seen in some of these animals. Sub-categorising pyelectasia into mild, moderate and severe, based on the effect of pyelectasia on the rest of the renal parenchyma, was useful, especially when attempting to determine the underlying cause of AKI. Pyelectasia was present in all cases (5/5) diagnosed with ureteroliths and 75% (3/4) of patients with severe pyelectasia were documented to have uroliths. These findings suggest, alongside previous literature, that severe pyelectasia may be sufficient enough to support a diagnosis of ureteral obstruction.11–16
Increased renal echogenicity has been reported in a wide range of renal diseases, including glomerular and interstitial nephritis, acute tubular necrosis, nephrocalcinosis and end-stage renal disease. 4 In the current study 22/45 (48.9%) patients had increased renal echogenicity; of these 77% (17/22) had both increased cortical and medullary echogenicity. Increases in cortical echogenicity alone should be interpreted with caution as proximal tubular lipidosis occurs in normal cats and has been shown to increase renal cortical echogenicity in otherwise architecturally normal kidneys.17,18 Furthermore, renal echogenicity has been shown to poorly correlate with histopathological findings in cats with chronic renal disease. 19
Increased cortical and medullary echogenicity was detected in 75% (3/4) of cases with ethylene glycol toxicity. This is similar to a previous study, which reported a mild-to-marked increased echogenicity in all 15 patients suspected to have ethylene glycol toxicity. 7 In the same study, 7/12 dogs and 1/3 cats had a persistence of a reduced echogenicity at the corticomedullary junction, termed a halo sign, and this appeared to be associated with anuria. In the current study only one cat, suspected to have AKI secondary to trauma, was recorded as having a halo sign and this patient was not oligouric/anuric. The current study therefore questions the significance of a ‘halo sign’ as a sole marker of renal dysfunction. This is supported by other studies comparing the corticomedullary junction echogenicity in cats with and without renal disease.18,19 These studies suggest that either hypo- (halo sign) or hyperechoic (medullary rim sign) echogenicities cannot be used in isolation to characterise AKI.
In this study the presence of retroperitoneal fluid was associated with the presence of oligouria/anuria. It is unclear whether the association between retroperitoneal fluid and oligouria/anuria is a result of fluid overload, or if retroperitoneal fluid indicates the severity of the underlying disease. If fluid overload was the only cause of retroperitoneal fluid it would be expected that the presence of peritoneal fluid would also be associated with oligouria/anuria. Another potential mechanism of retroperitoneal fluid production is tubular back leak following increased permeability of proximal tubular epithelium secondary to nephrotoxins or ischaemic damage. 20 Holloway and O’Brien described 12 dogs and six cats with non-obstructive AKI and perirenal fluid, 9 of which 15/18 had bilateral perirenal fluid and no evidence of peritoneal or pleural fluid suggestive of fluid overload. The presence of retroperitoneal fluid has previously been shown to correlate with severity of azotaemia, supporting the theory that perirenal fluid is associated with severity of renal dysfunction. 11 In the current study, 6/15 cases with retroperitoneal fluid had reported toxin exposure and in another five cases the cause was unknown and therefore a potentially toxic cause, most of which are associated with poor outcome.
No ultrasonographic abnormalities were statistically associated with survival when considered in isolation. However, when using an ultrasound scoring system there was a trend towards significance with regard to survival to discharge and a statistically significant association with higher score and lower survival at 6 months, with most cases being euthanased within weeks of discharge. The failure to report a statistically significant finding between survival to discharge and ultrasound score may be the result of a type II error. A larger study population may have shown more significant results.
When considering the conclusions of the study one must be aware of the study limitations. This study was a retrospective study with a small sample size. The retrospective nature of the study only allowed review of static ultrasound images and this may have hindered image interpretation. Furthermore, we only captured patients with azotaemic AKI, thereby reducing the sample size. It is therefore possible that results are liable to type II statistical error, especially with regard to prognostication. Furthermore, the association between the ultrasonographic findings and aetiology could not be determined owing to the small number of cases in which a diagnosis was made. Finally, the study population itself was from a referral hospital. Therefore, all cases of AKI had prior fluid therapy at the primary care practice making it difficult to assess if the ultrasonographic findings, particularly pyelectasia, retroperitoneal fluid and peritoneal fluid, were due to fluid administration or as a result of the underlying disease process.
Conclusions
Ultrasonographic findings are common in cats with AKI. A 6-point scoring system, as used in this study, may be helpful in diagnosing AKI with accompanying historical, physical examination and biochemical findings. The increasing number of ultrasonographic findings and the presence of retroperitoneal fluid alone are suggestive of oliguria/anuria and a higher ultrasound score may suggest a poorer long-term prognosis. More studies are required to determine the use of this score further and to assess if there are individual ultrasonographic findings specific to aetiology.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.