
Abstract
Objectives
Cats are commonly affected by chronic kidney disease (CKD). Many reactive carbonyl intermediates and end products originating from the oxidative stress pathways are recognised as uraemic toxins and may play a role in CKD progression. The aim of the present study is to confirm whether carbonyl end-product formation is higher in cats affected by CKD and to assess whether an angiotensin-converting enzyme inhibitor (ACEi) might affect these hallmarks.
Methods
Twenty-two cats were divided into three groups: a control group (CG), cats with CKD and cats with CKD treated with an ACEi. Serum levels of pentosidine, carboxymethyllysine, advanced oxidation protein products, malondialdehyde, methylglyoxal and hexanoyl-lysine were measured. In addition, biochemical parameters and systolic blood pressure were evaluated. After checking for normality, comparisons between groups were performed followed by multiple comparison tests. P values ⩽0.05 were considered significant. Correlations between concentrations of the considered biomarkers and of the other metabolic parameters were investigated.
Results
Advanced oxidation protein products, malondialdehyde and hexanoyl-lysine concentrations were significantly higher in CKD and ACEi-treated groups compared with the CG (P <0.05). Carboxymethyllysine increased in the ACEi-treated group when compared with the CG, whereas intermediate values of these biomarkers were found in the CKD group (P <0.05). The ACEi-treated group showed the highest values of carboxymethyllysine, advanced oxidation protein products and hexanoyl-lysine. By contrast, the CKD group had the highest concentration of malondialdehyde. No statistically significant difference was found in the levels of pentosidine or methylglyoxal. End products correlated with creatinine and urea and with each other.
Conclusions and relevance
Significantly high concentrations of both intermediate and end products of carbonyl/oxidative stress were detected in CKD cats. This is the first study to have concurrently taken into account several uraemic toxins and biochemical parameters in cats affected by CKD.
Introduction
The term ‘chronic kidney disease’ (CKD) indicates an irreversible decrease in renal function due to structural or functional defects in one or both kidneys.1,2 Cats, especially of geriatric age, are commonly affected by CKD.3,4 In human medicine, it has been shown that oxidative stress (OS) is associated with uraemia. 5 It has been hypothesised that two main events occur in CKD: the facilitation of inflammation and OS by uraemic toxins, 6 and the impairment of antioxidant enzymes in uraemia.7,8 To our knowledge, only four studies have evaluated OS in cats diagnosed with CKD: Yu and Paetau-Robinson conducted research on OS and the effects of dietary antioxidant supplementation; 9 Keegan and Webb correlated OS parameters with neutrophil function; 10 Kroficˇ Žel al evaluated the activity of antioxidant systems; 11 and Whitehouse et al investigated the increase in urinary F2-isoprostanes in different International Renal Interest Society (IRIS) stages of CKD. 12
OS is a complex phenomenon, which includes many pathways. Although it can be measured in different ways, the assessment of the by-products of OS reactions by means of biomolecules, such as proteins, lipids and sugars, is the most common procedure. When reactive species act on lipids many peroxidation products are created, such as hydroperoxides, conjugated dienes, isoprostanes and derived carbonyls, such as malondialdehyde (MDA) and hydroxynonenal. 13 It has recently been shown that hexanoyl-lysine (HEL), another marker of fatty acid oxidation, is formed at an earlier stage of the cascade. This compound is a specific marker of omega-6 oxidation and promotes the formation of adducts from linoleic acid or arachidonic acid. 14 Proteins are other molecules sensitive to the action of reactive species. Amino acids (aa) are prone to many reactions, including hydroxylation, nitration, sulfoxidation, chlorination, cross-linking and conversion to carbonyl derivatives. 13
Of all the by-products originating from proteins damaged by OS, carbonyls, advanced oxidation protein products (AOPPs) and adducts formed between aa and free carbonyls or lipid oxidation/reducing sugar products are the most extensively studied. 13 The latter group of reactions consists of the addition of compounds deriving from glycation and lipid peroxidation to proteins: 15 these reactions are also known as carbonylation. This modification is sustained by a surplus of reactive carbonyl compounds; in this circumstance, a series of different complex reactions lead to the formation of more stable final products, called ‘advanced end products’, such as pentosidine (Pent) and carboxymethyllysine (CML). While Pent is a marker of the glycoxidative cascade and can be classified as an advanced glycation end product (AGE), CML is not only formed along this pathway, but also during the lipoxidation cascade; thus, CML can also be considered an advanced lipoxidation end product compound. 16 An increase in these reactions is referred to as carbonyl stress and is related to the pathogenesis of several diseases, including chronic renal failure. 17
From this brief summary, it is clear that OS creates a series of reactions leading to measurable by- and end products; what is known in human medicine is that reactive oxygen species (ROS) increase carbonyl stress and facilitate the formation of end products, 18 which themselves act as inducers of ROS in a vicious cycle (Figure 1). This tight relationship is present in uraemic human patients affected by CKD, who show an increase in both carbonyl and oxygen reactive species.5,7 These molecules are recognised as uraemic toxins and may play a role in the progression of chronic renal failure.

The vicious cycle of reactive carbonyl species (RCS) and reactive oxygen species (ROS) formation pathways.
Over recent years, research into uraemic toxicity has highlighted dozens of retention solutes that interact negatively with physiological mechanisms. 19 Looking at the uraemic database, 20 the only uraemic toxins studied in feline medicine are creatinine (used for IRIS staging), urea, MDA and parathyroid hormone.9,21 Understanding how these substances are formed in chronic diseases can lead to the development of new therapeutic strategies.
Currently, in cats affected by CKD, the main therapeutic goal attempts to reduce the progression of the disease. 22 To date, the available approaches are based on the administration of proper diets (with the essential nutritional characteristics established by the Commission Regulation [EU] No 1123/2014 consisting of high-quality proteins in reduced quantity and restricted levels of phosphorous). Moreover, according to other sources, this dietary regime should be supplemented with omega-3 polyunsaturated fatty acids (PUFA) and antioxidants, dehydration should be corrected and drugs (such as calcium channel blockers and inhibitors of the renin–angiotensin–aldosterone system; ie, angiotensin-converting enzyme inhibitor [ACEi] or angiotensin receptor blockers [ARB]) 23 should be introduced to improve renal function, reduce blood pressure and lower systemic OS. 22 With regard to this last clinical recommendation, we previously reported that oral antihypertensive therapy exerts antioxidant activity, which scavenges ROS in humans. 24
The aim of the present study is to confirm whether in cats affected by CKD, carbonyl stress and end-product formation are higher than in healthy cats, and to assess whether ACEi may affect these hallmarks.
Materials and methods
Selection of cases
The study was carried out between January 2013 and June 2014. Twenty-two adult cats (nine neutered males and 13 neutered females) aged 4–14 years were enrolled, with body condition score (9-point scale, according to the American Animal Hospital Association) centred on the mean value for the CKD cats. Signalment data of the cats among the three groups are illustrated in Table 1. Cat owners gave their written consent for all clinical procedures that are part of routine care and quality standard of the involved hospital and residual samples from routine visits not related to the study were employed.
Summary of signalment data and laboratory findings for selected clinical parameters in the control group (CG), chronic kidney disease (CKD) cats and angiotensin-converting enzyme inhibitor-treated (ACEi-treated) cats

Data are reported as median (interquartile range; 25–75th percentiles). Letters identify differences between group comparisons (P <0.05). Reference interval values according to the laboratory
RI = reference interval; IRIS = International Renal Interest Society; CREA = creatinine; TP = total proteins; GLU = glucose; TG = triglycerides; K = potassium; P = phosphorus; UP/UC = urine protein:creatinine ratio; SBP = systolic blood pressure
The cats were divided into three groups. Control group cats (CG; n = 6) were enrolled during annual check-up examinations; the inclusion criteria for control animals were based on their clinical history and the absence of any disease on the basis of their anamnesis, physical examination, blood and urine analyses, and the absence of medications except for parasitic control.
The other two groups consisted of samples collected from cats affected by CKD and staged according to IRIS guidelines. 23 CKD diagnosis was confirmed with anamnesis, physical examination, complete blood count and urine analyses, with specific measurements of blood creatinine and confirmation of low urine specific gravity (<1035) at two separated time points. The exclusion criteria were pre- and post-renal azotaemia, acute renal injury, acute infections, feline lower urinary tract disease, presence of active urinary sediment, systemic metabolic disease (eg, hyperthyroidism), diabetes, heart failure and positivity for feline leukaemia virus or feline immunodeficiency virus.
The CKD group (n = 11) included samples from animals where the diagnosis was just confirmed (second time point sampling) and for this reason no pharmacological treatment was initiated – only diet and routine care support according to good clinical practices.
The third group (ACEi-treated, n = 5) included cats with a stable CKD (diagnosed as described before) that were being treated with the specific diet and the ACEi benazepril (dosage regime was adapted and based on the values commonly recommended in clinical animal practice); the residual samples were obtained from cats during the follow-up period, which was performed in a timeframe decided by the clinician.
All the cats in the latter two groups were kept on a renal diet formulated and standardised by a Diplomate from the European College of Veterinary and Comparative Nutrition.
Sampling
Serum was collected and stored for 30 mins at room temperature. Subsequently, it was separated by centrifugation (2500 g for 8 mins) and two aliquots were obtained: one for the analysis of the biochemical and metabolic parameters, mainly related to the renal function; and one for the assessment of the carbonyl stress biomarkers, which constituted the target of the present study. Samples were stored at −80°C and analysed according to the procedures described in the following sections. Urine samples were collected by cystocentesis when required by the clinician or by a non-invasive method (using a urine collection kit) and analysed within 1 h by an automated analyser to obtain the urine protein:creatinine (UP/UC) ratio. Blood urea, triglycerides (TG), potassium (K), phosphorous (P), creatinine (CREA) and total proteins (TP) were evaluated by an automated analyser. Plasma glucose (Glu) was determined in blood heparinised samples centrifuged within 15 mins after sample collection.
Systolic blood pressure (SBP) measurement was taken using an indirect Doppler method (Duo Vettex; Huntleigh Diagnostics) via the radial pulse with the cat sitting or in sternal recumbency. The recorded value is the mean of five measurements.
Advanced end products
All samples were analysed in duplicate.
Pentosidine
Detection of Pent was performed using high-performance liquid chromatography (HPLC), according to Valle et al, 25 using a Waters system. Briefly, protein content, after de-lipidation with hexane and precipitation with trichloroacetic acid, was hydrolysed with 6 mol/l hydrochloric acid for 18 h at 110°C in borosilicate screw-capped tubes, dried in a Speed-Vac concentrator and then reconstituted in HPLC-grade water containing 0.01 mol/l heptafluorobutyric acid (HFBA). Subsequently, it was filtered through a 0.45 µm pore diameter Ultrafree MC (Millipore) and injected into a Xterra C18 MS column (250 × 4.6 mm; Waters) with a curvilinear gradient program of 20–40% methanol from 0–30 mins and containing water (MilliQ; Millipore); both water and methanol contained 0.01 mol/l HFBA as a counterion. The Pent peaks were monitored using a Waters 2475 fluorescent detector (excitation 335 nm and emission 385 nm). A Pent synthetic standard (prepared as described by Grandhee and Monnier) 26 was injected at the start of each run to determine Pent concentration in the sample using peak area comparison. The amount of Pent was expressed as pmol per mg of plasma protein content.
CML
Serum CML was evaluated by ELISA (EIAab), according to the manufacturer’s instructions, and as reported by Bruynsteen et al. 27 The detection range of the CML ELISA kit was 0.78–50 ng/ml; therefore, the serum samples were diluted 1:10. Absorbance was read at 450 nm using a microplate reader. The observed results were expressed as ng/ml.
AOPPs
Determination of AOPPs was based on spectrophotometric analysis according to Bruynsteen et al. 27 AOPPs concentration was measured by spectrophotometry on a microplate reader at λ 340 nm and was calibrated with a chloramine-T (CT) solution in the presence of potassium iodide; briefly, 200 µl serum (diluted 1:10 with phosphate-buffered saline [PBS]) was placed on a 96-well microtitre plate, and 20 µl acetic acid was added. In standard wells, 10 µl 1.16 mol/l potassium iodide were added to 200 µl CT solution (0–100 µmol/l) followed by 20 µl acetic acid. The absorbance of the reaction mixture was immediately read at 340 nm against a blank containing 200 µl PBS, 10 µl potassium iodide and 20 µl acetic acid. The AOPPs concentrations were expressed as µmol/l of CT equivalents.
Carbonyls from the peroxidation cascade
MDA
Serum MDA was measured by HPLC according to the method published by Nielsen et al, 28 with slight modifications. Briefly, aliquots of serum were mixed (volume/volume) with a 0.6% (w/v) aqueous solution of thiobarbituric acid (TBA). The mixture was acidified with 1/20 volume of 100% (w/v) trichloroacetic acid and heated at 100°C for 1 h. The samples were then cooled in ice and centrifuged at 13,000 g for 5 mins. Aliquots of 50 μl of the supernatant were injected into the HPLC system equipped with a Novapak C18 4 µm 3.9 × 150 mm column (Waters). The elution was isocratic. The mobile phase consisted of a mixture of a 10 mM potassium dihydrogen phosphate solution, adjusted to pH 6.8 with KOH 1 M, and methanol in a ratio of 60/40. The flow rate was 1 ml/min. Detection was performed by a spectrofluorometery (excitation at 532 and emission at 553 nm). Under our conditions, the peak of the MDA–TBA adduct was well resolved at a retention time of 4.8 mins.
MDA concentration (nmol/ml) was calculated in reference to a calibration curve of MDA sodium salt standard according to the methodology developed by Nair et al. 29 Concentration was expressed in nmol/ml.
Hexanoyl-lysine
HEL was evaluated by ELISA (JalCA), according to the manufacturer’s instructions. The detection range of the HEL ELISA kit was 2–700 nmol/l. After overnight incubation with alpha-chymotrypsin, serum samples were ultrafiltered (cut-off 10 kDa) and diluted 1:2. Absorbance was read at 450 nm. Results were expressed as nmol/mg protein.
Carbonyl from the glycoxidation cascade
Methylglyoxal
Methylglyoxal (MGO) was evaluated according to the method proposed by Wild et al, 30 with slight modifications. The method is based on the reaction between N-acetyl-L-cysteine (NAC; Sigma Aldrich) and MGO at room temperature. The reaction was performed in 100 mM sodium dihydrogen phosphate buffer (adjusted to pH 7.0 with NaOH 10 M) at 22°C. As the standard curve for the reaction, different concentrations of MGO (0.5, 1, 2 and 5 mM) were used. MGO solutions (Sigma Aldrich) equating to 0.5, 2 and 5 mM were added to a volume of 980 μl with sodium dihydrogen phosphate. The reaction was started by adding 20 μl 500 mM NAC and the absorption was recorded after 7 mins. The condensation product, N-α-acetyl-S-(1-hydroxy-2-oxo-prop-1-yl) cysteine was determined by recording the absorption at 288 nm (UVIKON 923; Bio-Tek Instruments). Results were expressed as μmol/ml.
Serum protein content determination
Serum protein content was determined using the BCA protein assay kit according to the manufacturer’s instructions (Thermo Fisher Scientific).
Statistical analysis
Data were analysed using GraphPad Prism for Mac, version 7.00.
All measurements were performed in duplicate and data expressed as medians and interquartile ranges. After checking for normality using the Kolmogorov–Smirnov test, comparisons between groups were performed using the Kruskal–Wallis test followed by Dunn’s multiple comparison tests. P values <0.05 were considered significant (a ‘tendency’ was considered for P <0.1). Relationships between plasma concentrations of the considered biomarkers and the other metabolic parameters were investigated using the one-tailed Spearman’s correlation coefficient (rS).
Results
Results are illustrated in Tables 1 and 2.
Samples from cats in the ACEi-treated groups were obtained from animals treated with benazepril for a minimum of 40 days and a maximum of 60 days.
Comparison of the groups showed a significant increase in CREA and urea in CKD and ACEi-treated groups compared with healthy (CG) cats (Table 1). No statistically significant differences were found between groups for TP, GLU, TG and K. The highest concentration of P was found in the CKD group, whereas the ACEi-treated group showed intermediate values. In both CKD and ACEi-treated groups UP/UC was higher than in the control group.
AOPPs, MDA and HEL concentrations were significantly higher in CKD and ACEi-treated groups compared with the CG group. When compared with the CG, CML was higher in the ACEi-treated group, whereas the CKD group showed intermediate values. The ACEi-treated group was characterised by the highest values of CML, AOPPs and HEL; conversely, the CKD group showed the highest concentration of MDA. The levels of Pent and MGO showed no statistical differences between groups (Table 2).
Advanced glycated end products and carbonyl compounds in the control group (CG), chronic kidney disease (CKD) cats and angiotensin-converting enzyme inhibitor-treated (ACEi-treated) cats
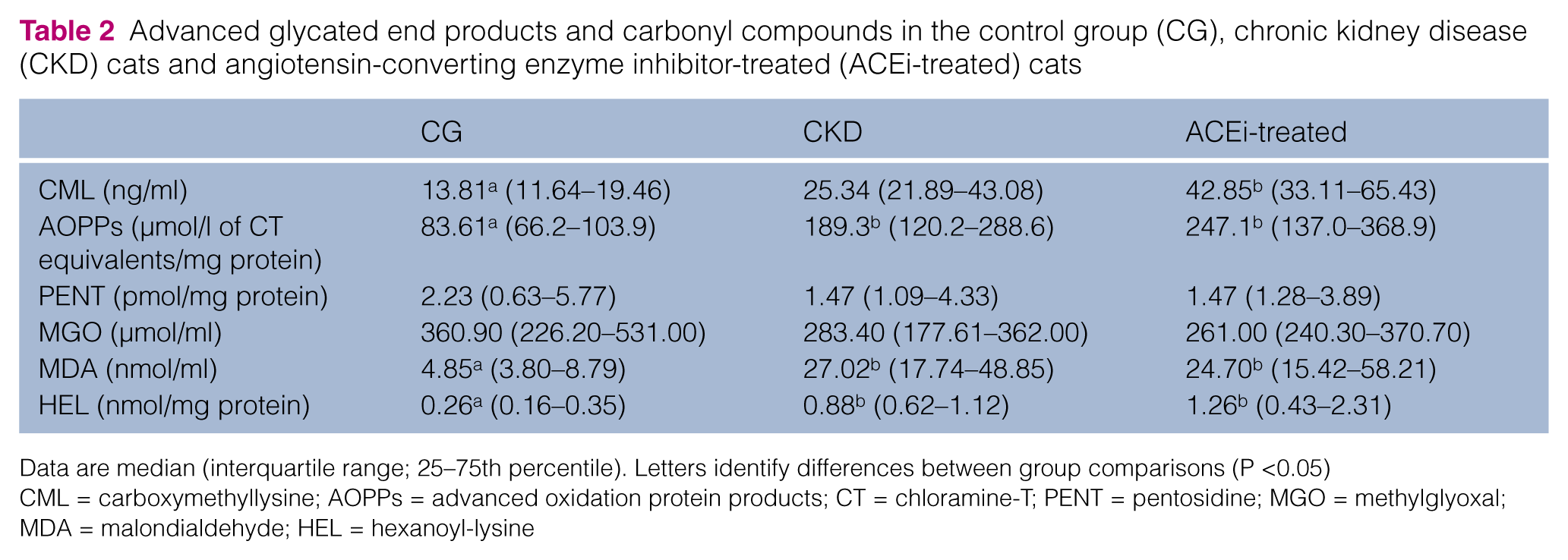
Data are median (interquartile range; 25–75th percentile). Letters identify differences between group comparisons (P <0.05)
CML = carboxymethyllysine; AOPPs = advanced oxidation protein products; CT = chloramine-T; PENT = pentosidine; MGO = methylglyoxal; MDA = malondialdehyde; HEL = hexanoyl-lysine
CREA was positively correlated with CML (rs = 0.49, P <0.05), AOPPs (rs = 0.56, P <0.05), MDA (rs = 0.47, P <0.05) and HEL (rs = 0.50, P <0.05). It was also correlated with laboratory findings for selected clinical parameters, such as urea (rs = 0.79, P <0.0001), P (rs = 0.57, P <0.05) and UP/UC (rs = 0.64, P <0.01). Urea was positively correlated with CML (rs = 0.46, P <0.05), AOPPs (rs = 0.62, P <0.01), MDA (rs = 0.72, P <0.0001) and HEL (rs = 0.56, P <0.05), as well as to K (rs = 0.52, P <0.05) and UP/UC (rs = 0.65, P <0.01).
HEL was positively correlated with CML (rs = 0.48, P <0.05), AOPPs (rs = 0.76, P <0.0001), MDA (rs = 0.90, P <0.0001) and K (rs = 0.60, P <0.01). AOPPs were positively correlated with CML (rs = 0.56, P <0.05), MDA (rs = 0.75, P <0.0001), P (rs = 0.48, P <0.05) and UP/UC (rs = 0.54, P <0.05). MDA was positively correlated with K (rs = 0.65, P <0.01) and UP/UC (rs = 0.54, P <0.01) and to CML (rs = 0.36, P = 0.05). CML was negatively correlated with GLU (rs = −0.482, P <0.05). MGO was negatively correlated with K (rs = −0.574, P <0.05). Pent was only positively correlated with SBP (rs = 0.46, P <0.05).
The correlation table is provided as supplementary material.
Discussion
The present study focuses on hallmarks of OS and carbonyl stress in feline CKD. Significantly higher concentrations of intermediates and ‘end products’ of carbonyl/OS, which are also uraemic toxins, were detected in nephropathic cats.
An increased concentration of creatinine and urea and an increase in the UP/UC ratio (indicating proteinuria associated with kidney disease, provided that pre- and post-renal causes are excluded) were observed in CKD cats and ACEi-treated cats. ACEi, like benazepril, have been shown to reduce proteinuria in cats; 31 however, in the present study, UP/UC in the ACEi-treated group was even higher than in the other group. The late initiation of the therapy (introduced 40–60 days before sample collection) can probably explain such a difference.
Over 100 substances have been classified as uraemic toxins by the European Uremic Toxin (EUTox) Work Group, 20 and recent studies have thoroughly categorised these different molecules. Urea and creatinine are the most common uraemic toxins that can increase in cats with CKD and, as expected, in our study both increased in the cats with CKD. These compounds are soluble in water, have low molecular weights and are classified by EUTox as the most reliable biomarkers for the evaluation of renal failure. 32 Not surprisingly, in our study, urea and CREA showed a positive correlation with each other, as well as with UP/UC. In fact, an increase in these parameters typically occurs in CKD cats, and it is used as a diagnostic tool according to the IRIS staging of CKD. 23
However, several other metabolites, other than these compounds, contribute to the toxic environment caused by the disease. 32 Their concentrations provide insight into the clinical severity of CKD and favour the maintenance of both oxidative and carbonyl stress in a vicious circle.
In addition, CREA and urea positively correlated with CML, AOPPs, MDA and HEL, confirming an association with two recognised markers of renal failure in feline medicine. In particular, a statistically significant increase of CML, AOPPs, HEL and MDA was found in the cats affected by CKD. By contrast, they showed a negligible increase in Pent and MGO. These differences were also consistently observed in the ACEi-treated group.
AOPPs are a cluster of oxidative products derived from proteins and are recognised as markers of protein oxidative damage and of inflammation severity. The injured proteins are generated through a mechanism involving free radical direct oxidation of aa (eg, tyrosine, lysine, proline, arginine, etc), 33 and as an indirect consequence of lipoperoxidation.
AOPPs are also defined as ‘accumulated solutes, normally excreted by the kidneys, that interact negatively with biological functions’. 15
It has been reported that serum AOPPs concentration (closely correlated with other markers) increases with the progression of chronic diseases.34,35 Accumulation of plasma and renal AOPPs is a common pathological finding in humans with CKD. 36 Witko-Sarsat et al showed that in vivo levels of AOPPs correlated well with creatinine clearance.34,35
In human studies of uraemic patients, the concentration of plasma AOPPs is related to the oxidative activity of circulating neutrophils, suggesting that these leukocytes might be involved in plasma AOPPs formation through the myeloperoxidase/H2O2 system. In agreement with this hypothesis, Keegan and Webb reported that the neutrophil oxidative burst is higher in chronic renal failure. 10 Moreover, recent studies showed alterations in neutrophil oxidative metabolism and OS in dogs with CKD.37–41
Neutrophils can therefore be a source of pro-oxidant molecules contributing to an abnormal production of ROS and participating in the formation of AOPPs. Neutrophil oxidative metabolism can, in turn, be activated by other uraemic toxins. 41
In accordance with the abovementioned findings, our study demonstrates for the first time a significant increase in AOPPs in cats. In fact, when compared with control animals, CKD and ACEi-treated cats showed a 77% and 132% increase, respectively, in this parameter. AOPPs are good hallmarks of the progression of chronic renal failure and the severity of uraemia; 42 accordingly, in our study, their concentrations correlated well with those of creatinine and urea. As previously reported, they are also a good and accurate biomarker of OS, 43 and in the present study significant correlations with other markers of lipoperoxidation were found (CML, MDA, HEL).
Serum MDA is an organic and very simple compound and one of the highly reactive carbonyls originating from PUFA oxidation (in particular from peroxidation of arachidonic, eicosapentaenoic and docosahexaenoic acid). 44 In humans, it is the most abundant product, as it comprises 70% of all the carbonyls obtained by lipid peroxidation. 18
In this study, serum MDA consistently increased in CKD (284%) and in ACEi-treated (256%) cats. An increase in serum MDA was previously observed in CKD cats by Yu and Paetau-Robinson, 9 and 4 weeks of antioxidant supplements did not exert any effect on this parameter.
MDA correlates with AOPPs, HEL and with other markers of CKD (creatinine, urea, potassium and UP/UC): the remarkably high correlation with HEL (r = +0.904) is explained by their shared origin from lipid peroxidation.
As potassium did not vary significantly between groups, but it often varies in CKD cats according to diet intake, 45 the positive correlation with MDA is probably suggestive of an increased OS in cats with higher potassium quartiles, although still in the normal range.
HEL is a recently discovered lipid peroxidation biomarker derived from the oxidation of omega-6 unsaturated fatty acids. 14 HEL is formed when a lipid hydroperoxide links to a lysine residue, forming a stable compound. 46 Arachidonic acid is one of the PUFAs that, after oxidation, gives rise to MDA and HEL compounds; 44 it needs to be present in cat food, especially during growth, gestation and lactation, because cats are unable to synthesise it. 47 The actual estimated requirements, based on a low reported synthesis capacity, is 8 mg/100 g dry matter (DM), considering a metabolic energy requirement of 75 kcal/kg0,67 in adult animals and 20 mg/100 g DM during growth and reproduction. 48 Arachidonic acid is naturally present in animal tissues, so it does not have to be added to food containing proteins of animal sources. 47
When compared with control cats, CKD and ACEi-treated cats showed highly significant increases in serum HEL (three times higher than controls in the CKD group and five times higher than controls in ACEi-treated cats). Therefore, it would be interesting to evaluate whether a high content of arachidonic acid in the diet of CKD cats might generate oxidants and promote OS, as observed in CKD disease; if that were the case, more attention should be paid to the total amount of this substance provided to cats, in particular to those affected by CKD. The diet should be balanced with an equivalent amount of antioxidants to avoid the increase of carbonyls, such as MDA and HEL, originating from the peroxidation cascade.
CML is formed during the Maillard reaction by a process of glycoxidation. It can derive from different compounds, such as aldoses, ketoses, ascorbate, PUFAs and other molecules, and it is classified as an AGE. Another relevant source of CML is from food. It is found not only in dairy products, but also in meat, fish, cereal-derived products, and in a group of fruit and vegetables that have been cooked or treated in an industrial context. 16
As previously shown, 49 CML increases in uraemic patients and such an increase is also generally paralleled by increased levels of Pent, 49 as they share the same molecular origin. In the present study, CML levels increased three-fold in the ACEi-treated group and doubled in the CKD group, but, intriguingly, a correlation with Pent was not observed.
We might hypothesise that although CML mainly derives from the peroxidation cascade, diet may also play a noteworthy role. Hull et al showed that the CML content of cat food can be high. 50 High exposure to CML should be taken into careful consideration because this compound could be hazardous for feline health. This is even more true in cats with CKD, as CML seems to be associated with degenerative disorders and CKD. 51
Interestingly, CML levels are positively correlated with markers of kidney function, such as CREA and urea, and negatively correlated with serum glucose, indicating that, in cats, high glucose might not lead to the formation of AGEs through the Maillard reaction. Other significant correlations were found with HEL (P <0.05) and AOPPs (P <0.05), which can therefore be included, as is the case for humans, in the array of toxins found in uraemic cats.
Methylglyoxal is generated by a series of metabolic pathways, mostly belonging to the glycolytic process. It is an important precursor of AGEs, being a highly powerful glycating agent. It is also involved in diabetic microvascular complications. 52 Increases in MGO have been observed during hyperglycaemia, as well as in the uraemic state.
In our study, MGO was not significantly different between the three groups of cats. Therefore, we can hypothesise that, in contrast to what has been observed in humans, the glycation pathway does not play a role in the pathophysiology of uraemia in cats.
Pent is a well-known advanced glycation end product and a uraemic toxin. Surprisingly, the levels of Pent were not significantly different in the three groups of our study. This finding differs from what has been reported in human patients affected by CKD. In these cases, a marked increase of Pent was found and also associated with a low glomerular filtration rate, OS and inflammation.53–55 In our opinion, in feline CKD, lipids and lipoperoxidation seem to play a more important role than glucose, glycation or glycoxidation, which appears to be unrelated to this disease. In cats, a distinct pathway for the formation and accumulation of uraemic toxins should be considered, along with different uraemic OS compounds. In line with this reasoning, Pent might turn out to be a minor end product in the bulk of AGEs.
In addition, in our groups of cats, Pent does not correlate with other carbonyl determinations and other clinical parameters, although it does with SBP. We can hypothesise that, in cats, Pent accumulation is, as in humans, age related, connected with the progression of renal failure, and occurring mainly in tissues rather than in blood. Tissue accumulation of Pent is well described in humans and in other animals such as rats with CKD (where it accumulates in the tubules), 56 dogs, rabbits, monkeys, and so on. Moreover, in cats with CKD, an interstitial fibrosis has been observed. 57 Pent accumulation may occur in the kidneys or in the artery walls, contributing to an increase in blood pressure. It is noteworthy that, in humans, serum Pent is positively associated with arterial stiffness and thickness. 58 Further studies are needed to evaluate this intriguing hypothesis.
According to our results, the use of an ACEi exerted a negligible effect on the carbonyl OS status. By contrast, Monacelli et al 24 reported, in humans, that valsartan, an angiotensin II receptor antagonist, besides having antihypertensive activity, is also effective in scavenging OS species.
However, some differences between the present study and that of Monacelli et al 23 should be considered. Our experimental animals only received the therapy for 40–60 days, whereas the trial reported by Monacelli et al lasted 6 months. 23 The difference in the duration of the treatment may explain the lack of efficacy reported in our study. Unfortunately, as we used residual samples to perform this study, the timeframe between the start of the therapy and the sampling was the one decided by the clinician to re-examine the cats, which in our cases resulted in a range of approximately 40–60 days and was probably not sufficient to exert an effect on the evaluated parameters.
Such a difference could also be due to the use of a different type of drug. In fact, in our experiment, cats were treated with benazepril, an ACEi, whereas in the study carried out by Monacelli et al, 23 human patients received valsartan, an angiotensin 1 antagonist.
Although carefully designed, our study suffers from some limitations, mainly owing to its small sample size. In particular, it would have been more appropriate to enrol a larger number of cats for each IRIS stage (from 1–4) in order to draw more valid conclusions. The progression of uraemic toxin production and/or the existence of a CKD threshold for their formation is also a matter of debate and deserves further investigation. Even if we had just included cats fed a renal diet, we would still have had confounding effects. In fact, renal diets of different brands can also vary in terms of omega 3–6, protein, P and carbonyl content. Further studies focusing on the intake of single diet components are required.
Conclusions
To the best of our knowledge, this is the first study to take into account several contemporaneous uraemic toxins – according to the EUTox database – and biochemical parameters in cats with CKD. Evidence of strong carbonyl stress is confirmed in CKD cats, irrespective of the therapy with an ACEi. These toxic molecules contribute to maintaining and promoting OS and facilitate the progression of systemic damage. However, two markers – Pent and methylglioxal – remained unaffected. This phenomenon suggests some hypotheses that need to be verified and, at the same time, raises the possibility that the disease might be characterised by a new pattern of markers. The significant and striking increases in CML and HEL offer challenging possibilities in terms of specific diets aimed at the prevention of kidney disease. Currently, more studies are needed to clarify the disease mechanisms and their associations with clinical signs, cellular damages and kidney malfunction in affected cats.
The results of the present study broaden our understanding of this widespread problem afflicting feline health and help pave the way towards new research fields required to make substantial progress in clinical veterinary practice.
Supplemental Material
Supplementary Material
Correlation between the clinical/biochemical, oxidative and carbonyl parameters considered in this study
Footnotes
Acknowledgements
We thank Dr Bruno Tasso (DIFAR, University of Genova, Italy) for the synthesis of malondialdehyde sodium salt and Dr Marco Maimone (Clinica Veterinaria Foce) for his help in the recruitment of the animals.
Author note
Part of the data were presented at the 2015 European Society of Veterinary & Comparative Nutrition conference.
Supplementary material
Correlation between the clinical/biochemical, oxidative and carbonyl parameters considered in the study.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was partially supported by Candioli Farmaceutici SPA.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.