
Abstract
Objectives
Although a clear relationship has been demonstrated between the presence of lumbosacral transitional vertebrae and the development of lumbosacral stenosis in dogs, this relationship has not been evaluated in cats. The aim of this study was to investigate the relationship between the presence of lumbosacral transitional vertebrae and lumbosacral stenosis in cats.
Methods
The medical records and diagnostic imaging studies of 13 cats diagnosed with lumbosacral stenosis were retrospectively reviewed for lumbosacral abnormalities and compared with findings of 405 cats that underwent CT for reasons unrelated to spinal disease.
Results
Clinical signs associated with lumbosacral stenosis included lumbosacral pain, low tail carriage, difficulty jumping, and urinary or faecal incontinence. Neurological signs included proprioceptive deficits, ambulatory paraparesis, pelvic limb ataxia, reduced spinal reflexes and reduced perianal reflex. Duration of clinical signs ranged from 1 day to 10 months (mean 3 months). Of the 13 cats with lumbosacral stenosis, seven (53.8%) were diagnosed with lumbosacral transitional vertebrae. In the control population of 405 cats, 24 (5.9%) were diagnosed with lumbosacral transitional vertebrae. Results indicated that lumbosacral transitional vertebrae were significantly (P <0.0001) more prevalent in cats with lumbosacral stenosis compared with the control feline population (odds ratio 18.52, 95% confidence interval 6.1–62.1). Development of clinical signs of lumbosacral stenosis in cats with lumbosacral transitional vertebrae (mean 10.8 years) was not significantly different from that of cats without lumbosacral transitional vertebrae (mean 12.7 years). Likewise, there was no significant influence of breed (P >0.99) or sex (P = 0.29) on the occurrence of lumbosacral transitional vertebrae.
Conclusions and relevance
Despite lumbosacral stenosis being a rare spinal condition in cats, lumbosacral transitional vertebrae can be considered a risk factor for its development.
Introduction
Degenerative spinal disease, including degenerative intervertebral disc disease and lumbosacral stenosis, is considered rare in cats.1,2 The most common feline spinal cord conditions include lymphoma, feline infectious peritonitis, myelitis and vertebral neoplasia.2,3
Lumbosacral stenosis is defined as a narrowing of the vertebral canal at the level of the lumbosacral junction (L7–S1), which can result in compression of the cauda equina. 4 Clinical signs associated with this condition include lumbosacral pain, pelvic limb lameness, abnormal tail carriage, reluctance to jump, and urinary and faecal incontinence.5–10
Degenerative lumbosacral stenosis (DLSS) is a multifactorial condition, 8 which is commonly seen in large-breed dogs.8–11 It is predominantly caused by Hansen type-II intervertebral disc disease. 8 Other abnormalities include osteophyte formation causing narrowing of the intervertebral foramina, hypertrophy of the interarcuate ligament and joint capsule, and epidural fibrosis.8,10,12 These changes result in a progressive narrowing of the vertebral canal and/or intervertebral foramina, thus producing clinical signs associated with cauda equina compression. 10
A lumbosacral transitional vertebra (LTV) is an abnormal vertebral segment, possessing both lumbar and sacral morphological characteristics.13,14 They are congenital spinal anomalies, located between the last normal lumbar vertebra and the first normal sacral vertebra.14–16
A previous study revealed LTV were the most common spinal anomaly in cats; however, no clinical signs were associated with them. 17 In dogs, LTV have been reported to be a risk factor for the development of DLSS, potentially by altering the biomechanics of the lumbosacral junction and thus accelerating degenerative changes.10,13,14,18 Studies have also shown a link between asymmetrical LTV and hip dysplasia in dogs.14,15,19 In cats, a similar trend has been identified but not statistically proven. 16 Therefore, it remains unclear if LTV also contribute to the development of DLSS in cats. The aim of this study was to investigate the relationship between LTV and DLSS in cats. It was hypothesised that the prevalence of LTV would be greater in cats with DLSS than in cats without DLSS.
Materials and methods
Case selection
The digital medical database of the Small Animal Referral Hospital, Royal Veterinary College, University of London was searched to identify cats with a diagnosis of DLSS between July 2007 and February 2016. Search terms used were lumbosacral stenosis, lumbosacral syndrome, lumbosacral disease, cauda equina, dorsal laminectomy and L7–S1. Cats were included if they had clinical signs and MRI findings compatible with a diagnosis of DLSS. Cats were excluded if the medical records and imaging studies were incomplete or unavailable for review. Information acquired from the medical records included signalment, duration and nature of clinical signs. MRI was performed under general anaesthesia with a high-field unit (1.5 T, Intera; Philips Medical Systems) and imaging studies included a minimum of T1- and T2-weighted sagittal and transverse images.
In order to evaluate the prevalence of LTV among the overall feline hospital population, all cats that had undergone CT imaging procedures, which included the thoracolumbar, lumbar and lumbosacral vertebral segments, within the same time period as the cats with DLSS (between July 2007 and February 2016) were reviewed. The signalment of each cat and the reasons for the CT procedures were recorded from the medical records. Animals with spinal disease or trauma were excluded from this group of cats. CT was performed with a 16-slice helical CT scanner (PQ 500, Universal Systems, Solon; GE Healthcare), under sedation or general anaesthesia. Sagittal, dorsal and three-dimensional (3D) volume-rendering images were constructed after completion of the transverse images.
Imaging review
For the control group, CT scans were reviewed by a final-year veterinary student following training by a board-certified neurologist, with references to normal lumbosacral anatomy available (Figure 1). The presence of an LTV was diagnosed based on the presence of transverse processes on the first sacral vertebra, an intervertebral disc space present between the transitional vertebra and the caudal contiguous sacral vertebra, or increased distance between the base of the S1 and S2 sacral spinous processes as seen on CT sagittal, dorsal and 3D volume-rendering reconstructions (Figures 2 and 3). The bone window was used for this evaluation and potential cases of LTV were also evaluated by a board-certified neurologist before a final diagnosis of LTV was made. To count the number of lumbar vertebrae, the last thoracic vertebra was used as a reference point. Any other lumbosacral abnormalities were also recorded.

Normal feline lumbosacral anatomy shown via (a) skeletal model dorsoventral view, (b) skeletal model lateral view, (c) CT three-dimensional volume rendering and (d) CT sagittal reconstruction
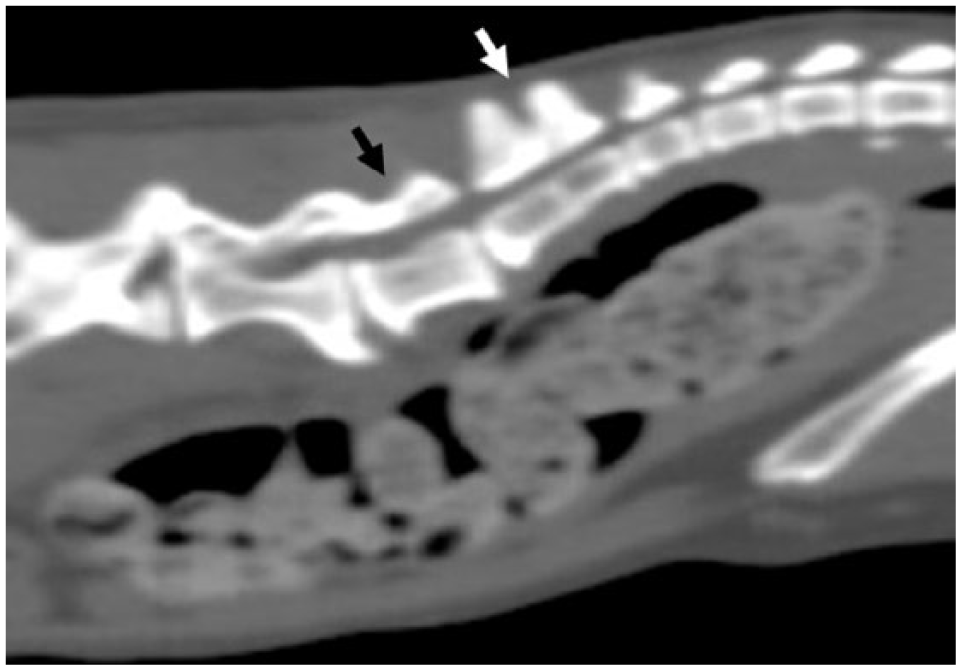
Sagittal reconstruction of the lumbosacral vertebral column of a cat with a lumbosacral transitional vertebra. The black arrow points to the eighth lumbar vertebrae. The white arrow shows only two dorsal spinous processes of the sacrum

Dorsal view of a three-dimensional reconstruction of feline pelvis and lumbosacral vertebral column. S1 possesses several features of a lumbar vertebrae, including transverse processes and an intervertebral disc space. This can be seen in both (a) and (b). Increased distance between the dorsal spinous processes of S1 and S2 can be seen indicated by the black arrows in (a) and (b)
LTV were classified based on a number of criteria: the number of lumbar and sacral vertebrae present, the presence of transverse processes on S1 and whether the transitional vertebra possessed more lumbar or sacral morphological characteristics.
MRI, orthogonal radiographs and CT studies of cats affected by DLSS were analysed by a board-certified neurologist and the same criteria were used to define the occurrence of an LTV.
Statistical analysis
Data analysis was performed using a statistical software package (Prism, version 7.0b for Mac OS X; GraphPad Software). Fisher’s exact test was used to compare the prevalence of LTV within the general feline population, and within the group of cats affected by DLSS. This test was also used to compare the influence of sex, purebred status and type of breed (for breeds represented by more than five cats in the control population) on the presence of LTV. A Mann–Whitney U-test was used to evaluate the relationship between LTV and age at diagnosis of DLSS. P values <0.05 were considered significant and confidence intervals (CI) were set at 95%.
Results
A total of 418 cats were included in this study, of which 13 had DLSS and 405 underwent CT for reasons unrelated to spinal disease.
Control group
In total, 405 cats had CT imaging performed between July 2007 and February 2016. The group comprised 233 males and 172 females. Three hundred and fifty-one of the 405 cats were neutered, of which 202 were male and 149 were female. Breeds represented were domestic shorthair (n = 260), domestic longhair (n = 31), British Shorthair (n = 27), Bengal (n = 12), Siamese (n = 10), Maine Coon (n = 8), Persian (n = 8), Birman (n = 6), Burmese (n = 6), domestic semi-longhair (n = 5), Tonkinese (n = 4), Exotic Shorthair (n = 3); three breeds were represented by two cats each, nine breeds were represented by one cat each and 10 cats were crossbreeds. Age ranged from 13 days to 19 years and 7 months (mean 9.5 years, median 10 years).
Reasons for CT scans included neoplasia screening (n = 172), respiratory disease (n = 57), neurological disease excluding spinal disease (n = 29), endocrine disease (n = 25), weight loss and inappetence (n = 24), haematological abnormalities (n = 24), ophthalmic disease (n = 14), gastrointestinal disease (n = 14), urogenital disease (n = 11), abdominal effusions (n = 8), pyrexia (n = 7), cardiovascular disease (n = 7), orthopaedic disease (n = 6), skin disorders (n = 5) and hepatic disease (n = 2).
Cats affected by DLSS
In total, 13 cats were diagnosed with DLSS, of which eight were male and five were female. All cats were neutered. Breeds represented were domestic shorthair (n = 8), domestic longhair (n = 1), domestic mediumhair (n = 1), Siamese (n = 1) and British Shorthair (n = 1). Age ranged from 2 years and 8 months to 16 years and 10 months (mean 11.7 years, median 11.5 years).
The duration of clinical signs ranged from 1 day to 10 months (mean 3 months). Clinical signs included lumbosacral pain on palpation (n = 12), low tail carriage (n = 4), difficulty jumping (n = 4), urinary incontinence (n = 1) and faecal incontinence (n = 1). Neurological deficits were present in 92% (n = 12) of the cats with DLSS, including proprioceptive deficits (n = 10), ambulatory paraparesis (n = 9), pelvic limb ataxia (n = 5), reduced muscle tone (n = 4), plantigrade stance (n = 4), reduced spinal reflexes (n = 4) and reduced perianal reflex (n = 1).
In total, 46% (n = 6) underwent MRI for DLSS diagnosis, 38% (n = 5) had both MRI and radiographs performed, and 15% (n = 2) underwent MRI and CT imaging. Diagnostic findings confirming DLSS included intervertebral disc protrusion (n = 9), narrowing of the intervertebral disc space (n = 6), spondylosis deformans (n = 6) and vertebral endplate sclerosis (n = 4).
Comparison of LTV in DLSS cats and the control population
The prevalence of LTV in the control population was 5.9% (n = 24), whereas the prevalence among the cats with DLSS was 53.8% (n = 7). The DLSS cats had a significantly (P <0.0001) greater prevalence of LTV compared with the control group (odds ratio [OR] 18.52, 95% CI 6.1–62.08). Cats affected by DLSS and an LTV had a mean age at diagnosis of 10.8 years (median 9.3 years), whereas cats with DLSS without LTV had a mean age of 12.7 years (median 12.5 years). This difference was not significantly different (P = 0.5064). There was also no significant influence of sex (P = 0.5921), purebred status (P >0.9999) or type of breed on the presence of LTV in cats with DLSS. For the population of 405 control cats, no significant influence of sex (P = 0.2878) or purebred status (P >0.9999) on the presence of LTV was found. No specific breeds were over-represented (P >0.05 for all breed represented by more than five cats).
LTV analysis
A total of 31 cats involved in this study were found to have LTV present. There were 24 LTV identified in the control population of cats, and seven were found in cats diagnosed with DLSS.
For the 24 cats with LTV detected within the control population 29.2% (n = 7) had eight lumbar vertebrae, 50.0% (n = 12) had seven lumbar vertebrae and 20.8% (n = 5) possessed only six lumbar vertebrae. Eighteen cats had only two sacral spinous processes, and the other six cases had all three spinous processes. Asymmetrical transverse processes of S1 were present in 50% (n = 12). In the control population spondylosis deformans was identified in three cats with LTV and 25 cats without LTV. The presence of LTV had no significant influence on the presence of spondylosis (P = 0.2252). LTV possessed mostly sacral characteristics in 54.2% (n = 13), whereas 45.8% (n = 11) had mostly lumbar characteristics of the LTV.
Of the seven cats with DLSS and LTV, 57.1% (n = 4) LTV had mostly lumbar characteristics and 42.9% (n = 3) had mostly sacral characteristics. One cat had only six lumbar vertebrae, four cats had eight lumbar vertebrae and two possessed seven lumbar vertebrae.
Discussion
This study compared the prevalence of LTV in cats diagnosed with DLSS to a control population. To the best of our knowledge, no other studies have been conducted to investigate the relationship between LTV and DLSS in cats.
In dogs it has been previously reported that LTV can be considered a risk factor for the development of DLSS. 14 The prevalence of LTV was significantly higher in cats with DLSS compared with cats that underwent CT for reasons unrelated to spinal disease. The presence of an LTV can therefore potentially be considered a contributing risk factor for the development of DLSS in cats. It has been demonstrated in dogs that animals with an LTV develop clinical signs of DLSS at a significantly younger age than animals with DLSS without a concurrent LTV. 13 Although the average age of diagnosis of DLSS in cats with LTV was 10.8 years vs 12.7 years in cats without LTV, this difference did not reach statistical significance. It can, however, not be excluded that this represents a type II error and that a significant difference would have been demonstrated if a larger number of cats with DLSS could have been included.
German Shepherd dogs have been shown to have an increased risk of DLSS and LTV;8,9 however, no specific breed predispositions could be identified in cats in this study or in previous studies.13,14,16 The differences in effect of breed regarding canine and feline populations may be primarily due to the anatomical variation between the two species. In the dog, the three sacral spinous processes are partially fused, forming the median sacral crest; however, they remain separate and evenly spaced in the cat. 17 Furthermore, the spinal cord in dogs typically terminates at L6–L7; however, in cats it extends further caudally and terminates at S1–S3. 20 The body conformation of cats in general varies much less with breed in comparison to dogs. 17
In a previous study evaluating congenital abnormalities of the feline vertebral column, transitional vertebra were found to be the most common abnormality with an LTV reported to be present in 1% of the population, 17 which is lower than reported in the study presented herein. Although other reasons cannot be excluded, one potential reason for this difference could be the use of CT instead of survey radiographs in the present study. In a previous study of dogs, 3.5% of the general canine population had LTV. 14 This prevalence is similar to the results of this study. The same canine study also revealed that 16.3% of dogs with cauda equina syndrome had LTV, with an OR of 8.4 (95% CI 3.7–18.9). 14 These figures are lower than the results of this study, with 53.9% of cats affected by DLSS having LTV and an OR of 18.52. Although the results of this study should be interpreted in light of its limitations, this finding may indicate a difference in pathology of DLSS between species and could suggest that the role of LTV in the development of DLSS may be more important in cats than in dogs.4,8,9,11
Despite more male cats being included in this study, no significant association between the presence of LTV and sex was identified (P = 0.2878). This finding is in agreement with previous research in dogs.13,14
Of the control cats with LTV 29.2% had eight lumbar vertebrae present. The relevance and nature of eight lumbar vertebrae in dogs has been a matter of debate. One study in canines argued that, clinically, the presence of L8 was irrelevant and therefore was not considered as an LTV. 13 Conversely, a more recent study in German Shepherd dogs found that in all dogs with eight lumbar vertebrae, L8 was short in length and more caudally positioned when compared with normal lumbosacral anatomy; therefore, L8 was classified as an LTV. 21 In the study presented here L8 was also considered an LTV, which could be another reason for the higher prevalence of LTV vs previously published data in cats. 16 In the control population of cats with LVT 20.8% (n = 5) had only six lumbar vertebrae present. It is possible that this reduction in the number of lumbar vertebrae is associated with the presence of a thoracolumbar transitional vertebra; however, this was not evaluated in this study.
In the control population with LTV present, 50% had asymmetrical transverse processes identified on S1. This is identical to the prevalence of asymmetrical LTV found in cats in a study that investigated the association between LTV and hip dysplasia. 16 The same study identified a trend between the presence of spondylosis deformans and asymmetrical LTV in cats; however, no statistical significance was established. 16 The study presented here did not find an association between the presence of spondylosis deformans and LTV in the control population. Spondylosis deformans is a characteristic finding associated with DLSS; 8 therefore, it was not evaluated in relation to LTV in the cats affected by DLSS.
This study is limited by several factors. Cats with DLSS underwent MRI, whereas control cats underwent CT to evaluate the presence of LTV. For this reason, observers were not blinded to clinical status of individual cats and it can therefore not be excluded that this has influenced the results of this study. Although MRI was considered the diagnostic method of choice to evaluate cats with suspected lumbosacral disease and CT was considered the diagnostic method of choice to evaluate the control population of cats, little is known about the reliability and inter-method agreement of both imaging techniques to evaluate the presence of LTV. Evaluating for the presence and characteristics of LTV is traditionally undertaken by survey radiographs.13,20,22 Although a good agreement has been demonstrated between CT and MRI for the assessment of DLSS in dogs, 22 these two advanced imaging techniques have not yet been compared for the specific purpose of evaluating the presence and anatomical characteristics of LTV. 20 Although the control cats underwent CT for reasons unrelated to spinal disease, the majority of them did not undergo a neurological examination. It can therefore not be excluded that some of them might have demonstrated subtle gait abnormalities. It can also not be excluded that some cats of the control population would have developed clinical signs of DLSS later in life.
Another consideration is the anatomical characterisation of LTV based on information from canine lumbosacral anatomy, 16 and the need to adapt this information to take into account feline anatomical differences. One example of such an interspecies anatomical difference is the normal separation of the sacral spinal processes. 17 A study in German Shepherd dogs found the prevalence of LTV in the breed was 40%, a significantly higher result compared with previous studies in the same breed.13,21 However, it was suggested that the increased prevalence could be a result of including the separation of the spinous process on S1 from the median crest as an LTV, something not undertaken in previous studies. 21 This highlights the difficulties in comparing classification methods for LTV between different species, as this separation of sacral spinous processes is a normal finding in the cat. 17
The sample size of cats with DLSS was much smaller than the control group. Although this illustrates the rare nature of DLSS in cats, this had a restrictive influence on the validity of the results and may not have been fully representative of the general population of cats with lumbosacral disease.
Conclusions
The results of this study suggest that LTV should be considered as a contributing risk factor for the development of DLSS in cats. Despite the limitations of this study, a significantly greater prevalence of LTV was identified in cats with DLSS compared with the control population.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.