
Abstract
Practical relevance:
Hepatic lipidosis (HL) is the most common form of liver dysfunction in cats. If recognized early and treated appropriately, the prognosis is good; if not, the prognosis is grave.
Clinical challenges:
Distinguishing HL as idiopathic or secondary is critical since the presence of a concurrent disease affects the therapeutic plan and the prognosis.
Audience:
Despite the unique and severe nature of a cat’s response to anorexia and the complexity of the metabolic changes underlying this condition, the clinical acumen and technical ability to effectively diagnose and treat HL are readily available to all small animal practitioners.
Patient group:
Although many species develop a ‘fatty liver’, the cat is one of relatively few species that suffer from HL. The classic presentation is that of an overweight cat that stops eating for days to weeks, losing weight in the process.
Equipment:
Abdominal ultrasound is frequently employed in the diagnostic work-up of an anorectic cat; ultrasonographic findings often support a presumptive diagnosis, provide samples for cytology and, perhaps most importantly, help identify concurrent conditions that must be addressed for therapeutic success. All of the equipment necessary for essential nutritional intervention in an anorectic cat is readily available and easily affordable.
Evidence base:
The material for this review draws heavily on a relatively large number of original studies, excellent reviews by recognized experts, and informative communication with experienced clinicians, hence the term ‘collective effort’.
It has long been known that the feline liver is home to a significant number of metabolic specializations, constraints and requirements. 1 , 2 Although many studies have focused on protein metabolism, the characteristics of lipid metabolism in cats have also been extensively investigated.3,4 The first description of feline hepatic lipidosis (HL) was published in 1977. 5 In 1984, Tams referred to a cat that had been anorectic for 9 days and showed fatty changes, vacuolated cells and mononuclear infiltration on liver biopsy. Supportive care, including ‘high caloric intake’, was used to successfully treat this particular patient. 6 It was at about this time that HL was recognized as one of the most common liver abnormalities seen in the feline veterinary population. 7 Shortly thereafter, in 1986, Center and colleagues at Cornell identified the pattern of liver enzyme elevations that appears to be pathognomonic for feline HL. 8 That same year, a case report described the presence of both renal tubular acidosis and HL in a chronically anorectic cat, one that did not respond to treatment, thereby highlighting the important role that concurrent disease plays in prognosis and treatment failure in cats that have developed HL. 9
Presentation
Feline HL may occur spontaneously and therefore is categorized as idiopathic, or it may occur as a sequela of anorexia caused by an identifiable disease or condition and is therefore categorized as secondary. There does not appear to be a gender or breed predilection and age at presentation is variable, with most cases occurring in middle-aged cats. Most cats with HL are overweight prior to the weight loss seen in many of these cases.10–13
Anorexia and weight loss are hallmarks of the history of cats with HL. When obese cats were forced to lose weight by a 50% reduction in caloric intake, the weight loss occurred without the development of HL. 14 When otherwise healthy but obese laboratory cats had their diets switched and stopped eating, they lost 30–40% of their body weight over 6–7 weeks and developed HL. 15 The duration of anorexia and the degree of weight loss are variable, but can range from several days to several weeks, with a decrease in weight of 25% or more. Vomiting, lethargy and weakness are the next most common presenting complaints, with diarrhea or constipation occurring less frequently. Ptyalism is rarely present and may be a manifestation of hepatic encephalopathy, nausea secondary to a systemic disease, or the result of an ulcerated or necrotic oral lesion.10–13,16

Cats with HL frequently present as jaundiced and dehydrated (Figure 1). Abdominal palpation may reveal hepatomegaly. A variety of other abnormalities may be found on physical examination in those HL cats with concurrent disease, and it is especially important to look for causes of pseudoanorexia (eg, oral disease, tongue lesions, significant dental disease).10,12,13,16

Icteric sclera (a), mucous membranes (b) and pinna (c) in a 7-year-old female neutered domestic shorthair cat presenting with a 2 week history of anorexia and lethargy
It is estimated that 50–95% of cats presenting with HL will have a relevant and significant concurrent condition (see Table 1).10–13
Concurrent diseases found in cats with hepatic lipidosis, in order of approximate prevalence
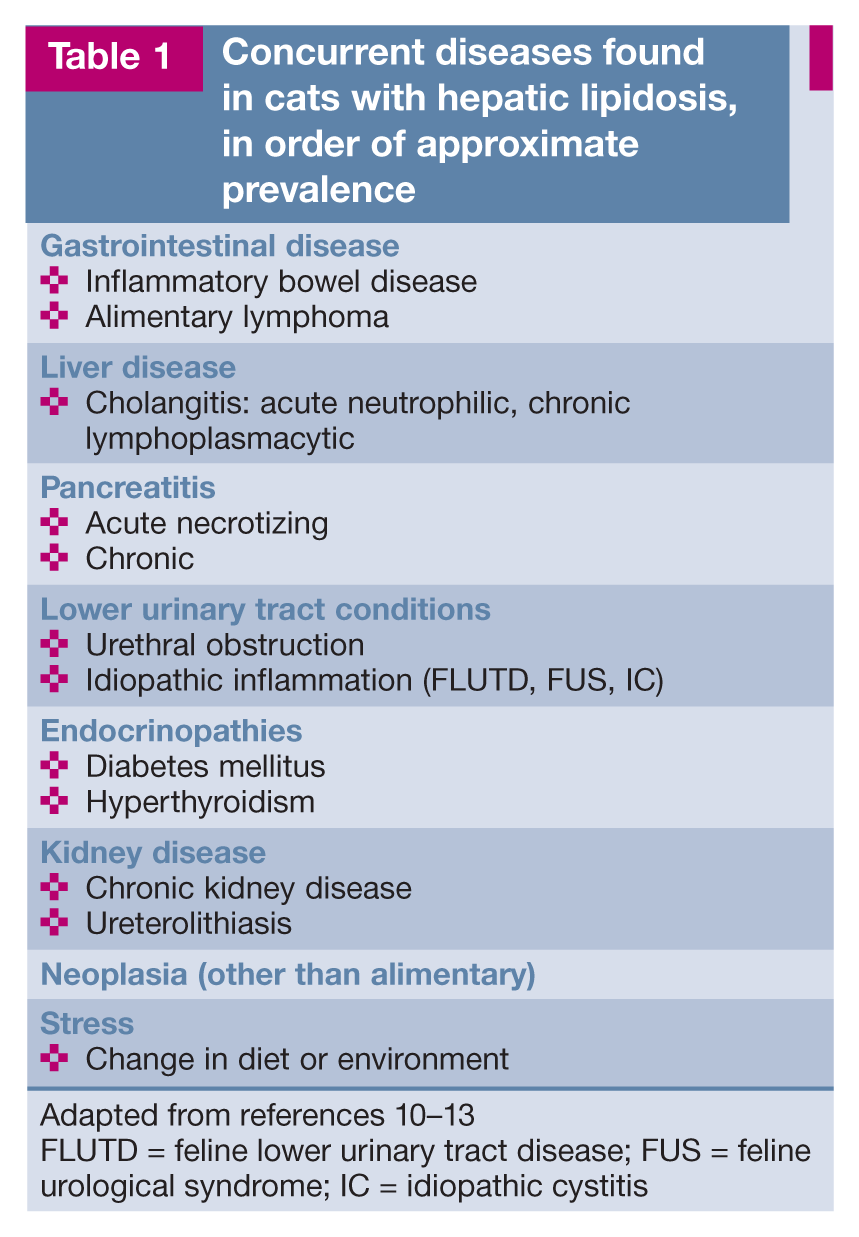
FLUTD = feline lower urinary tract disease; FUS = feline urological syndrome; IC = idiopathic cystitis
Diagnosis
Physical examination
Physical examination most often reveals an obese or over-conditioned cat that has turned yellow (Figure 1), although neither finding is a requirement nor pathognomonic. The very observant clinician may catch a whiff of acetone breath (or might be tempted to proclaim to those within hearing distance that they perceive this smell if the other pieces fit!). 12
Blood work
Regardless of etiology, poikilocytes and Heinz bodies, along with a mild to moderate non-regenerative anemia, may be found on a complete blood count (CBC) in HL cats, but these are non-specific findings. A mature neutrophilia is present in a few cases; otherwise CBC results can be influenced by the presence of a separate inflammatory or infectious disease.10,12,13,17
Abnormalities on the biochemical profile may include hyperglycemia as the result of stress, diabetes mellitus or acute severe pancreatitis. Hypoalbuminemia may be present in idiopathic HL or as a result of significant gastrointestinal disease. A low blood urea nitrogen results from derangements in processing of protein through the urea cycle. The majority of cats with HL (>80%) have a significant elevation in alkaline phosphatase (ALP) enzyme activity, and very few of these same cats will have any notable elevation in gamma-glutamyltransferase (GGT), an enzymatic pattern that is considered by many to be pathognomonic for feline HL.11,17
Alanine aminotransferase (ALT) and aspartate aminotransferase liver enzyme activity is mildly to moderately elevated in most cases of HL, while elevations in ALT similar to or greater than ALP should motivate a search for primary liver disease such as cholangitis or neoplasia.
An early study by Biourge et al 18 demonstrated that the elevation in ALP in anorectic cats precedes the elevation in total bilirubin seen in the majority of cats presenting for HL, which should raise a clinician’s index of suspicion and prompt early intervention.
Serum bile acids will be significantly elevated in cats with hyperbilirubinemia and so is an unnecessary diagnostic test in these cases.11,12,17 Elevated bile acids in cats that are not jaundiced may be an early indicator of HL and intrahepatic cholestasis, or indicative of a portosystemic vascular anomaly or hepatic failure secondary to another severe, chronic liver condition, both of which are rare in cats.
Electrolyte abnormalities and azotemia are non-specific findings secondary to anorexia, vomiting, diarrhea and dehydration, or in some cases a result of a concurrent condition such as kidney disease. Hypokalemia, hypo-magnesemia and hypertriglyceridemia are present in a significant percentage of cases, with hypercholesterolemia being less common.12,19 Hypophosphatemia resulting in hemolytic anemia was reported in one cat with idiopathic HL, but can also be seen in diabetic ketoacidosis or during the course of nutritional intervention. 20
A number of cats with HL will have abnormalities in one or more measures of coagulation – activated clotting time, prothrombin time, partial thromboplastin time, fibrinogen, fibrin degradation products, and proteins invoked by vitamin K absence – but clinically relevant bleeding abnormalities are rare.11,17,21 Thrombocytopenia (<80,000 platelets / ml) and an activated partial thromboplastin time >1.5 times the upper limit of the reference interval have been associated with severe bleeding during biopsy procedures13,22 (see ‘vitamin K’ box).
Urinalysis
Urinalysis reveals variable concentrating ability and frequent lipiduria, as can also be seen with renal tubular lesions.11,17 The presence of bacteriuria or growth of an organism on culture would suggest a concurrent condition such as a urinary tract infection or pyelonephritis.
Imaging
Imaging is frequently a component of the diagnostic work-up of an anorectic, vomiting, icteric cat. In cases of HL, hepatomegaly may be seen on abdominal radiographs, but this is a relatively subjective and non-specific finding. In one early study 23 hepatic hyperechogenicity relative to falciform fat was found to be an ultrasonographic change with 100% positive predictive value in diagnosing cases of severe HL. However, in several subsequent studies authors were unable to correlate hepatobiliary ultrasonographic findings with specific feline hepatic diseases.24,25 Ultrasonography continues to be a valuable tool for identifying hepatobiliary disease or non-hepatic abnormalities in cases of secondary HL. 26
Cytology
Ultrasound-guided fine-needle aspiration of the liver is frequently performed, although cytology may be misleading in cases of suspected idiopathic HL, where detection of nodular, localized or multifocal infiltrative lesions may be missed. 27 The use of an automatic Tru-cut biopsy gun device is not recommended in cats. 28 Fine-needle aspiration is preferred to other more invasive biopsy procedures because HL cats are not initially favorable anesthetic candidates and in the face of clotting abnormalities may benefit from prophylactic vitamin K administration (see ‘vitamin K’ box). Aspirated hepatocytes are filled with vacuoles which will often displace and deform the nucleus (‘signet ring’ structure).
The diagnostic work-up of HL is often considered complete at this point. If cytology reveals something besides the ‘classic’ appearance of vacuolated hepatocytes (inflammatory cells, cells with neoplastic characteristics, etc), is ‘non-diagnostic’, or if imaging suggests that hepatic tissue or other abdominal organs are abnormal enough to warrant a closer look, then either exploratory laparotomy or, if available, laparoscopic examination and biopsy would be the next logical step.
Histopathology
The gross appearance of the liver in a cat with HL, as seen during laparoscopy, is shown in Figure 2. At Colorado State University (CSU) laparoscopy is the technique of choice for obtaining hepatic biopsies, pancreatic biopsies and gall bladder aspirates (Figure 3), but many practitioners are adept at performing exploratory abdominal surgery for diagnostic samples with minimal morbidity.29–31 Surgery is also recommended in cases where an organ might need to be removed (eg, cholecystectomy).
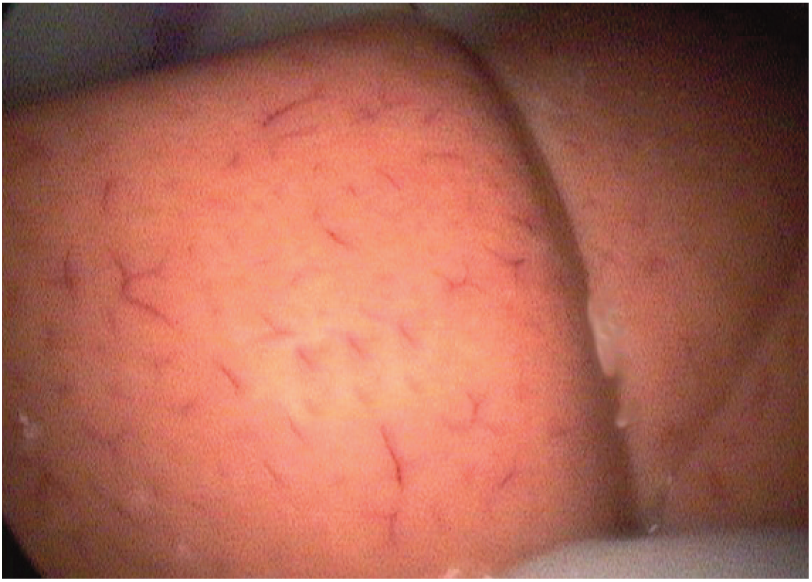
Enlarged pale liver lobes (laparoscopy) consistent with feline hepatic lipidosis. Courtesy of Dr David Twedt, Colorado State University

Spinal needle (16 G) used to aspirate the gall bladder during laparoscopy. Courtesy of Dr David Twedt, Colorado State University
Histopathology reveals diffuse lobular changes, with more than 50% of hepatocytes filled with cytoplasmic lipid-containing vacuoles (Figure 4).11,17 HL results in intrahepatic cholestasis, with structural changes that are distinct from cholestasis secondary to bile duct obstruction (ie, extrahepatic cholestasis). 32

Liver histopathology consistent with a diagnosis of feline hepatic lipidosis. Courtesy of Dr David Twedt, Colorado State University
Supportive treatment: addressing vital parameters, dehydration and electrolyte abnormalities
Supportive care aimed at stabilizing vital parameters and correcting dehydration (see summary box on fluid stabilization on page 221) and electrolyte abnormalities is the top priority in cats presenting with anorexia, vomiting, lethargy and/or icterus – all clinical signs consistent with HL.
Pre-renal azotemia, hypokalemia, hypo-phosphatemia and hypomagnesemia are likely therapeutic targets in cats with HL. Other abnormalities resulting from a concurrent disease, such as significant anemia, effusions, toxic neutrophils and fever, may warrant early intervention. Vomiting, pain and, rarely, signs of hepatic encephalopathy would require treatment as well. There are a number of excellent recent reviews outlining the approach to treating these problems in feline patients.35–39
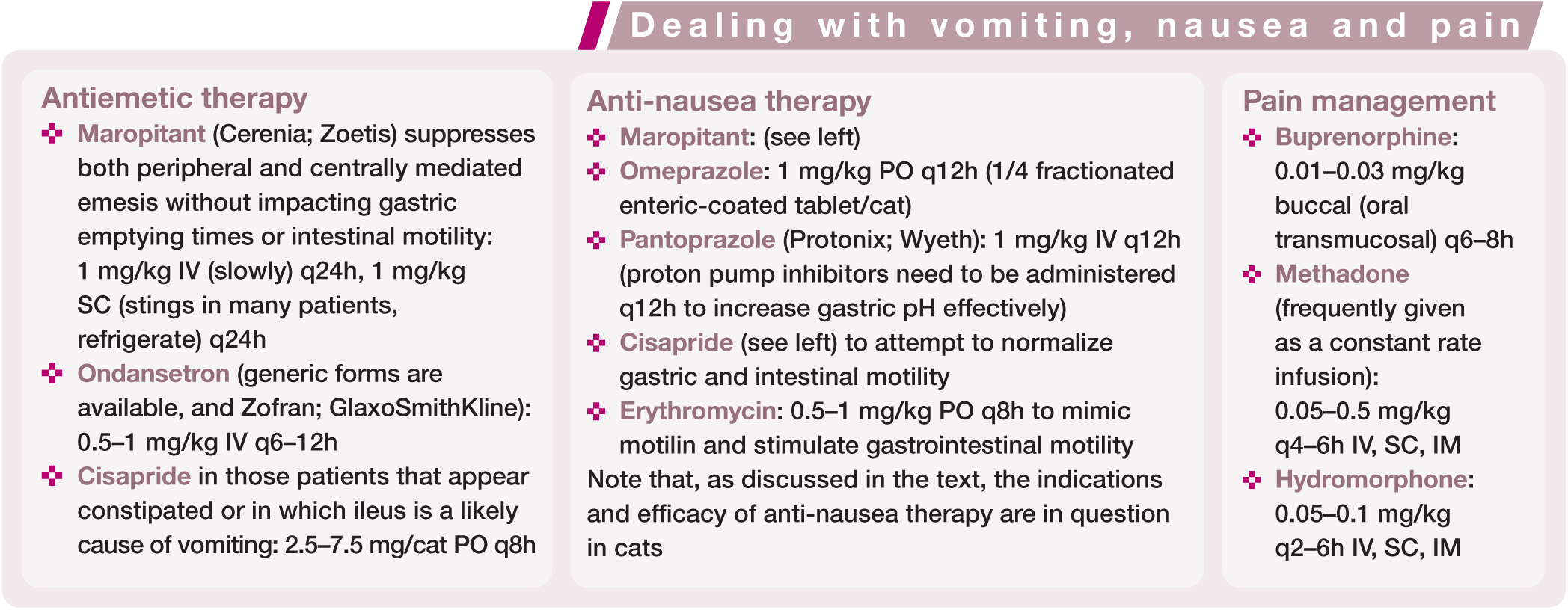
Antiemetic therapy
A common presenting complaint in cases of feline HL is vomiting. As soon as vomiting is no longer an assessment tool in case management (eg, possible foreign body obstruction scheduled for repeat radiographs), it should be addressed pharmacologically. The author’s preferred feline antiemetic is maropitant, although ondansetron is frequently used as well or in combination at CSU. A box on page 221 summarizes the relevant dose rates.
Anti-nausea therapy
In the absence of vomiting or ptyalism, assessing whether or not a cat is ‘nauseated’ is difficult, and although treatment for assumed nausea is frequently employed, the specifics and effectiveness of this strategy are up for debate. At CSU, maropitant is frequently administered to non-vomiting patients in the belief that it helps with nausea. Omeprazole or pantoprazole are also frequently administered for presumed antinausea effects (see box on page 221 for dose rates), although cats may not develop an ‘acid stomach’ as in other species, and the indiscriminant use of proton pump inhibitors or H2-receptor antagonists should be avoided. 40

Clinical signs of dehydration

Pain management
Pancreatitis is, historically, one of the earliest concurrent conditions reported in cats with HL (Table 1). 41 The definitive diagnosis of feline pancreatitis can be problematic, treatment is non-specific, and the prevalence is likely under-appreciated. A key therapeutic goal in cases of pancreatitis is the control of pain, whether clearly determined or wisely assumed. The author’s preferred treatment for the discomfort of pancreatitis (and other painful visceral conditions that might cause a cat to stop eating) is oral transmucosal buprenorphine. 42 Both a long-acting product (Simbadol; Zoetis) and a sustained-release formulation (Buprenorphine SR; SR Veterinary Technologies) have been recently introduced and may be used, although this decreases the owner’s ability to titrate the dose to effect. See the box below for dosages.
Other support
At CSU N-acetylcysteine is frequently administered (200 mg/ml, initial dose is 140 mg/kg; dilute a 20% solution 1:4 with D5W [5% dextrose in water], flush intravenous line with D5W first, then administer through a 0.22 μm filter over 20 mins; up to seven subsequent doses at 70 mg/kg q12h) as an antioxidant and liver ‘protectant’ shortly after admission in cases of significant liver damage or dysfunction.

Specific treatment: aggressive nutritional support
Aggressive nutritional support is the cornerstone of therapy. 11 From the first published case series, in 1989, it was recognized that the foundation of treatment for cats with idiopathic HL was to find a way to get nutrition into the cat. 47 In that particular report the cats were fed a balanced diet supplemented with L-carnitine via a gastrostomy tube. The feeding tube was utilized for an average of 48 days (range 22–98). 47
The majority of HL cats are anorectic for a reason, which might be a relatively obvious concurrent disease, or may be a subtle but, for the cat, stressful event that is only revealed by thorough questioning of the owner. 48 Clearly, any specific treatment(s) targeting that concurrent condition will play an important role in returning the cat to a state of voluntary ingestion. Unfortunately, obtaining a definitive diagnosis in cats is difficult; finding a feline disease that has a specific treatment is uncommon; getting that treatment into the cat can be challenging for a variety of reasons; and a large number of drugs used in feline medicine have gastrointestinal side effects that result in anorexia (eg, antibiotics).
For HL, nutrition is the specific therapy for the condition, and therefore early intervention is aimed at effectively getting nutrition into these patients.
There seem to be an infinite number of strategies for encouraging cats to eat voluntarily, with endless anecdotal reports of success. One such strategy, acupuncture, is incorporated by a number of clinicians at the author’s institution, with variable but seemingly patient-specific success. Unfortunately, by the time a cat with HL presents to a veterinarian it is extraordinarily unlikely that any of these efforts will be successful.
It is also unlikely that pharmacological appetite stimulation will be effective within the desired time frame, although it can be attempted. It is important to remember that by the time an anorectic cat with HL is presented for evaluation, that cat has likely not eaten for several days, and so any delay in the definitive administration of nutritional support is potentially deleterious. The feline appetite stimulant of choice at the author’s institution is mirtazapine. 49 Possible side effects include vocalization, agitation, vomiting, tremors and hypersalivation. 50 An alternative appetite stimulant would be cyproheptadine, but mirtazapine and cyproheptadine should not be combined as the two have antagonstic mechanisms of action. Dose rates for both are given in the box below. 51
Accessing the gastrointestinal tract
Total or partial parenteral nutrition strategies are beyond the scope of this review and require significant technical support for administration and monitoring.52,53 There are a number of variations on the design and placement of percutaneous endoscopic gastrostomy tubes or jejunostomy feeding tubes,54,55 but these are rarely used at the author’s institution and will not be covered in this review. ‘Force feeding’ by any means is not advised as there is a significant risk of aspiration pneumonia, food aversion and disruption of the bond between owner and pet. The risk of inducing a food aversion is particularly concerning in cats, and the best strategy is to support the cat’s nutritional plane in ways that do not require getting food through its mouth until it voluntarily resumes eating.
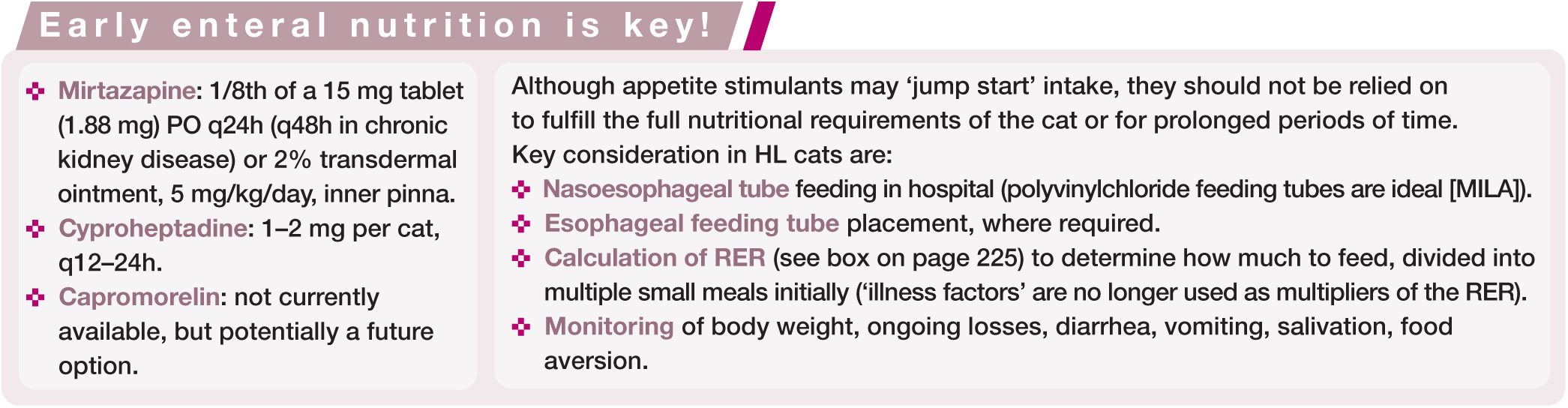
The quickest and easiest way to get nutrition into a cat in the clinic is a nasoesophageal (NE) feeding tube (see summary box below). Advancing the tube through the lower esophageal sphincter into the stomach makes it a nasogastric (NG) feeding tube, which some clinicians prefer because it allows suction of gastric contents or air (decompression). Cats are not sent home with NE or NG tubes in place; too frequently the tube is rendered useless by the cat shortly thereafter.
On the rare occasion when NE/NG tube feeding and appropriate supportive care proves insufficient to elicit voluntary eating an esophagostomy tube (E-tube) is placed (see box on page 224). Having established access to the cat’s gastrointestinal tract, the next question becomes what and how much to put in there?


Final nasoesophageal tube placement secured with sutures
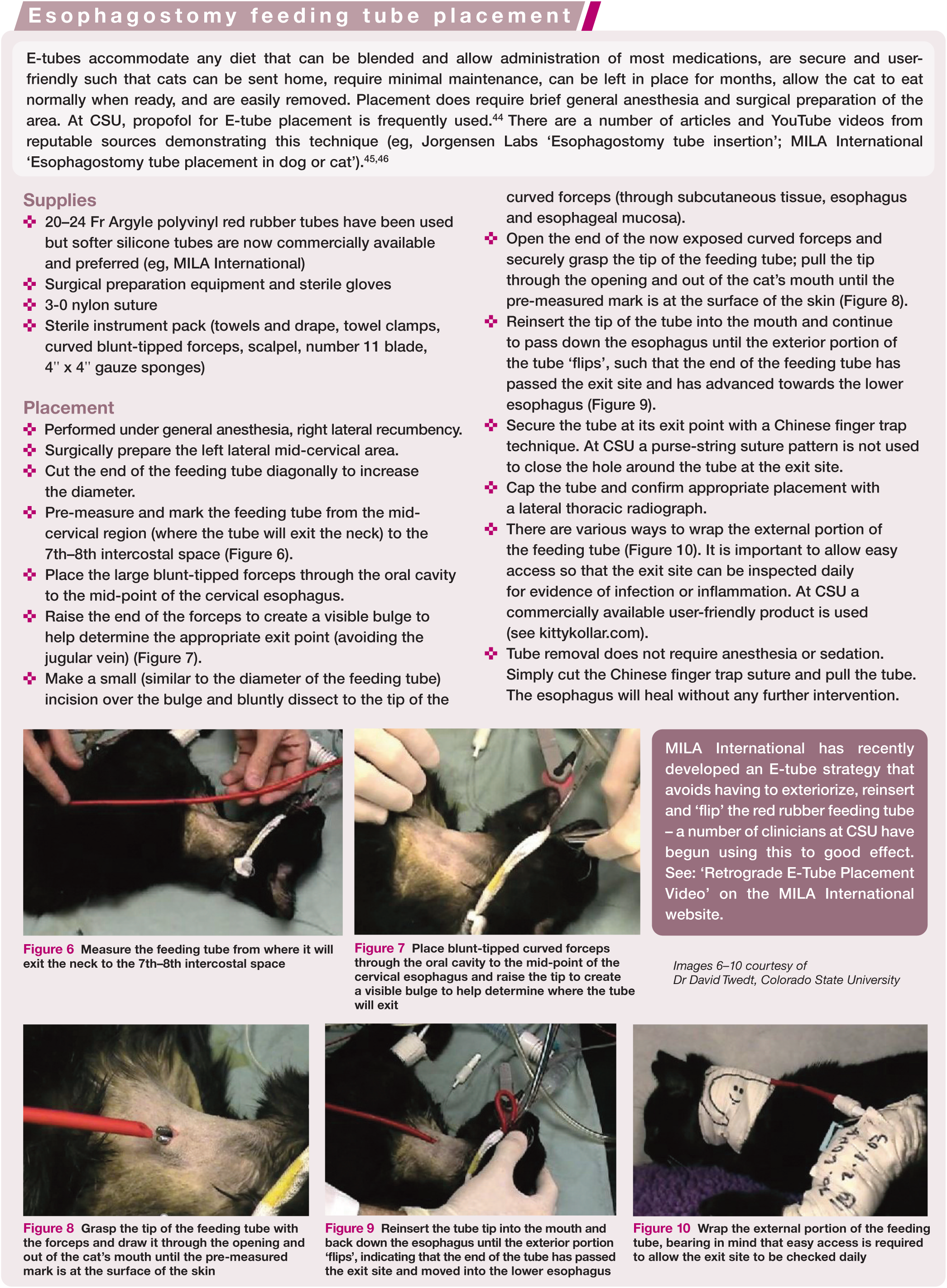

Measure the feeding tube from where it will exit the neck to the 7th–8th intercostal space

Place blunt-tipped curved forceps through the oral cavity to the mid-point of the cervical esophagus and raise the tip to create a visible bulge to help determine where the tube will exit

Grasp the tip of the feeding tube with the forceps and draw it through the opening and out of the cat’s mouth until the pre-measured mark is at the surface of the skin

Reinsert the tube tip into the mouth and back down the esophagus until the exterior portion ‘flips’, indicating that the end of the tube has passed the exit site and moved into the lower esophagus

Wrap the external portion of the feeding tube, bearing in mind that easy access is required to allow the exit site to be checked daily

How much to feed?
An excellent review article in this journal by Chan, ‘The inappetent hospitalized cat: clinical approach to maximizing nutritional support’ provides a step-by-step reference including an easy-to-follow flow chart that almost eliminates the need for a calculator! 56
The actual amount and schedule of feedings are based on common sense – starting with a portion (50%) of the resting energy requirement (RER; see box above) on day 1 and increasing gradually, using multiple smaller feedings initially (four per day, not to exceed 25 ml/meal) and thereafter simultaneously increasing volume (by 5 ml total per day) and decreasing frequency over time. It is important always to pay attention to the response of the cat and adjust accordingly.
Refeeding syndrome and hypophosphatemia with hemolysis have been associated with the initiation of enteral alimentation in cats with anorexia, hyperbilirubinemia and weight loss (see ‘Initial fluid stabilization of the sick cat’ box on page 221 for phosphate supplementation).57,58 Hypokalemia is a common and significant electrolyte abnormality in cats that can be addressed by adding potassium gluconate to the diet (see later). Heinz body formation may develop during the feeding process.
Although E-tube feeding of a cat feels incredibly user-friendly to veterinarians, it is still a ‘big deal’ for owners, at least initially. Spending time educating owners (including basic wound assessment and care), demonstrating techniques, sharing videos that they can refer to at home, staying in contact and rechecking biochemical parameters all helps to ensure success.
What to feed?
An argument can be made for any number of specific diets, dietary requirements and supplements, such as those listed in Table 3.59,60 However, many practitioners appear to be successful simply using a diet specifically formulated for cats, with high protein, high fat and low carbohydrate, avoiding any need for additional supplementation. Dr Sharon Center (Cornell) emphasizes the need to avoid negative nitrogen balance in these obligate carnivores by using diets that contain ⩾4.0 g/kg protein of high biologic value, to a total of 70–80 kcal/kg/day. 10
Supplementation of diets for cats with hepatic lipidosis 59

See text for discussion of potassium supplementation/dosing, and reduced dosing of L-carnitine
PO = oral; PUFA = polyunsaturated fatty acids
At CSU, feeding usually starts with one of the canned ‘recovery’ or ‘maximal caloric density’ diets that are easy to blend with an equal volume of water and require a simple calculation to determine the number of kcal/ml of slurry (usually between 1 kcal/ml and 2 kcal/ml). In the vast majority of cases no further supplements are added to those diets. However, potassium appears to be a particularly important electrolyte in sick cats, and hypokalemia is a negative prognostic indicator in cats with HL. 61 Fortunately, it is easily supplemented (2 mEq per day) with a variety of products. Some clinicians will add L-carnitine, although at a reduced dose from that given in Table 3 (7–14 mg/kg/day).
A significant number of cats with liver, gastrointestinal or pancreatic disease are hypocobalaminemic and so supplementary cobalamin is frequently given (starting with 250 μg SC injection once weekly). These cats are likely to be under some degree of oxidative stress (hence the vitamin E entry in Table 3), with reduced levels of an important antioxidant, glutathione, so S-adenosylmethionine (SAMe) may also be added to the treatment regimen. 62
Outcome
The response to treatment and the prognosis for cats with HL depend in large part on the concurrent disease that is frequently present. For example, cats with HL and acute pancreatitis had a 20% survival rate compared with cats with idiopathic HL, which had a 50% survival rate.16,63 In another report, in 4/11 cats with HL that died, the cause of death was inevitably a concurrent condition. 47 Cats with idiopathic HL are, in general, younger than cats with secondary HL, and more likely to survive. Regardless, there is a greater likelihood of survival in those HL cats where nutritional intervention is accomplished quickly and aggressively. 17 Fortunately, and somewhat surprisingly, it seems to be an almost universal observation that HL does not develop again in those cats that do survive.
Key Points
HL starts as a clinical diagnosis, based on a cat’s presentation, history and physical examination. Additional diagnostic tests may give results consistent with the clinical diagnosis.
Anorexia and weight loss are key presenting signs. Many cats are overweight before the weight loss.
The presence of concurrent disease will affect treatment and prognosis.
Supportive care aims to stabilize vital parameters and correct dehydration and electrolyte abnormalities.
Nutrition is the specific therapy for HL. Early intervention aims to get nutrition into these patients.
Footnotes
Conflict of interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.