
Abstract
Objectives
Ultrasonography can detect extrahepatic biliary obstructions. However, visualisation of part of the bile duct using ultrasonography can be technically difficult if there is overlying bowel gas. This study investigated the safety and value of drip infusion cholangiography with computed tomography (DIC-CT) in the visualisation of the bile duct in healthy cats and extrahepatic biliary obstruction in cats with cholelithiasis.
Methods
DIC-CT was performed in three healthy cats and two cats with cholelithiasis. Meglumine iotroxate was administered by intravenous drip infusion over 30 mins. The attenuation value was measured perpendicular to the lumen by a region of interest covering about 50% of the area of the lumen.
Results
The bile ducts were visualised successfully with DIC-CT in all healthy cats without any significant adverse events. The attenuation value of the contrast medium was 271 ± 37 HU. In the two cats with cholelithiasis, the presence or absence of extrahepatic biliary obstruction was determined using DIC-CT without any significant adverse events. The attenuation value of cholelithiasis in the cat with an extrahepatic biliary obstruction was 933 ± 119 HU. In the cat with no extrahepatic biliary obstruction, the attenuation value of the contrast medium was 249 ± 53 HU and the attenuation value of cholelithiasis was 167 ± 28 HU.
Conclusions and relevance
DIC-CT visualises bile ducts and detects obstructive biliary disease without significant adverse events. Therefore, it appears to be a safe procedure for visualisation of the bile duct in cats.
Introduction
In humans, drip infusion cholangiography with CT (DIC-CT) is a method that enables fast and non-invasive volumetric imaging of the bile duct. 1 DIC-CT reportedly detects obstructive biliary disease but carries the risk of adverse reactions. 2 The frequency of adverse events is reported to be as high as 3.4%. 2
In cats, ultrasonography enables the identification of an extrahepatic biliary obstruction and provides useful information for detecting the location and cause of obstruction. 3 However, visualisation of the bile duct using ultrasonography can be technically difficult if there is overlying bowel gas. 4 To our knowledge there are no reports in the literature that describe visualisation of the bile duct with DIC-CT in cats. The aim of this report was to evaluate the safety and the value of DIC-CT for the detection of extrahepatic biliary obstruction in cats.
Materials and methods
Three healthy cats and two cats with cholelithiasis, ranging from 8 to 10 years of age, were included in this study. In healthy cats, physical examination and haematological and serum biochemical analyses were performed immediately prior to DIC-CT, and immediately and 1, 3 and 7 days after DIC-CT. Haematological and serum biochemical analyses included the total white blood cell count, packed cell volume (PCV), total bilirubin (T-Bil), serum aspartate aminotransferase, serum alanine aminotransferase (ALT), serum alkaline phosphatase (ALP), total cholesterol, albumin, blood urea nitrogen and creatinine.
For the two cats with cholelithiasis, the case records of the Veterinary Teaching Hospital of Osaka Prefecture University were reviewed. Both cats underwent a physical examination, haematological and serum biochemical analyses, and ultrasonography prior to DIC-CT. Haematological and serum biochemical analyses included the ones performed in the healthy cats. A definitive diagnosis was made based on findings from a cholecystectomy.
For the CT evaluation, the cats were anaesthetised with intravenous propofol (Rapinovet; Schering-Plough Animal Health) and maintained with isoflurane and oxygen.
DIC-CT was performed using a multi-detector 16-slice CT scanner (Activion16; Toshiba Medical Systems). DIC-CT was performed with a pitch of 0.5, with increments of 0.5 mm, 100 mAs and 120 kV. Meglumine iotroxate (Biliscopin; 2 ml/kg) was administered by intravenous drip infusion over 30 mins with the animal conscious. The animal was anaesthetised immediately after the administration of contrast. The CT scanning started 1 h after the initiation of contrast administration. The patients were positioned in dorsal recumbency. Apnoea was induced during the image acquisition by stop ventilator. The attenuation value was measured perpendicular to the lumen by a region of interest covering about 50% of the area of the lumen.
Results
In healthy cats, DIC-CT was performed easily during the study. The contrast medium filled the gallbladder, cystic duct, hepatic duct, common bile duct and the duodenum quickly (Figure 1). The attenuation value of the contrast medium was 271 ± 37 HU. All the healthy cats experienced no significant adverse events. Results from laboratory tests showed that the haematology parameters remained within normal limits throughout the study.
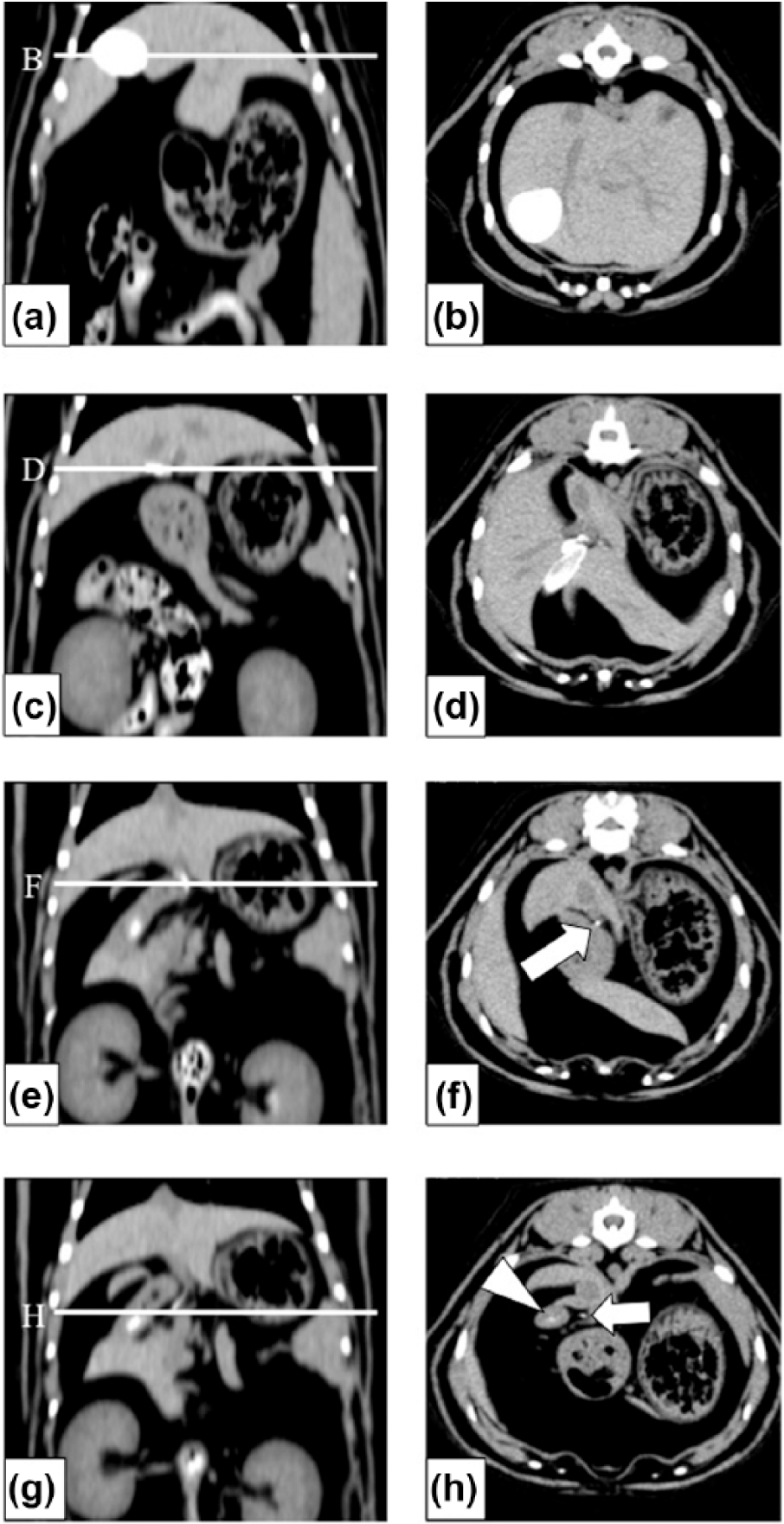
(a,c,e,g) Dorsal and (b,d,f,h) transverse CT images with meglumine iotroxate in healthy cats. (a,b) The contrast medium-filled gallbladder. (c,d) The contrast medium-filled cystic duct. (e,f) The contrast medium-filled hepatic duct. (g,h) The contrast medium-filled common bile duct (arrow) and duodenum (arrowhead). The animal was placed in dorsal recumbency
Case 1
A 10-year-old female mixed-breed cat presented with a 2 week history of intermittent vomiting. On physical examination, the cat was normal. Abdominal radiographs revealed cholelithiasis with the calculi located in the gallbladder and bile ducts (Figure 2A). The ultrasonographic examination could not identify common bile duct dilatation by acoustic shadow of cholelithiasis and ring-down artefacts of overlying bowel gas. Serum biochemical analyses revealed high serum activity levels of ALT (>900 IU/l), ALP (182 IU/l) and T-Bil (0.8 mg/dl). The results from the DIC-CT were indicative of an extrahepatic biliary obstruction. There was no contrast medium in the gall bladder, common bile duct or duodenum. Cholelithiasis was detected in the gallbladder and cystic, hepatic and common bile ducts (Figure 2b–d). The attenuation value of cholelithiasis was 933 ± 119 HU (Figure 2). The diameter of the common bile duct suggested a dilatation (5.6 mm). There were no significant adverse events. With the patient still under anaesthesia, surgery was performed after the diagnosis of an extrahepatic biliary obstruction by DIC-CT. When the cholecystectomy was performed, the obstruction in the cystic duct or common bile duct was released. Postoperative medical treatment consisted of ursodeoxycholic acid (10 mg/kg, q24h Gokumisin; Nipro Pharma). The results of serum biochemical analyses were normal 21 days postoperatively. The cat was asymptomatic.
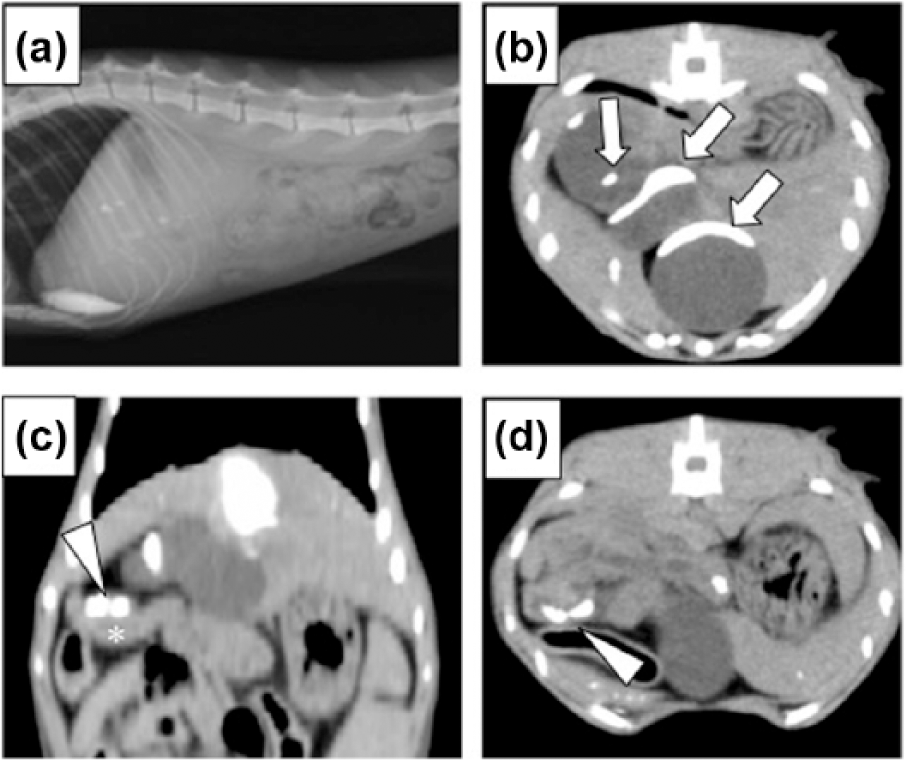
(a) Left lateral abdominal radiograph and (b,d) transverse and (c) dorsal CT post-contrast images with the animal (case 1) in dorsal recumbency. (a) Cholelithiasis was located in the gallbladder and bile ducts. (b–d) Cholelithiasis was observed in the gallbladder (arrows) and common bile duct (arrowhead). Asterisk indicates the duodenum
Case 2
A 9-year-old castrated male Abyssinian cat presented with intermittent vomiting. On clinical examination, the cat was found to be normal. Abdominal radiographs of the liver (Figure 3a) and serum biochemical analyses revealed no abnormalities. Haematological analyses revealed anaemia (PCV 27%). Ultrasonography identified cholelithiasis with an acoustic shadow. DIC-CT results indicated no extrahepatic biliary obstruction. The contrast medium filled the hepatic and common bile ducts and the duodenum quickly (Figure 3b,c). The attenuation value of contrast medium was 249 ± 53 HU (Figure 3c). Cholelithiasis was detected in the gallbladder. The attenuation value of cholelithiasis after contrast administration was 167 ± 28 HU (Figure 3b). There were no significant adverse events. With the patient still under anaesthesia, surgery was performed after the diagnosis of cholelithiasis by DIC-CT. When the cholecystectomy was performed, the absence of an obstruction in the cystic duct or common bile duct was determined by using a soft catheter.

(a) Left lateral abdominal radiograph and (b,c) transverse CT post-contrast images with the animal (case 2) in dorsal recumbency. (a) Abdominal radiographs of the liver region revealed no abnormalities. (b) Cholelithiasis was observed in the gallbladder (arrows). (c) The contrast medium-filled common bile duct (open arrow) and duodenum (arrowhead)
Discussion
An extrahepatic biliary obstruction is uncommon in cats. The most common causes of extrahepatic biliary obstruction include cholangiohepatitis (with or without bile inspissation), acute necrotising pancreatitis, extra- or intra-luminal masses, cholelithiasis and congenital abnormalities of the extrahepatic biliary tract. 3 Ultrasonography can identify an extrahepatic biliary obstruction, 3 which is diagnosed by a dilation of the gallbladder or common bile duct (⩾ 5 mm). 5 However, ultrasonography is associated with the technical difficulty of bile duct visualisation if there is overlying bowel gas. 4
In humans, DIC-CT is a non-invasive diagnostic method used to detect gallstones or to visualise bile duct disease.2,6 This examination provides pre-therapeutic information of an obstruction with significant dilatation. The diagnostic value of DIC-CT was rated as moderate or good in >93% of the examinations in humans. 2 In DIC-CT, the attenuation value of the main biliary duct was 261 HU. 2 The attenuation value of cholelithiasis depends on the presence of any degree of calcification. 7 Meglumine iotroxate, which has protein-binding characteristics, increases the risk of adverse reactions. 8 The frequency of adverse events associated with meglumine iotroxate infusion has been reported to be as high as 3.4%. 2 In humans, DIC-CT carries the risk of adverse reactions, including anaphylaxis, urticaria and respiratory distress. 2
In healthy cats, DIC-CT detected the bile duct without significant side effects. There were no haematological or serum biochemical abnormalities. In case 1, an attenuation value (933±119 HU) higher than that of contrast medium (271±37 HU) in healthy cats suggests that there was no filling of the gallbladder and common bile duct nor did the contrast medium flow into the duodenum. Therefore, a region with a high attenuation value was considered diagnostic for cholelithiasis. An extrahepatic biliary obstruction was caused by cholelithiasis. In case 2, the attenuation value of the hepatic duct, common bile duct and duodenum was 249 ± 53 HU. Therefore, we considered that the contrast medium filled the hepatic and common bile ducts, and entered the duodenum. The extrahepatic biliary obstruction was not caused by cholelithiasis.
The attenuation value of cholelithiasis in case 1 (933±119 HU) was higher than that in case 2 (167 ± 28 HU). Unfortunately, we did not perform a component analysis of cholelithiasis. This difference in the attenuation value may be affected by the components of the cholelithiasis. DIC-CT detected an extrahepatic biliary obstruction without the influence of cholelithiasis or bowel gas. There were no significant adverse events after DIC-CT.
Conclusions
DIC-CT allows visualisation of the bile ducts and detects obstructive biliary disease without significant side effects. It has the ability to visualise the bile duct in cats. However, because of the small number of participants in this study, further studies are required in order to verify the safety and value of DIC-CT in cats.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.