
Abstract
Case series summary
This report summarises and reviews the published cases of open-mouth jaw locking in cats and describes three further cases. Case 1 was a 5-year-old, 5.3 kg male neutered domestic shorthair cat. CT identified changes consistent with temporomandibular joint (TMJ) dysplasia with osseous degenerative changes, and the cat subsequently underwent bilateral partial zygomectomy with bilateral partial coronoidectomy. Case 2 was a 10-year-old, 6.0 kg male neutered Exotic Shorthair. Aside from a fracture of the left maxillary canine tooth crown and absence of the left maxillary fourth premolar tooth, no abnormalities were found on CT scan. The cat also underwent bilateral partial zygomectomy with bilateral partial coronoidectomy. The third case was a 1-year-old, 4.0 kg male neutered Persian cat. Changes on CT were consistent with bilateral TMJ dysplasia, and the cat underwent staged bilateral partial zygomectomy with bilateral partial coronoidectomy. There was no recurrence of open-mouth jaw locking in any of the cases on long-term follow-up.
Relevance and novel information
Open-mouth jaw locking has been reported in cats of a wide range of ages, from 1–10 years. Cats with all skull types (brachycephalic, mesaticephalic and dolichocephalic) may be affected, but brachycephalic breeds seem to be over-represented. A CT scan with the jaw locked in place is recommended for diagnosis and surgical planning purposes; two of the cases reported here document the first cases of TMJ dysplasia in cats to be definitively diagnosed using CT. Trauma and symphyseal or TMJ laxity may also predispose to development of the condition. Partial coronoidectomy and partial zygomatic arch resection performed alone or in combination are generally successful at preventing recurrence. Bilateral partial zygomectomy with bilateral partial coronoidectomy has not previously been reported as a surgical treatment, and is recommended when open-mouth jaw locking occurs bilaterally.
Introduction
Open-mouth jaw locking is characterised by an inability to close the mouth as a result of ventrolateral displacement of the mandibular coronoid process relative to the zygomatic arch following full-mouth opening (eg, playing with large objects, yawning). The condition may occur unilaterally or bilaterally, and animals present with the mouth wide open and the mandible tilting downwards on the locked side. A bony prominence (the coronoid process) may be felt adjacent to the ipsilateral zygomatic arch. Signs such as salivation, pawing at the mouth and apparent pain and distress are often seen.1–4 The condition is well documented in dogs but remains rare in cats, with only 11 previous cases reported in the literature.1–9 This report includes three new cases where CT was used in the diagnosis and surgical planning of this unusual disorder.
Case series description
Case 1
A 5-year-old, 5.3 kg male neutered domestic shorthair cat presented to the orthopaedic department of Langford Vets (University of Bristol), following five episodes of open-mouth jaw locking. The cat had a history of chronic gingivostomatitis and had undergone extraction of all teeth except the canines, incisors and the mandibular left fourth premolar (308) 17 months prior to presentation. All five episodes of open-mouth jaw locking had occurred within a 2 week period, and all but the first episode had required manual realignment of the mandible under sedation by the referring veterinary surgeon. The episodes were thought to be associated with yawning and had occurred either at night or in the early morning. The owner reported that the second time the jaw locked it was wider than all other times (>1–2 cm); the cat was subjectively painful and/or distressed, was drooling saliva and vocalising excessively. During all other episodes the cat was unable to eat or drink and was subdued, but no distress or pain response was observed. Between locking episodes the cat exhibited normal behaviour.
On physical examination all cardiovascular parameters were within normal limits. Mild gingivitis was noted adjacent to the remaining teeth. Palpation of the skull did not reveal any abnormalities. The cat was admitted to the hospital for further investigations and was sedated with 5 μg/kg intravenous (IV) dexmedetomidine and 0.3 mg/kg IV butorphanol. To make a definitive diagnosis and to assess potential underlying causes of the open-mouth jaw locking, CT of the head was carried out using a 16 slice Siemens Somaton CT scanner. Scans were performed with the jaw open and closed; however, it was not possible to recreate the open-mouth jaw locking under sedation. CT images were analysed by a European College of Veterinary Diagnostic Imaging board-certified specialist using an OsiriX (Pixmeo) open-source DICOM viewer. On the closed-mouth images, the retroarticular processes of the temporal bone were elongated bilaterally and extended more rostrally and ventrally than normal, partially enclosing the condyloid process of the mandible. Both condyloid processes were irregular and flattened dorsally (Figure 1). No abnormalities of the mandibular symphysis were identified. On the open-mouth images, the right temporomandibular joint (TMJ) space was completely collapsed and the left TMJ space was narrow, but the coronoid processes were not displaced lateral to the zygomatic arches. The changes were consistent with TMJ dysplasia with osseous degenerative changes. The sedation was reversed with 250 μg/kg intramuscular (IM) atipamezole and the patient was returned to the feline ward overnight. The following day, the cat was premedicated with 0.2 mg/kg IV methadone and 5 μg/kg IV dexmedetomidine, and general anaesthesia was induced with 1 mg/kg IV alfaxalone. The patient was intubated with a 5 mm internal diameter endotracheal tube and anaesthesia maintained using isoflurane (1–1.8%) in 100% oxygen (1.5–2.5 l/min) via a T-piece circuit. Throughout anaesthesia the cat was monitored with non-invasive blood pressure monitoring, a lead II electrocardiogram (ECG), oral temperature probe, capnograph and pulse oximeter. Compound sodium lactate solution was administered at 12 ml/h and a 50 ml bolus was given over 10 mins during anaesthesia to address hypotension. Under anaesthesia it was possible to recreate open-mouth jaw locking manually on both sides. The CT was repeated with the jaw locked on the left side, which showed ventrolateral displacement of the coronoid process of the mandible and subluxation of the left TMJ (Figure 2). A diagnosis of open-mouth jaw locking due to impingement of the coronoid process on the ventrolateral aspect of the zygomatic arch was made, which was thought most likely to be secondary to the TMJ dysplasia. The cat was prepared for surgery of both lateral aspects of the face by clipping the hair over the surgical sites and aseptically preparing the skin. The cat was initially positioned in right lateral recumbency and draped for surgery of the left lateral facial area. The mouth was locked open on the left side by the anaesthetist, and a 5 cm incision through the skin and subcutaneous tissue was made over the ventral border of the rostral portion of the zygomatic arch, where the displaced coronoid process could be felt. The fascial attachments to the arch were elevated, taking care to preserve the dorsal buccal branch of the facial nerve. A 3 cm incision was made into the periosteum, which was subsequently lifted from the zygomatic bone using a periosteal elevator. Visualisation of the coronoid process of the mandibular ramus in contact with ventral lateral zygomatic arch was obtained, enabling identification of the structures that required removal (Figure 3). Using an air-powered 3 mm sphere-shaped diamond spinal bur, a full-bone-width portion of the rostral zygomatic arch measuring 10 mm in length was removed. This was followed by removal of the dorsal 4 mm of the coronoid process. The periosteum and subcutaneous tissues were closed separately with 4-0 poliglecaprone 25 (Monocryl; Ethicon) in simple continuous pattern. Four 4-0 nylon cruciate sutures were placed to appose the skin edges. The patient was repositioned into left lateral recumbency and the procedure repeated for the right side, using the same technique. Meloxicam 0.1 mg/kg SC was administered prior to recovery. Analgesia postoperatively was provided by methadone 0.2 mg/kg IV q4h over 20 h and subsequently with buprenorphine 0.02 mg/kg IV for the following 12 h. The initial injection of meloxicam was followed with 0.05 mg/kg orally (PO) meloxicam, which was dispensed for the owner to administer once daily for 5 days. The patient began eating the following morning and was discharged later that day. To minimise postoperative pain, a soft diet was recommended for 2 weeks following surgery. When at home, the owner noted in the cat an inability to settle, including periods of running around in an agitated manner and excessively licking itself. Oral buprenorphine was prescribed by the referring veterinary surgeon, which reportedly alleviated the signs initially, and the meloxicam was continued. The cat had been trying to scratch at its face, mostly on the left side, but had not been able to remove the buster collar. By day 10 postoperatively the wounds were healing satisfactorily and the sutures were removed. The altered behavioural signs had continued and so a 10 day course of gabapentin (50 mg PO twice daily) was prescribed. After completion of the gabapentin course, two sessions of acupuncture and two sessions of cold-laser therapy were undertaken at the referring veterinary surgeon. In total, the meloxicam was continued for 6 weeks postoperatively. At 7 weeks postoperatively, the owner reported that the patient had recovered fully and there were no further signs of pain or discomfort. The patient continued to eat and yawn normally throughout recovery with no apparent discomfort. At the 3 and 10 month telephone call follow-ups, there had been no recurrence of jaw locking, and the patient was able to yawn and eat without showing pain or discomfort, and was behaving normally.

(a) Case 1, sagittal CT scan showing subluxation of the left temporomandibular joint (arrow), retroarticular process elongation (arrowhead) and dorsally flattened condyloid process. (b) Sagittal CT of a normal feline skull at the same level for comparison. 1 = condyloid process; 2 = mandibular fossa of the temporal bone; 3 = temporal bone; 4 = mandible; 5 = external acoustic meatus; 6 = orbit
Case 1, CT three-dimensional reconstruction of the skull showing displacement of the left coronoid process ventrolateral to the zygomatic arch (arrow)

Case 1, intraoperative photograph showing ventrolateral displacement of the left coronoid process (arrow). Z = zygomatic arch; C = coronoid process
Case 2
A 10-year-old, 6.0 kg male neutered Exotic Shorthair cat presented to the orthopaedic department of Langford Vets (University of Bristol), following an 18 month history of open-mouth jaw locking. The first locking episode was reduced by the referring veterinary surgeon under general anaesthesia. An uncomplicated (without pulp exposure) fracture of the maxillary left canine tooth was identified, and a mild degree of TMJ laxity was found on manipulation of the mandible. There was no recurrence for 13 months following this incident and the patient exhibited normal behaviour. However, over the 5 months prior to referral there had been a further five open-mouth jaw-locking episodes, each occurring approximately 1 month apart. The owner reported that the episodes usually happened overnight and the jaw would never unlock spontaneously. The owner was able to manually reduce the open-mouth jaw locking at home on two occasions, but the other occasions required reduction of the jaw under sedation by the referring veterinary surgeon. The patient did not appear to be distressed when the jaw was locked, and would continue to eat even immediately after manual reduction of the jaw. There was no history of trauma, and no difficulty in yawning or eating had ever been perceived. The patient had a 5 year history of chronic kidney disease, which was stable and was being treated with benazepril (2.5 mg PO once daily). The cat had also undergone a right keratectomy, conjunctival graft and Hotz-Celsus procedure for a sequestrum and entropion 2 years prior to the onset of the open-mouth jaw locking. Physical examination of the cat was unremarkable. There was no evidence of instability or luxation of the mandible at presentation. The cat was admitted for further investigations. A blood sample was obtained from the jugular vein for biochemistry analysis. The results showed a mild azotaemia with a mild hyperphosphataemia (urea 12.6 mmol/l [reference interval {RI} 6.5–10.5 mmol/l]; creatinine 195 μmol/l [RI 133–175 μmol/l], phosphate 1.68 mmol/l [RI 0.95–1.55 mmol/l]). An increase in creatinine kinase was also noted (530 IU/l [RI 50–150 IU/l]). The cat was sedated with 5 μg/kg IV dexmedetomidine and 0.3 mg/kg IV butorphanol. A further 2.5 μg/kg IV dexmedetomidine was administered to maintain sedation. CT of the head was carried out, first with the jaw closed and then with the jaw locked open on the right side. It was also possible to lock the jaw on the left side. On the closed-mouth images the skull was noted to be markedly brachycephalic. The left maxillary canine tooth crown was fractured (uncomplicated crown fracture) and the left maxillary fourth premolar tooth was absent. Both TMJs were normal, and there were no abnormalities of the mandibular symphysis. On the open, locked-jaw images, the right coronoid process of the mandible was displaced ventrolateral to the right zygomatic arch (Figures 4 and 5), and the right TMJ was luxated with the condyloid process of the mandible rostral to the mandibular fossa of the zygomatic process of the temporal bone (Figure 4). The left TMJ was subluxated with the condyloid process again displaced rostrally but remaining in contact with the mandibular fossa. No underlying cause of the open-mouth jaw locking could be determined from the images. The patient was administered 250 μg/kg IM atipamezole. Following this the patient was discharged to allow time for the owners to consider whether to opt for surgical intervention. Two weeks later the cat was admitted for surgery. A premedication of 0.3 mg/kg IV methadone and 3 μg/kg IV dexmedetomidine was administered. General anaesthesia was induced via 1.8 mg/kg alfaxalone IV. The patient was intubated with a 3.5 mm internal diameter endotracheal tube and anaesthesia maintained using isoflurane (1.3–2%) with 100% oxygen at 3 l/min via a T-piece circuit. Throughout the anaesthetic the cat was monitored with non-invasive blood pressure monitoring, a lead II ECG, oral temperature probe, capnograph and pulse oximeter. Compound sodium lactate solution was administered at 20 ml/h, and 20 mg/kg of cefuroxime was administered IV every 90 mins until the end of surgery. A temporary tarsorrhaphy was performed bilaterally to prevent damage to the eyes, and the surgical sites were prepared as for the first case. An approach through the skin and underlying soft tissues was created in a similar fashion as for case one. An air-powered 3 mm sphere-shaped diamond spinal bur was used to remove 4 mm from the dorsal aspect of the coronoid process. A partial zygomectomy was performed involving resection of a 10 mm long portion of the rostroventral margin (approximately one-quarter of the width of the zygomatic arch) to prevent locking. The surgery was repeated on the contralateral side. The temporary tarsorrhaphy sutures were removed at the end of surgery. Buprenorphine was administered at 20 μg/kg IV q6h postoperatively, and the cat began eating within 12 h of surgery. It was discharged the following day with a 2 day course of sublingual buprenorphine (20 μg/kg q8h). The cat’s renal disease precluded the use of non-steroidal anti-inflammatory drugs (NSAIDs). It was recommended that the cat be fed soft food for 2 weeks. The cat continued to eat at home, and no postoperative complications were encountered. At the 4 and 10 month telephone call follow-ups, there had been no recurrence of jaw locking, the patient was able to yawn and eat without apparent pain or discomfort, and was behaving normally.
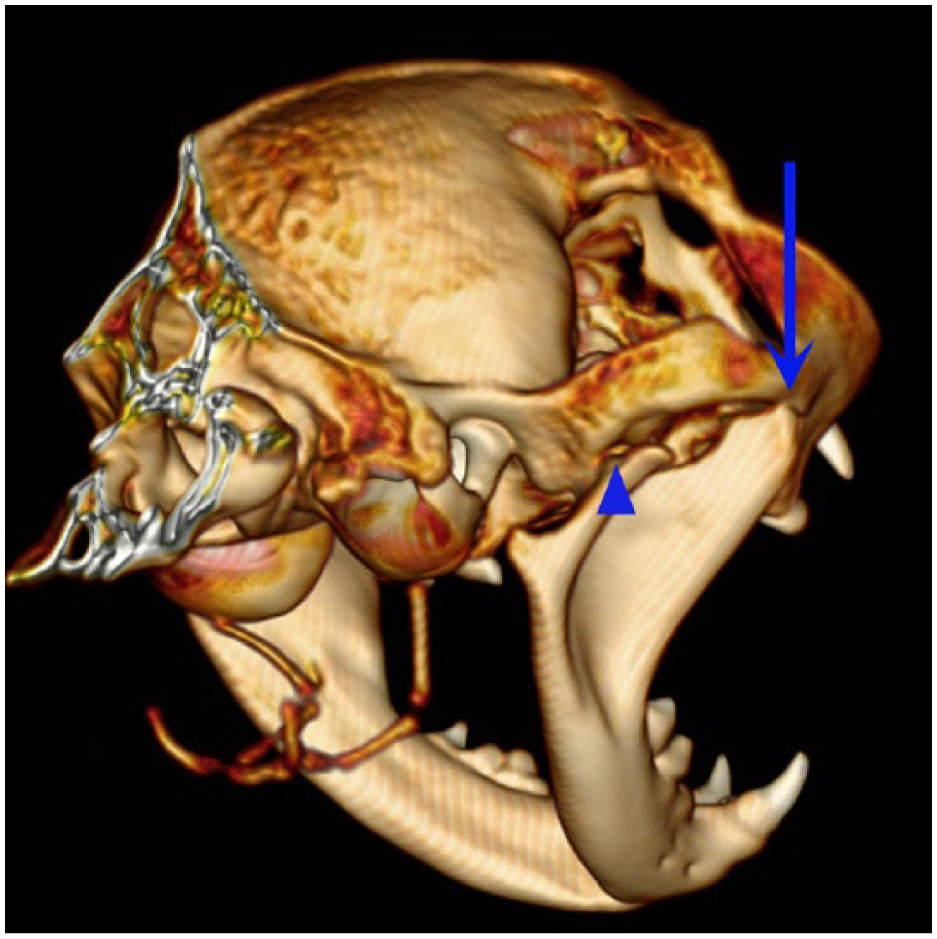
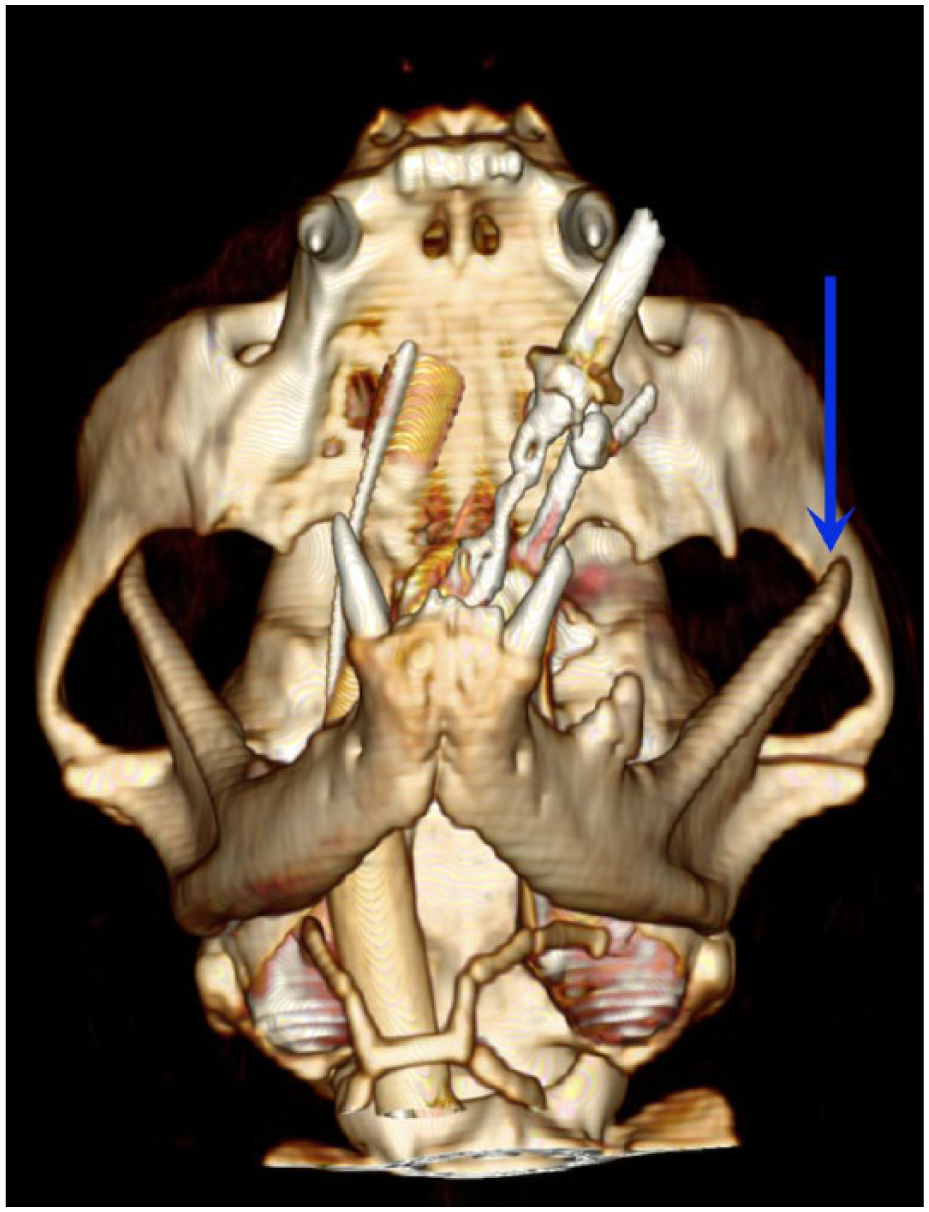
Case 2, CT three-dimensional reconstruction of the skull showing luxation of the right temporomandibular joint (arrowhead) and displacement of the right coronoid process ventrolateral to the zygomatic arch (arrow)

Case 2, transverse CT scan showing displacement of the right coronoid process ventrolateral to the zygomatic arch (arrow). Z = zygomatic arch, C = coronoid process, M = mandible, O = orbit, NP = nasopharynx
Case 3
A 1-year-old, 4.0 kg male neutered Persian cat presented to the Veterinary Clinic Città di Codogno (Codogno, Lodi, Italy) with a 3 month history of recurrent open-mouth jaw locking. Initially, the cat was able to unlock the mandible spontaneously, with quick relapses. The referring veterinarian was also able, on a few occasions, to manually unlock the mandible without the need for sedation or anaesthesia. One month before presentation, the cat had been treated at the referring practice with a bilateral maxillomandibular fixation device, whereby a non-absorbable suture was passed full thickness from the upper to lower lips, to impede full mandibular extension. However, 5 days after the removal of the labial sutures, a further episode of open-mouth jaw locking occurred, with recurrence happening almost every night thereafter. A radiographic examination of the skull (ventrodorsal, right and left lateral oblique and rostrocaudal open-mouth projections) was performed by the referring veterinarian and showed subluxation of the left TMJ and displacement of the right coronoid process of the mandible ventrolateral to the zygomatic arch when the mouth was locked open. A week before presentation, the cat had fallen from a table and developed a hindlimb lameness, which was treated conservatively with NSAIDs.
On presentation, the cat was in excellent body condition. Slight relative mandibular prognathism and anterior reverse scissor bite were visible. The range of motion of the mandible was considered normal and the symphysis was stable on manipulation. The owners indicated that the mandible locked mostly on the right side (with slight right ventrolateral rotation of the mandible), but the precise frequency of right and left dislocations could not be determined. A blood sample was obtained from the jugular vein for biochemistry analysis. The results showed mild hypercalcaemia (10.7 mmol/l [RI 7–10 mmol/l]), leukocytosis (21.8 ×109/l [RI 5.0–18.0 ×109/l]), neutrophilia (14.9 ×109/l [RI 2.5–12.5 ×109/l]), increased red blood cell count (9.69 ×1012/l [RI 4.0–9.0 ×1012/l]) and increased mean platelet volume (9.6 fl [RI 4.0–7.0 fl]).
The cat was referred to a specialist centre (Clinica Veterinaria dell’Orologio, Sasso Marconi, Bologna, Italy) for CT the same day. The imaging was carried out with the mouth closed, the mouth open and, finally, with the mandible locked open on the left side. Subluxation of the left TMJ joint and displacement of the left coronoid process of the mandible ventrolateral to the left zygomatic arch were seen when the jaw was locked open. The right and left mandibular condyloid process and mandibular fossa of the mandibular process of the temporal bone were flattened (Figure 6). The mandibular symphysis was normal. The following day the cat was admitted for surgery. A premedication of 0.1 mg/kg IM morphine, 3 mg/kg IM ketamine and 4 μg/kg IM dexmedetomidine was administered. General anaesthesia was induced with 2 mg/kg IV propofol. The patient was intubated with a 3.5 mm internal diameter endotracheal tube, and anaesthesia was maintained using isoflurane (1–2%) with 100% oxygen at 1.5 l/min via a T-piece circuit. Throughout the anaesthetic the cat was monitored with non-invasive blood pressure monitoring, a lead II ECG, anal temperature thermometer, capnograph and pulse oximeter. IV lactated Ringer’s solution was administered at 10 ml/h throughout the procedure, and one dose of cefazoline (30 mg/kg) was administered IV. Under anaesthesia it was possible to recreate open-jaw locking manually on both sides. A click noise at the right TMJ was produced during locking on the right side. Ventrodorsal radiographs of the locked temporomandibular joints were obtained with dental radiographs (Kodak size DF50, Ultra-Speed dental films) placed extraorally (Figure 7). Given that the mandible was reported to lock on the right side, surgical treatment was initially performed unilaterally. The cat was positioned in left lateral recumbency and right left maxillary nerve block was administered through a cutaneous, subzygomatic approach using 0.05 ml 2% lidocaine and 0.15 ml 0.5% bupivacaine solution. The skin was prepared for surgery on the right side of the face as described for the previous two cases. An approach through the skin and underlying soft tissues was created in a similar fashion as for the other cases. A #2 tungsten dental bur on a high-speed drill was used to remove 5 mm bone from the dorsal aspect of the coronoid process and a 10 mm full-thickness section of bone from the mid-portion of the zygomatic arch, to prevent locking. After ensuring that right jaw locking could not be reproduced manually by maximally opening the mouth, rotating the mandible towards the right side, and closing the mouth, the periosteum and subcutaneous tissues were closed separately with 5-0 poliglecaprone 25 (Monocryl; Ethicon) in a simple continuous suture pattern. The skin was then closed using skin staples. Postoperative analgesia was achieved by administration of IM meloxicam (0.1 mg/kg once) and morphine (0.2 mg/kg q8h for 24 h). The cat was discharged the following day and the clients were instructed to continue meloxicam treatment (0.05 mg/kg PO once daily for 5 days), disinfect the wound daily and have the cutaneous staples removed 10 days following surgery. It was recommended that the cat be fed its normal dry diet.

(a) Case 3, three-dimensional CT reconstruction of the skull showing the subluxated left temporomandibular joint during left open-mouth jaw locking. Flattening of the left condyloid process and mandibular fossa of the temporal bone (arrow) is evident and there is widening of the joint space. Courtesy of Clinica Veterinaria dell'Orologio, Sasso Marconi, Bologna, Italy. (b) Three-dimensional CT reconstruction of a normal feline skull for comparison. 1 = condyloid process; 2 = mandibular fossa of the temporal bone; 3 = zygomatic arch; 4 = mandible; 5 = external acoustic meatus; 6 = hyoid apparatus; 7 = temporal bone

(a) Case 3, ventrodorsal extraoral radiograph of the right temporomandibular joint showing displacement of the right coronoid process ventrolateral to the zygomatic arch (arrow) during right open-mouth jaw locking. The mandible is rotated and appears oblique because of the jaw locking. (b) Ventrodorsal extraoral radiograph of a normal feline skull for comparison. Z = zygomatic arch; C = coronoid process
Two weeks following discharge a new episode of jaw locking happened, this time to the left side. The referring veterinarian was able to manually reduce the locking by gentle traction on the left mandibular canine tooth. This happened four more times until the cat was brought back to us 3 weeks after the initial surgical procedure. The skin wound on the right side of the face appeared completely healed. Jaw locking could not be induced manually on either side in the animal awake, but once under anaesthesia (using the same anaesthetic protocol described for the first surgical procedure) the mandible could easily be locked to the left side by opening the mouth maximally and slightly rotating the mandible towards the left side. A click noise at the right TMJ was again heard, which was thought most likely to be due to subluxation of the TMJ, although it was not possible to determine this definitively. The mandible could not be locked to the right side. Dental occlusal size radiographic films were used again with an extraoral technique, which confirmed left-sided locking. The surgery was repeated on the left side as described previously for the right side, except that the skin closure that was performed by placing sutures using 4-0 nylon (Ethilon; Ethicon). The cat was discharged the following day with the same medication and instructions given after the first procedure. There has been no recurrence of jaw locking 8 years following surgery.
Literature review
Of the cases described in the literature, including the additional three reported here, nine were male (six neutered) and five were female (four neutered), with a median age of 3 years and mean age of 4.4 years. Eight cats were Persian, two Siamese, two domestic shorthair, and there was one Siamese crossbreed and one Exotic shorthair (Table 1).
Summarised details of the cases previously described in the literature, and the additional three reported in this article

FN = female neutered; TMJ = temporomandibular joint; MN = male neutered; DSH = domestic shorthair; F = female intact; M = male intact; SC = Siamese crossbred; ES = Exotic shorthair
Open-mouth jaw locking in cats has been assumed to be a result of TMJ dysplasia with or without excessive TMJ laxity (five cases), although maxillofacial trauma (n = 5), mandibular symphyseal laxity (n = 3), changes in occlusion due to tooth extraction/loss (n = 2) and developmental abnormalities (n = 2) have been hypothesised to be contributing factors in other reports.1–9 Breed-specific (Persian and Siamese) skull conformation has also been theorised to be a possible contributing factor.1,2,4
Before the advent of CT, radiography was used to aid in the diagnosis of the condition, but owing to the limitations of this imaging modality, identification of the inciting cause was difficult. Only one of the reported cases suspected to have TMJ dysplasia actually had radiographic changes consistent with the disease, 8 and of the four cats reported to have undergone CT, no abnormalities of the TMJs were found.1,3,4
Manual mandibular replacement and application of a tape muzzle for a few weeks may be tried for single occurrences of open-mouth jaw locking, although we have had no success with this approach. Surgery is recommended for recurrent cases. The surgical procedures described in the literature are summarised in Table 1. Partial zygomectomy has been reported to either involve removal of a partial-width segment or full-width segment of the zygomatic arch.1–3,5–7 Long-term outcomes after surgery were reported to be excellent in all of the published cases and the additional three cases reported herein.1–9 One case had short-term recurrence of open-mouth jaw locking following bilateral partial (full-width) zygomectomy; this occurred several times 5 weeks following discharge, but each episode lasted only for a few seconds and reduced spontaneously. No additional episodes were noted at the 6 month follow-up. 2 Postoperative dental malocclusion was noted in the case that underwent bilateral condylectomy. This cat subsequently underwent reduction of the canine crowns, but there was a persistent shift of the mandible to the right side. However, the owner reported the cat to be content and displaying normal behaviour. 8 In the case which underwent symphysiotomy, symphysiectomy and intermandibular arthrodesis, discomfort during yawning/meowing (as perceived by the owner), and slight pain on opening the mouth on veterinary examination was noted 2 weeks after discharge. The cat had reportedly recovered at the 9 and 33 month follow-up telephone calls. 3 One of our cases showed signs consistent with pain for 7 weeks postoperatively. At the 3 and 10 month telephone call follow-ups the cat was behaving normally, and had displayed no further signs of pain.
Discussion
This report summarises the documented cases of open-mouth jaw locking in cats, and describes three further cases. To our knowledge, two of the additional cases reported here document the first cases of TMJ dysplasia in cats to be definitively diagnosed using CT. Furthermore, bilateral partial zygomectomy with bilateral partial coronoidectomy has not previously been reported as a surgical treatment. All three cases were investigated using CT, and were successfully treated, with no long-term recurrence of open-mouth jaw locking.
Proposed aetiologies of open-mouth jaw locking
TMJ dysplasia
TMJ dysplasia is widely reported to be the causal factor of open-mouth jaw locking in dogs,10–13 and has also been theorised to be the cause in cats.2,5,7,8 Dysplasia may allow a wider range of motion of the TMJs, permitting the displacement of the coronoid process ventrolateral to the zygomatic arch. However, in the reported literature dysplastic changes have only been documented in one cat. 8 This may, in part, be owing to the limitations of radiographic examination of the skull, although of the four previously reported cases for which CT was utilised, none of the cats were found to have identifiable dysplastic changes. This suggests that, in at least a portion of cases, TMJ dysplasia may not be the cause of open-mouth jaw locking. Another explanation may be that osseous dysplastic changes had not yet developed at the time of diagnostic imaging; there was an absence of detectable dental/bone abnormalities in seven of the previously reported cases, and all but one of these were between 1 and 3 years old. The domestic shorthair cat reported here (case 1) had osseous abnormalities of the TMJ. The cat was 5 years old and therefore the changes were consistent with bilateral TMJ dysplasia with the later development of degenerative changes to the bone. However, the third case reported here showed bilateral flattening of both the condyloid process and the mandibular fossa of the zygomatic process of the temporal bone (indicative of TMJ dysplasia), and this cat was only 1 year old.
Symphyseal laxity and vertical mandibular range of motion
It has been suggested that a degree of symphyseal laxity is required for jaw locking to occur.2,3,11 This laxity may be enhanced by dental and skeletal malocclusion due to altered levering forces. 14 Unfortunately, symphyseal laxity was not specifically measured in the cases described here. Vertical mandibular range of motion (vROM) appeared subjectively normal. The normal vROM in cats has been shown to be 62 ± 8 mm (median 63 mm, range 41–84 mm). 15 An abnormally wide vROM could predispose a case to open-mouth jaw locking, as the tip of the coronoid process may extend past the distal aspect of the zygomatic arch, but this hypothesis needs to be further evaluated.
Head trauma
Case 2 did not have any identifiable abnormalities of either TMJ. The only findings were a fracture of the left maxillary canine tooth, and the absence of the left maxillary fourth premolar tooth. Trauma has been implicated as a cause of open-mouth jaw locking.3,6,9 The fractured and absent teeth in this case may have been related to a previous traumatic episode, and therefore one could speculate that this may have contributed to the subsequent jaw locking. History of head trauma was not reported in case 1 and a mild trauma happened to case 3 but after multiple episodes of jaw locking.
Genetics and conformation
In dogs, a genetic component is likely to play a part in the aetiology of open-mouth jaw locking, as chondrodystrophic and brachycephalic breeds are reportedly affected most frequently. 1 Genetics and skull conformation may also play a part in cats, since of the 11 cases reported in the literature and three reported here, nine were of brachycephalic breeds (eight Persians and one Exotic Shorthair), three were Siamese (or Siamese crosses) and only two were domestic shorthair cats.
The mechanism for brachycephalic dog and cat breeds developing open-mouth jaw locking remains elusive. Features of a feline brachycephalic skull include mesioversion of the maxillary canine teeth, maxillary brachygnathism and dorsorotation of the jaws, 16 which results in abnormal dental occlusal relationships, particularly between the canine teeth. It remains speculative as to whether the application of abnormal masticatory forces due to malocclusion can, in fact, have an effect on symphyseal and TMJ laxity, and increase the risk for open-mouth jaw locking. In three of the cases published, symphyseal laxity was identified, and all three cats were Persian.1,3,4 Cases 2 and 3 were brachycephalic, and in the absence of other findings it is possible that symphyseal or TMJ laxity may have been the cause of the jaw locking. The genetic link between Siamese breeds and open-mouth jaw locking is even less clear. The Siamese type skull can be classified as long nosed or dolicocephalic. One case was noted to have a flattened left zygomatic arch on radiographs, thought either to be developmental or as a consequence of trauma. 9 The Siamese ‘type’ case had radiographic confirmation of TMJ dysplasia with degenerative osseous changes, 8 and no abnormalities were found in the third Siamese cat. 4 A proposed mechanism of open-mouth jaw locking in Bassett Hounds (a hypochondroplastic breed with rhizomelic limb shortening but a relatively normal or dolichocephalic skull) is that a greater angle between the axis of rotation of the TMJ and the long axis of the condyloid process causes greater movement of the lateral aspect of the condyle. This may cause stretching of the lateral ligament and joint capsule, which may lead to joint laxity and open-mouth jaw locking as a consequence.9–11 However, a more recent paper found that periarticular new bone formation and narrowing of the joint space develop more frequently at the medial rather than the lateral aspect of the TMJ of dogs, therefore contradicting the assumption that the obliquity of the TMJ results in excessive movement at the lateral aspect of the condylar process. 17 Future studies to objectify the differences in anatomical conformation between varying shape skulls, and the relationship between dental occlusion and mandibular stability, are required to test these hypotheses.
Muscular pathology
In one report pterygoid muscle spasticity was demonstrated using electromyography in a case of open-mouth jaw locking in a human and suspected in three dogs due to the absence of other identifiable causes. 9
Diagnosis and imaging modalities
Radiography was the imaging modality used in the investigation of open-mouth jaw locking in the early case reports. As TMJ disease has been reported to be a potential causal factor of open-mouth jaw locking, oblique lateral radiographic views are required for assessment of the TMJ. 14 However, this is technically demanding. CT is superior to radiography for assessment of the TMJ and to rule out other potential underlying causes, and makes the initial diagnosis of open-mouth jaw locking easier. As well as providing greater detail of the osseous structures, the ability to assess the skull in transverse, sagittal and dorsal planes, and to create three-dimensional reconstructions means that a precise and comprehensive evaluation of the entire skull can be performed. This, in turn, enables a more accurate diagnosis and prognosis, and permits surgical planning.4,14 Cone-beam CT has also been demonstrated to be an effective diagnostic imaging modality for TMJ evaluation in cats. This diagnostic modality uses an X-ray tube-detector system that rotates 360° around the patient's head and acquires images that are analysed by a specific computer program. 18
Surgical management
Surgical options for open-mouth jaw locking include unilateral or bilateral partial coronoidectomy, partial zygomectomy, and a combination of partial coronoidectomy and partial zygomectomy. Regarding zygomectomy, both resection of a full-width segment of the zygomatic arch and removal of a partial width segment have been reported.1–3,5–7,13 Bilateral zygomectomy as a sole treatment has been associated with temporary recurrence postoperatively, 2 whereas recurrence following bilateral coronoidectomy has not so far been reported. Other reported surgical treatments are imbrication-plication of the lateral aspect of the TMJ capsule, maxillom-andibular fixation devices and mandibular condylectomy (in dysplastic patients). Imbrication-plication has not been found to be successful in preventing recurrence. 12 Maxillomandibular fixation devices rely on healing of periarticular soft tissues to prevent recurrence following TMJ luxation or subluxation in traumatic cases, and are likely to be ineffective in cases affected by TMJ dysplasia or symphyseal laxity. 3 Bilateral condylectomy performed in a case of TMJ dysplasia was reported to cause dental malocclusion in one report. 8 Symphysiotomy, symphysiectomy, and intermandibular arthrodesis were successful in one cat with open-mouth jaw locking associated with excessive laxity of the mandibular symphysis. 3
Two of the additional cases reported here underwent bilateral resection of a full-width segment of the zygomatic arch and partial coronoidectomy, whereas case 2 underwent bilateral resection of a partial-width segment of the zygomatic arch and partial coronoidectomy. Previous case reports have described partial coronoidectomy as a sole surgical treatment of open-mouth jaw locking in cats, with no occurrence of postoperative complications.4,9 Regarding case 1, it was necessitated by the owners’ stipulated requirement that the cat only undergo one surgery as finances would not permit further surgery if the condition recurred; a full-thickness partial zygomectomy in addition to the partial coronoidectomy was therefore performed. The decision for case 2 and 3 was influenced intraoperatively; the mandible was repeatedly manipulated during burring and it was found that preventing the coronoid process from engaging with the zygomatic arch was most readily achieved by removing apposing bone from each structure; case 3 required a full-thickness partial zygomectomy, whereas a partial-thickness partial zygomectomy was sufficient for case 2. While none of the cats described here had experienced recurrence of the open-mouth jaw locking at the time of follow-up, case 1 showed signs of discomfort for 7 weeks postoperatively. This may indicate that in some cases the induced bone trauma following full-width partial zygomectomy causes more postoperative pain than partial-width partial zygomectomy, although it is not possible to make definitive conclusions from only one case. Postoperative pain or behavioural changes were not reported in the other published cases that underwent full-width partial zygomectomy, nor were they seen in case 3. Other differentials for the discomfort could have been soft-tissue inflammation or trauma to a branch of the maxillary branch of the trigeminal nerve. Objective pain assessment should be performed in future cases in order to draw more substantiated conclusions relating pain and the type of surgical procedure performed. Postoperative dietary recommendations can include feeding a soft diet and avoiding hard food to minimise postoperative pain; however, these recommendations may not always be necessary unless the patient shows signs consistent with pain when chewing food.
Conclusions
Open-mouth jaw locking is seen in cats with a wide age range (from 1–10 years; mean 4.4 years). Cats with all skull types (brachycephalic, mesaticephalic and dolichocephalic) may be affected, but brachycephalic breeds seem to be over-represented. Trauma, temporomandibular dysplasia and symphyseal laxity may predispose to development of this condition. When available, a CT scan with the jaw locked in place is recommended for diagnosis and surgical planning purposes. While the presence or absence of TMJ dysplasia does not alter the surgical treatment when open-mouth jaw locking due to ventrolateral coronoid displacement is diagnosed, CT permits rapid identification of coronoid displacement and the degree of overlap between the coronoid process and zygomatic arch, and allows evaluation of the skull for other abnormalities, which may necessitate additional procedures; for example, fractures or TMJ luxation.
Coronoidectomy and zygomatic arch resection performed alone or in combination is generally successful at preventing long-term recurrence of this condition. We recommend bilateral coronoidectomy with or without partial zygomectomy for open-mouth jaw locking when the mandible can be manually locked on both sides under anaesthesia. The surgery should be unilateral if locking is only possible on one side, though the owner should be warned of possible future contralateral locking. The decision to perform a partial zygomectomy (and whether to remove a partial- or full-width segment of the bone) should depend on intraoperative findings or the necessity for a single surgery (eg, concurrent patient health concerns regarding anaesthesia or owner requirements).
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.