
Abstract
Objectives
The bronchial lumen to pulmonary artery (BA) ratio is utilized to evaluate pulmonary pathology on CT images. The BA ratio may be unreliable when changes are present in bronchial and pulmonary arteries concurrently. Bronchial lumen to vertebral body (BV) and pulmonary artery to vertebral body (AV) ratios have been established in normal cats and may serve as an alternative. This study aimed to evaluate the BV, AV and BA ratios in cats before and after infection with Dirofilaria immitis, with and without selamectin administration, and to characterize the distribution of disease.
Methods
Archived CT images were reviewed from three groups of cats: D immitis-infected untreated (n = 6); infected pretreated with selamectin (n = 6); and uninfected untreated (n = 5). The BV, AV and BA ratios were calculated for all lung lobes for baseline (D0) and day 240 (D240) postinfection. Ratios and percentage change from baseline were compared between lobes and between groups.
Results
BV and AV ratios were more consistent in identifying abnormalities when disease was present in bronchial and arteries concurrently than BA ratios. Infected untreated cats had significant changes in both BV and AV ratios and percentage change from baseline. Abnormal BV and AV ratios were noted in the infected selamectin group, although less widely distributed.
Conclusions and relevance
The BV and AV ratios more accurately identified bronchial and pulmonary artery abnormalities in D immitis-infected cats. Both bronchial and pulmonary artery changes were present in infected cats, decreasing the diagnostic application of the BA ratio. Pulmonary artery changes were more widely distributed than bronchial changes in the lung. Heartworm-infected cats receiving selamectin had bronchial and pulmonary artery changes but to a lesser extent than untreated heartworm-infected cats. The CT-derived BV and AV ratios are a useful measure to evaluate lung disease of cats.
Introduction
High-resolution CT of the lung is becoming widely utilized to evaluate pulmonary pathology in client-owned dogs and cats. The bronchial lumen to pulmonary artery (BA) ratio has been used as a component of interpreting pulmonary CT images, particularly when bronchiectasis is suspected.1,2 However, when disease exists in both bronchial and pulmonary arteries concurrently, the BA ratio may be less reliable. Although used extensively in human medicine, studies have suggested that changes in the BA ratio should be interpreted carefully as changes in the pulmonary arteries may lead to misdiagnosis.3,4 We previously proposed the use of the bronchial lumen to vertebral body (BV) and pulmonary artery to vertebral body (AV) ratios and published reference intervals (RIs) in normal cats. 5 Evaluation of these ratios in a disease state that affects both the bronchial and pulmonary artery would determine the utility of these ratios.
Dirofilaria immitis infection in cats results in interstitial myofibrocyte proliferation causing restrictive lung pathology and also affects both bronchial and pulmonary arteries. 6 Subtle interstitial lung disease not noted on radiographs was present in some cats pretreated with the preventive selamectin. 6 Application of the BV and AV ratios on CT images of D immitis-infected cats in comparison to the BA ratio would evaluate the utility of these ratios and further elucidate the distribution of disease in heartworm-infected cats.
We hypothesized that evaluation of BV and AV ratios would more reliably detect disease in the bronchi and pulmonary arteries of cats than the BA ratio. Our secondary objective was to utilize the BV and AV ratios to further characterize disease in individual lung lobes in heartworm-infected cats.
Materials and methods
CT images of 12 cats infected with D immitis and five healthy, control cats were acquired from images from a previously published study. 6 Cats were specific pathogen-free female, intact domestic shorthairs and ranged in age from 7–8 months at initiation of the study. The previous study had the approval of the Auburn University Institutional Animal Care and Use Committee, and cats were housed in an Association for Assessment and Accreditation of Laboratory Animal Care-approved facility.
CT images from three populations of cats were reviewed from the previously published study. 6 The first group (n = 6) included cats that were infected with D immitis that had not received preventive (Inf/Un); a second group (n = 6) included cats that were pretreated with selamectin (Revolution; Zoetis) at a label dosage 32 days and again 2 days prior to infection with D immitis (Inf/S); and the final group (n = 5) included cats that were neither infected nor administered the preventive (Control).
Study images from day 0 (D0) and day 240 (D240) postinfection were evaluated. Images were acquired as previously described using a helical single detector row CT unit (CT/i scanner; General Electric).5,7 Briefly, cats were positioned in sternal recumbency for image acquisition. Contiguous, 5 mm collimated transverse images and 1 mm transverse images were acquired of the entire lung field utilizing a detail algorithm both pre- and post-non-ionic intravenous contrast (2 ml/kg [Isovue-370; Bracco Diagnostics]). The anesthetic protocol used has been previously described.5,7 Thoracic CT imaging was performed using a single-breath hold technique where the airway pressure was held at 14 cm of water. 7
Image review was completed on a dedicated image viewing station using a commercially available software package (eFilm 3.3; Merge Healthcare). Measurements were acquired as previously described by a single investigator. 5 Using a bone window (window width [WW] 2500; window level [WL] 480), vertebral body height was measured mid-body at T6. A lung window (WW 1500; WL 600) was used for all bronchial and pulmonary artery measurements, and internal bronchial lumen and pulmonary diameters were measured (Figure 1). Measurements were made at the following locations: right cranial and left cranial (cranial) subsegment at T4–T5, right middle and left cranial (caudal) subsegment at T6–T7, and right and left caudal at T9–T10 intervertebral disc spaces. BV, AV and BA were calculated for the right cranial, right middle, right caudal, left cranial (cranial) subsegment, left cranial (caudal) subsegment and the left caudal lobes.

CT images of bronchial and pulmonary artery lumen measurement in the right caudal lung lobe of (a) an uninfected control group cat and (b) a Dirofilaria immitis-infected cat 240 days post-infection
The BV, AV and BA ratios for each lung lobe were compared with published RIs.5,7 Differences between groups for each ratio for individual lung lobes were evaluated using Kruskal–Wallis one-way ANOVA on Ranks followed by Dunn’s method for pairwise multiple comparison. Percentage change from baseline for each cat was calculated using ratios comparing D0 to D240 for each ratio in each lung lobe. Percentage change from baseline of each ratio was compared between groups on D0 and D240 using Kruskal–Wallis one-way ANOVA on Ranks with pairwise multiple comparison accomplished using Dunn’s method. Statistical analysis was completed using a statistical software package (Sigma Plot 12.0; Systat Software). Statistical significance was set at P ⩽0.05.
Results
Across all lung lobes for the Inf/Un and Inf/S groups, a total of 72 sets of ratios (BV, AV and BA) was calculated. Sixteen sets of measurements revealed BV ratios outside of RIs with a corresponding BA ratio within the published RI. Thirty-seven of the AV ratios that exceeded RIs had a corresponding normal BA ratio. Both the BV and AV ratio on 16 measures at D240 were outside of RIs, but the BA ratio was within the normal RI. The AV ratio was solely increased in the face of a normal BA ratio 21 times. There was agreement 11 times between abnormal BA and either abnormal BV or AV ratios, and there was agreement five times with all ratios within the published RIs.
On D240, significant differences in BV ratios were found in the right cranial (P = 0.037), right middle (P = 0.002) and left cranial (caudal) lobes (P = 0.003) between groups (Figure 2). For the BV ratios, both Inf/Un and Inf/S groups were significantly different from the control group in the right middle lobe and left cranial (caudal) lobes. No statistical difference was found between the Inf/Un and Inf/S groups as there was a large SD in the Inf/S group. Differences between groups were not noted in other lung lobes in regards to the BV ratios. Significant differences in the AV ratios between Inf/Un and control groups were noted in all lung lobes (Figure 3; right cranial, P = 0.004; left cranial [cranial], P = 0.015; right middle, P = 0.002; left cranial [caudal], P = 0.001; right caudal, P = 0.001; left caudal, P = 0.009). A significant difference between the Inf/S and control groups was also noted in the right middle lobe (P = 0.002) with no significant difference noted between the Inf/Un and Inf/S groups. Differences were also noted in the right caudal lobe AV ratios between the Inf/Un and Inf/S groups (P = 0.001) with no difference between the Inf/S and control groups. The BA ratios seen in Figure 4 were significantly different between groups in the right cranial (P = 0.037) and left caudal lobes (P = 0.04). Comparison of BA ratios in all other lobes revealed no significant differences.

Box plot with median for the bronchial to vertebral body (BV) ratios for each lung lobe in three groups of cats: Dirofilaria immitis-infected cats 240 days postinfection (Inf/Un), cats pretreated with selamectin and infected with D immitis 240 days postinfection (Inf/S) and an uninfected control group (Control)
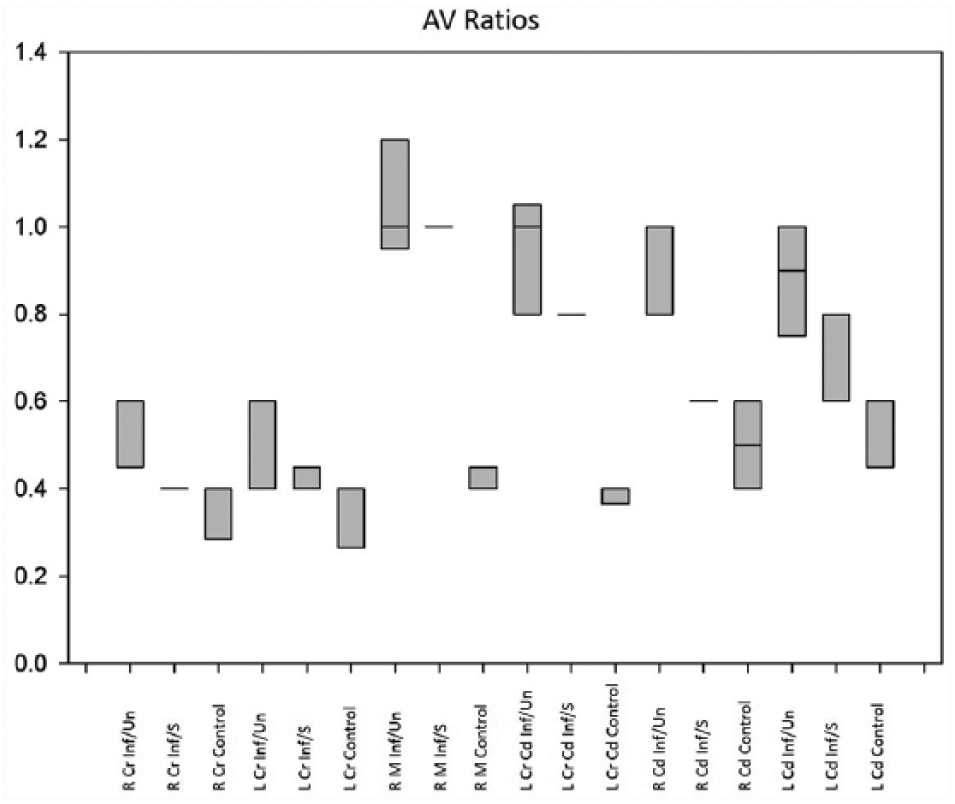
Box plot with median for the pulmonary artery to vertebral body (AV) ratios for each lung lobe in three groups of cats: Dirofilaria immitis-infected cats 240 days postinfection (Inf/Un), cats pretreated with selamectin and infected with D immitis 240 days postinfection (Inf/S) and an uninfected control group (Control)

Box plot with median for the bronchial to pulmonary artery (BA) ratios for each lung lobe in three groups of cats: Dirofilaria immitis-infected cats 240 days postinfection (Inf/Un), cats pretreated with selamectin and infected with D immitis 240 days postinfection (Inf/S) and an uninfected control group (Control)
A significant percentage change from baseline in BV ratio (Figure 5) was noted between Inf/S and control groups in the left cranial (cranial) (P = 0.02) and right middle (P = 0.002) lobes, and a significant percentage change in BV ratio was also noted in the left cranial (caudal) lobe (P = 0.002) between both the Inf/Un and Inf/S group compared with the control group with no difference noted between the Inf/Un and Inf/S groups. No significant differences in percentage change of BV were noted in other lobes. When evaluating percentage change in AV ratios (Figure 6), the Inf/Un group was found to be significantly different from the control group in the right cranial (P = 0.018), right middle (P = 0.002), left cranial (caudal) (P = 0.001), right caudal (P = 0.002) and left caudal (P = 0.021) lobes. Additionally, a significant difference between the Inf/S and controls was found in the right middle lobe (P = 0.002) with their being no difference between the Inf/Un and Inf/S groups. Percentage change in the AV ratio was also noted to be different between the Inf/Un and Inf/S groups in the right caudal (P = 0.002) lobe. No significant difference was seen in the left cranial (cranial) lobe for this measurement. The BA ratio was also evaluated for percentage change from baseline (Figure 7). Significant differences were only found between the Inf/Un and control groups in the right (P = 0.005) and left caudal (P = 0.006) lobes.

Box plot with median for the percentage change from baseline in bronchial to vertebral body (BV) ratios for each lung lobe in three groups of cats: Dirofilaria immitis-infected cats 240 days postinfection (Inf/Un), cats pretreated with selamectin and infected with D immitis 240 days postinfection (Inf/S) and an uninfected control group (Control)
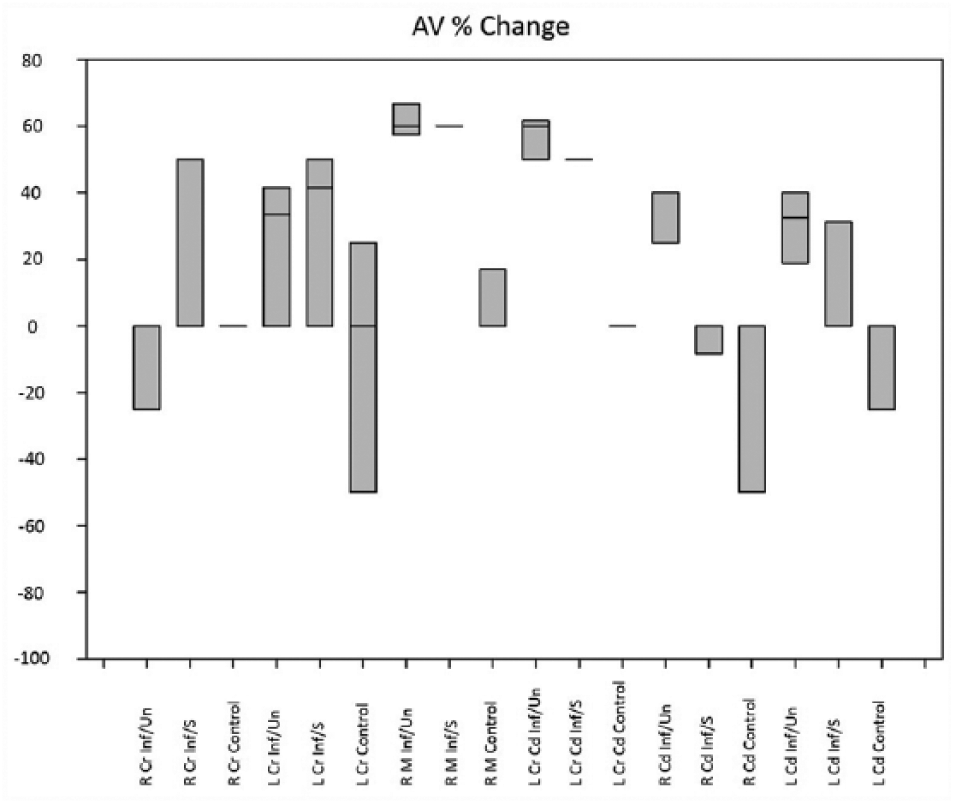
Box plot with median for the percentage change from baseline in pulmonary artery to vertebral body (AV) ratios for each lung lobe in three groups of cats: Dirofilaria immitis-infected cats 240 days post-infection (Inf/Un), cats pretreated with selamectin and infected with D immitis 240 days postinfection (Inf/S) and an uninfected control group (Control)

Box plot with median for the percentage change from baseline in bronchial to pulmonary artery (BA) ratios for each lung lobe in three groups of cats: Dirofilaria immitis-infected cats 240 days postinfection (Inf/Un), cats pretreated with selamectin and infected with D immitis 240 days postinfection (Inf/S) and an uninfected control group (Control)
Discussion
BV and AV ratios were more likely to identify abnormalities in cats infected with D immitis than the BA ratio. The advantage of this measure was evident when abnormalities in pulmonary artery diameter were present or when both the bronchial lumen diameter and the pulmonary artery diameter were concurrently abnormal. Increased bronchial diameter was noted most significantly in the right middle and left cranial (caudal) lobes in cats infected with D immitis, regardless of preventive treatment. Increased pulmonary artery diameter was noted in all lobes in cats in the Inf/Un group, and in the right middle and right caudal lobes, pulmonary artery enlargement was noted in the group receiving preventive treatment. This information is consistent with, but further expands on, previously published findings of evidence of subtle lung disease in D immitis-infected cats pretreated with selamectin which was not evident on routine thoracic radiographs. 6 The uneven distribution in different lung lobes between cats in the infected groups is consistent with previous reports on the uneven pathology linearly in bronchial and pulmonary arteries. 6
The BA ratio has been the standard for evaluation of CT images for the diagnosis of bronchiectasis in human medicine, and it has recently been evaluated in both dogs and cats.2,7,8 In uncomplicated disease where only one aspect of the lung (eg, bronchial or pulmonary arteries) is affected, the BA ratio can be a useful tool. When conditions are present that affect both components of this ratio, its usefulness is diminished as both numerator and denominators become variables. Relying on an increased BA ratio as an indicator of bronchiectasis or to rule out abnormalities can lead to misdiagnoses. A human study of CT measures of bronchiectasis in smokers has indicated the limitations of this evaluation. 3 Although individuals had increased BA ratios suggestive of bronchiectasis, some of the increased ratios were actually related to the changes in pulmonary arteries. 3
We previously published a study of normal cats using BV and AV ratios where the bronchial diameter and pulmonary artery diameter, respectively, are compared with the vertebral body. We have demonstrated that the vertebral body was a stable variable to compare bronchial and pulmonary artery diameter. In the present study, we have demonstrated that the use of the BV and AV ratios is more likely to identify abnormalities in a group of cats with D immitis than the BA ratio, and that in several instances where the BA ratios were considered normal, cats actually had significant changes to both the bronchial and pulmonary arteries.
Heartworm disease in cats is a complex condition, which results in significant lung disease, even in the absence of adult D immitis infection. This condition has been termed heartworm-associated respiratory disease, and it results in restrictive lung disease affecting both the bronchial and pulmonary arteries. 6 The present study builds on previously published CT evaluation of cats with D immitis by applying the BV, AV and BA ratios to these images and further defining location of disease. The prior study applied a subjective scoring system to CT images to characterize disease of the pulmonary arteries, and increased scores were noted in all described lobes with most severely affected lobes being the left caudal, cranial and accessory lobes. 6 In contrast to that study, we chose to describe changes in the subsections of the left cranial lobe separately, and the accessory lobe was not described owing to the inability to consistently obtain a reliable view for accurate bronchial and arterial diameter measurements.
We determined that the pulmonary arteries were significantly affected in the majority of lobes, with the greatest percentage change from baseline in the right middle and caudal subsegment of the left cranial lung lobes. No specific description of bronchial diameter was provided in the previous publication, and through application of the BV ratio to the images, significant disease was seen in cats with D immitis, which corresponded with histological changes previously published. 6 Percentage change from baseline of BV ratio was, again, greatest in the right middle and the caudal subsegment of the left cranial lobes. Results from the current study also supported previous findings that evidence of pulmonary disease was present in cats pretreated with selamectin, although this disease was not as widespread or as severe as was noted in infected, untreated cats. The objective measurements of the bronchial and pulmonary artery diameters and calculation of the ratios allowed for a more detailed description of changes in D immitis-infected cats.
This method of CT evaluation may have broad application to other diseases of the cat lung that affect both the bronchial and pulmonary artery or when concurrent conditions that affect both are present.
Conclusions
The BV and AV ratios are more reliable for detection of abnormalities in the bronchial and pulmonary artery diameter than the BA ratio, particularly in patients with disease affecting both the bronchial and pulmonary arteries. Cats infected with D immitis have significant changes in both the bronchial and pulmonary arteries, with changes being more severe in the pulmonary arteries. The right middle and caudal subsegment of the left cranial lung lobes were more affected than previously described. As has been previously described, cats pretreated with selamectin can develop changes in both the bronchial and pulmonary arteries, although these are not as widespread as is seen in untreated cats.
Footnotes
Conflict of interest
In the past 5 years ARD has received reimbursement, speaking fees or research support from Zoetis, Bayer Animal Health and Elanco, manufacturers of Dirofilaria immitis heartworm preventives; and IDEXX and Zoetis, manufacturers of serologic tests. The other authors have no competing financial interests to disclose.
Funding
The previously published research, which generated the CT images, was funded by Zoetis.