
Abstract
Objectives
The increased demand for animal blood transfusions creates the need for an adequate number of donors. At the same time, a high level of blood safety must be guaranteed and different guidelines (GLs) deal with this topic. The aim of this study was to evaluate the appropriateness of different GLs in preventing transfusion-transmissible infections (TTI) in Italian feline blood donors.
Methods
Blood samples were collected from 31 cats enrolled as blood donors by the owners’ voluntary choice over a period of approximately 1 year. Possible risk factors for TTI were recorded. Based on Italian, European and American GLs, specific TTI, including haemoplasmas, feline leukaemia virus (FeLV), feline immunodeficiency virus (FIV), Anaplasma phagocytophilum, Ehrlichia species, Bartonella species, Babesia species, Theileria species, Cytauxzoon species, Leishmania donovani sensu lato and feline coronavirus (FCoV), were screened. Rapid antigen and serological tests and biomolecular investigations (PCR) were used. Several PCR protocols for haemoplasma and FeLV DNA were compared.
Results
The presence of at least one recognised risk factor for TTI was reported in all cats. Results for FIV and FeLV infections were negative using rapid tests, whereas five (16.1%) cats were positive for FCoV antibodies. Four (12.9%) cats were PCR positive for haemoplasma DNA and one (3.2%) for FeLV provirus, the latter being positive only using the most sensitive PCR protocol applied. Other TTI were not detected using PCR.
Conclusions and relevance
Blood safety increases by combining the recommendations of different GLs. To reduce the risk of TTI, sensitive tests are needed and the choice of the best protocol is a critical step in improving blood safety. The cost and time of the screening procedures may be reduced if appropriate tests are selected. To this end, the GLs should include appropriate recruitment protocols and questionnaire-based risk profiles to identify suitable donors.
Introduction
Recently, the increase in indications for veterinary blood transfusion and its routine use in the veterinary practice caused a rise in the demand for animal donors. A high level of blood safety must be guaranteed to perform this procedure.
Transfusion-transmissible infections (TTI) from apparently healthy and asymptomatic blood donors represent a well-known threat in blood transfusion, in addition to other adverse events.1–4 Therefore, the identification of risk factors and characteristics of ‘low-risk’ blood donors are very important for increasing blood safety. Appropriate recruitment strategies could also reduce infection risks. In human medicine, the World Health Organization identified regular, voluntary, non-remunerated donors as those with the lowest risk for TTI. 5 However, this model cannot be used because different situations and settings exist in veterinary medicine. In cats, different prevalences of microorganisms were found based on the source of the feline donors: a previous study found that laboratory-reared cats and cats housed indoor with no history of flea or tick infestation were ideal blood donors. 6
Moreover, strategies and procedures ensuring blood safety for TTI change in different settings. 7 For humans, it is well known that each country has to address specific issues or constraints that influence the safety of its blood supply, including the incidence and prevalence of TTI, the structure and level of development of blood transfusion services and the economic resources available. 5
There are several guidelines (GLs) for testing protocols in veterinary medicine. GLs are generally developed according to the circumstances and needs of each country. No single set of GLs can ensure absolute blood safety. 5 Both US and European GLs aim to standardise veterinary blood transfusion procedures and to guarantee blood safety.8–10 Additional GLs have been published in Italy to regulate veterinary blood transfusions in dogs, cats and horses.11,12 However, all these GLs differ in some aspects, such as the microorganism to be screened or the screening methods used.8–10
The aims of this research were: (1) to evaluate the differences among existing GLs, and (2) to perform a preliminary investigation on a selected population of feline blood donors from an Italian blood bank, evaluating how blood safety can be improved using tests recommended by the different GLs.
Materials and methods
Comparison of international and national GLs
The main existing GLs for veterinary blood transfusions were compared.8–12 The European and US GLs were written by a panel of experts, according to evidence-based medicine, even if the level of evidence for each topic was not always explicitly declared.8–10 The Italian GLs for animal transfusion was written by a panel of experts commissioned by the Italian Ministry of Health.11,12
Feline blood donor selection
From January 2014 to January 2015 period, blood samples were collected from cats enrolled as blood donors at the Blood Bank of the Veterinary Teaching Hospital of the University of Perugia. Cats were enrolled using the criteria of suitability indicated in the Italian GLs:11,12 body weight ⩾5 kg, age 2–8 years, docile character, regularly vaccinated with core vaccines (feline calicivirus, feline herpesvirus, feline parvovirus) and two non-core vaccines (Chlamydia felis [formerly Chlamydophila felis] and feline leukaemia virus [FeLV]). Blood donors enrolled in cases of life-threatening emergencies, for which the national GLs recommend fast and restricted screening limited to feline immunodeficiency virus (FIV), FeLV and Mycoplasma haemofelis, were excluded from the study.
The owners of cat blood donors were asked for the following information: complete history, blood collection date, type of owner (staff or client), identification of the animal, age, sex, weight, breed, origin (adoption from breed or stray cat or purchase at a pet shop), type of housing (indoor vs outdoor or mixed), cohabitation with other cats, ectoparasite treatment and frequency, coat (long or short hair) and laboratory test results. Travel history was not systematically investigated because it was not initially included in the information required.
For each potential donor, before the collection of blood, a careful physical examination was performed, with particular emphasis on the presence of fleas or ticks, and biological samples were collected by a single operator for clinicopathological screening, consisting of a complete blood count, typing of blood group, serum chemistry, urinalysis and faecal examination.
Blood donation was a voluntary choice by the owners, who signed a written consent form to authorise blood collection and storage and the use of samples and data for scientific purposes. Therefore, based on the current regulations of our institutions, formal approval of the ethical committee was not needed for this study.
Sample collection
A 1 ml sample of blood from each donor was placed into two anticoagulated tubes containing sodium-citrate or EDTA to obtain buffy coat and plasma, respectively. Three millilitres of blood was placed in a plain Vacutainer tube (Becton Dickinson) to obtain serum by centrifugation (1000 g for 10 mins). An aliquot of each sample was stored at −80°C for further investigations.
TTI screening
Serum samples were screened by rapid tests using an ELISA for FeLV antigen and FIV antibodies (SNAP FIV/FeLV Combo test; IDEXX Laboratories) and an immunochromatographic method for feline coronavirus (FCoV) antibodies (FASTest FIP; MegaCor Diagnostik).
For each cat a Romanowsky-stained blood smear was microscopically examined to assess the presence of morphologically detectable microorganisms, with attention given, in particular, to haemoplasmas.
DNA and RNA were extracted from 200 μl of both buffy coat and whole-blood samples according to validated protocols (supplementary material),13–25 using a commercial kit for viral RNA and DNA and bacterial DNA (QIAamp cador Pathogen Mini Kit; Qiagen), in accordance with the manufacturer’s instructions. The concentration and purity of the extracted nucleic acids were quantified using a NanoDrop spectrophotometer (NanoDrop 2000; Thermo Fisher Scientific).
Previously published PCR assays, used for the diagnostic activities in the laboratory that performed the tests, were applied to detect the infectious agents (supplementary material).13–25 Several published PCR protocols were performed in the case of haemoplasmas13–15 and FeLV18–20 to compare the sensitivity of the assays. In this case, 10-fold dilutions of positive samples were used.
A PCR targeting the 18S ribosomal RNA gene was used as internal control to rule out possible PCR inhibitors in the samples.
With regard to FeLV, the PCR product of the expected size was purified with an extraction kit (Qiaquick PCR purification kit; Qiagen) and directly sequenced on both strands with the specific primers previously described, 20 using a DNA analyser (ABI 3730; Applied Biosystems) and capillary sequencer (Bio-Fab Research). The sequences were assembled and aligned using BioEdit software, 26 and sequence similarities were assessed by comparison with the sequences deposited in GenBank using BLAST software. 27
Statistical analysis
A χ2 test, with Yates’s correction, and Fisher’s exact test were used to compare the proportions of positive and negative samples, stratified for the data of the animals at the time of the visit (staff- or client-owner, age, sex, breed, origin, type of housing, cohabitation with other cats, ectoparasite treatment and frequency, kind of coat), as most appropriate. Age was analysed by grouping the animals into age categories testing a cut-off ⩽3 years. A P value <0.05 was considered statistically significant. EpiInfo 28 and OpenEpi 29 were used for analysis.
Results
Comparison of international and national GLs
Different aspects concerning criteria of suitability, selection and TTI screening for blood donors are reported in the GLs.8–12 However, all GLs consider FIV, FeLV and M haemofelis as the minimum essential level of screening (Tables 1 and 2). Based on the epidemiological situation of the individual country,14,30–37 and as suggested by all GLs, Italian GLs were partially integrated with European and US GLs for increasing blood safety. Accordingly, further TTI were investigated: Candidatus Mycoplasma haemominutum, Candidatus Mycoplasma turicensis, Anaplasmataceae family (Anaplasma phagocytophilum and Ehrlichia species), Bartonella species, Babesia species, Theileria species, Cytauxzoon species, Leishmania donovani sensu lato and FCoV. In addition, biomolecular methods were added to the procedures recommended by the Italian GLs. 12
Criteria for donor selection of US, European and Italian guidelines (GLs). Existing previous versions are also reported

This age is indicated to reduce the risk of Bartonella species bacteraemia
Limited screenings are planned: only FIV, FeLV and M haemofelis investigations are considered. FeLV rapid antigen test should be used in this case, and the owner of the recipient should be informed about the higher risk of infectious disease transmission
Based on the judgement of the veterinarian in charge and on the epidemiological conditions. Possibility of testing a pool of samples is considered
Note: storage of whole blood in EDTA causes the detachment of the bacteria from the surface of the red blood cells within a few hours (6 h) and false-negative results could occur 3
NC = not considered; FHV = feline herpesvirus; FPV = feline parvovirus; C felis = Chlamydia felis, formerly Chlamydophila felis; FeLV = feline leukaemia virus; FIV = feline immunodeficiency virus; FIP = feline infectious peritonitis; M haemofelis = Mycoplasma haemofelis
Level of recommendation and corresponding diagnostic test for the main microorganisms responsible for transfusion-transmissible infections (TTI) advised by US, European and Italian guidelines (GLs)
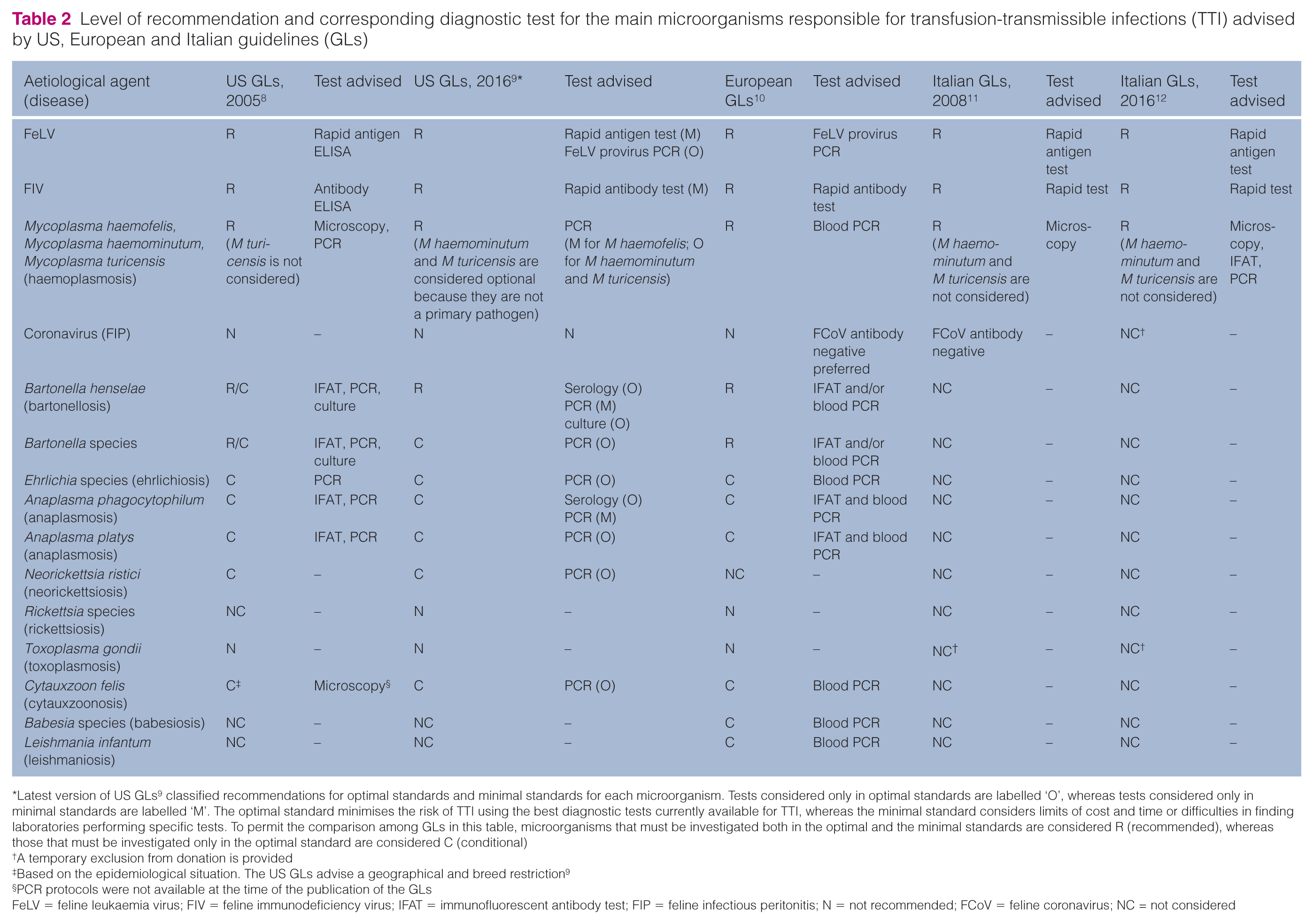
Latest version of US GLs 9 classified recommendations for optimal standards and minimal standards for each microorganism. Tests considered only in optimal standards are labelled ‘O’, whereas tests considered only in minimal standards are labelled ‘M’. The optimal standard minimises the risk of TTI using the best diagnostic tests currently available for TTI, whereas the minimal standard considers limits of cost and time or difficulties in finding laboratories performing specific tests. To permit the comparison among GLs in this table, microorganisms that must be investigated both in the optimal and the minimal standards are considered R (recommended), whereas those that must be investigated only in the optimal standard are considered C (conditional)
A temporary exclusion from donation is provided
Based on the epidemiological situation. The US GLs advise a geographical and breed restriction 9
PCR protocols were not available at the time of the publication of the GLs
FeLV = feline leukaemia virus; FIV = feline immunodeficiency virus; IFAT = immunofluorescent antibody test; FIP = feline infectious peritonitis; N = not recommended; FCoV = feline coronavirus; NC = not considered
Feline blood donor profiles
Thirty-one cats from 18 different owners were included in the study. Six (19.4%) were female (three neutered) and 25 (80.6%) male (15 neutered). Mean age was 4 years (median 5 years, range 2–8 years) and mean weight was 6.23 kg (median 6 kg, range 5–9 kg). Twenty-three (74.2%) were domestic shorthairs, whereas eight (25.8%) were Maine Coon. Twenty cats (64.5%) were client-owned and 11 (35.5%) staff-owned, including students of the veterinary medicine course. Based on the answers received, 22 (71.0%) cats were adopted stray kittens, whereas nine (29.0%) were purebred cats. Thirteen (44.8%) cats lived indoors, whereas 16 (55.2%) had access to the outdoors. Twenty-six (83.8%) lived with other cats. Only two owners performed regular ectoparasite treatments, whereas 25 others (89.3%) administered the treatments mainly in warm periods, and one never administered ectoparasite treatments. Thirteen cats (46.4%) were long-haired and 15 (53.6%) short-haired. In three cases the recording of the answers missed information on the kind of coat and treatment, and in two cases the type of housing.
At least five owners travelled with their cats to different areas of southern-central Italy.
No cats had recent illnesses. Physical examination and clinicopathological screenings were unremarkable, with all the parameters within the standard reference intervals, and cats were considered eligible for blood donation.
TTI screening
All cats were negative using FIV and FeLV rapid tests, whereas five (16.1%) were positive for FCoV antibodies.
Blood smears did not reveal morphologically detectable microorganisms.
Cats were negative using PCR for Anaplasmataceae (Anaplasma species and Ehrlichia species), Bartonella species, Babesia species, Theileria species, Cytauxzoon species, L donovani sensu lato and FCoV, whereas haemoplasma DNA was detected in four cats (12.9%) using all the PCR protocols targeting the 16S rRNA gene.13–15 However, the nested PCR 14 was found to be 10-fold more sensitive than the other PCR protocol used.13,15 Further specific tests16,17 identified three cats as infected with Candidatus Mycoplasma haemominutum and one with M haemofelis. The latter cat was also PCR-positive for FeLV provirus using the specific nested PCR protocol, 19 but not with the other protocols used to detect FeLV DNA.18,20 The specific nested protocol 19 was at least 10-fold more sensitive than the others.18,20 Sequencing of the positive FeLV PCR product shared 98–100% identity with the homologous FeLV region long terminal repeat sequences reported in GenBank (accession numbers AY374218, L25630, M18248, KP728112).
Statistical analysis
No statistical association with positivity to the screened microorganisms and the characteristics of the cats was found.
Discussion
In this study, Italian GLs were applied to 31 feline candidate blood donors enrolled over a 1 year period. According to these GLs, these cats were fully eligible as blood donors. However, based on donor selection criteria or recommendations of other GLs, blood safety could not be completely guaranteed. Indeed, the enrolled cats, although clinically healthy, had risk factors for harbouring TTI and were positive for some microorganisms included in the other GLs.
All 31 cats were negative using rapid tests for FIV and FeLV. One cat was positive for FeLV provirus but only when using the most sensitive PCR protocol. This cat should be excluded from the donation programme, considering that FeLV provirus carriers testing negative for the p27 antigen may transmit FeLV infection to a naïve recipient via blood transfusion. 38 These results show that the Italian GLs would have missed this infected cat because, as opposed to the other GLs,9,10,39 PCR is not recommended for detecting proviral FeLV. Furthermore, the results also raised the issue that the same animal may be classified as eligible or ineligible as a blood donor based on the different PCR assay that is applied.
Blood smears negative for haemoplasmas cannot exclude infection. The sensitivity of microscopic analysis is too low to detect haemoplasmas in chronically asymptomatic cats and does not differentiate the Mycoplasma species.40,41 Using sensitive PCR protocols, as suggested by European and US GLs and previous studies,2,3,8,10 12.9% of cats were positive, with a prevalence comparable with that of previous studies on blood donors.37,40,42 This confirms the endemicity of haemoplasma in clinically healthy cats and the high probability of finding a positive cat even in a limited number of samples.6,40 All the PCR protocols identified the positive cats,13–15 but the nested PCR was 10-fold more sensitive than the other protocols. 14 This protocol should be preferred for its higher sensitivity, as fluctuations in the number of circulating haemoplasmas may lead to false-negative results using less sensitive protocols. 41 For the same reason, screening for TTI should always be performed on the same blood collected for donation: negative results for blood samples collected even a few days before the donation cannot rule out the presence of haemoplasmas in subsequent blood samples used for transfusion because of the fluctuation in bacteraemia. Moreover, considering that the highest risk of haemoplasma transmission by blood was found within 1 week of its collection, 2 and that the risk in feline blood donation was recently defined non-negligible, 37 sensitive PCR tests should be recommended.
M haemofelis, the only species included in the Italian and updated US GLs, was detected in only one cat, whereas three cats were positive for Candidatus Mycoplasma haemominutum. The Italian GLs recommend temporarily excluding cats infected by M haemofelis from the donation programme until PCR results are negative, whereas US GLs exclude them permanently, assuming that these cats may be chronic carriers of Mycoplasma species.41,43 The identification of haemoplasma species is considered optional by the US GLs. 9 However, four haemoplasma species are recognised in cats, and their pathogenic significance is debated;40,41,44 hence, the identification of Mycoplasma species, although time-consuming, may be recommended.
Although not currently recommended by all GLs, the screening of FCoV antibodies using rapid tests, as is required by the Italian GLs, showed a low prevalence of infection (16.1%) vs previous studies in Italian populations.35,45 Furthermore, a specific nested PCR assay demonstrated that blood samples were negative for FCoV. However, the European GLs and a recent study advise that seropositive cats should be excluded from the donor programme because it is possible that passively transferred anti-FCoV antibodies could endanger the recipient, if infected, even if no evident risk of transmission of FCoV via blood has been demonstrated;10,46–49 no reports of transmission following blood transfusion have been described until now and there is no evidence that seropositive cats will develop FIP.9,10 With the current shortage of donor cats, the exclusion of FCoV seropositive cats is likely unnecessary and could cause a relevant reduction in the number of blood donor cats. Moreover, considering that transitory viraemia is possible, even in seronegative cats,45,50 FCoV RNA screening of blood collected for donation could be appropriate.
The comparison of analytical sensitivities of the different protocols was limited to haemoplasmas and FeLV PCR assays. However, this approach would also have been appropriate for the other tests. Therefore, validated and common protocols could be described and advised by GLs in order to guarantee the same level of accuracy in detecting blood donors with TTI everywhere, as is the case for notifiable diseases. 51 As in people, however, test accuracy may be time consuming and expensive. Otherwise, a lower level of risk assessment should be accepted by the owner of the recipient by written consent, such as in the case of emergency transfusions, as is currently indicated by all GLs.9,10,12
Accordingly, additional appropriate strategies for selecting ‘low-risk donors’ should be applied to reduce the cost and time of screenings and to guarantee a high level of blood safety. For example, the use of a questionnaire to identify suitable donors could be an inexpensive and useful tool. As is already the practice in human medicine, recently both US and European GLs provided different questionnaires to determine the risk profile.9,10 However, even if the questionnaire was not available at the time of enrolment in the study, the owners in the current study were asked specific questions and the profiles of the donor candidates showed that they had risk factors for harbouring TTI. All 31 Italian donor cats had at least one TTI-risk characteristic or behaviour, such as access to the outdoors, for which the US GLs specifically recommend repeated testing, 9 or the irregular ectoparasite treatment performed by 89.3% of the owners. All GLs advise regular ectoparasite treatments, but the frequency of treatments is not specified. Monthly ectoparasite prophylaxis was suggested by other studies.3,7 The owners should be encouraged to carry out ectoparasite prophylaxis correctly, considering the relevance of this practice in the control of a wide range of vector-borne diseases. Although travel history was not systematically investigated, at least five owners travelled with their cats to different areas of southern-central Italy; these cats were at risk of some infectious diseases and therefore should be considered at high risk for harbouring TTI.33,34 Unfortunately, the small number of cats in this study limited the statistical power. A higher number of animals could improve the identification of specific risk factors for TTI in Italy.
The possible exclusion of cats with a TTI risk profile from donor programmes contrasts with the difficulty of finding a sufficient number of adequate donors, as is confirmed by the enrolment of only 31 cats in more than 1 year. This makes the rejection of candidate donors very difficult, even if they have a TTI risk profile. Thus, the application of a wide range of sensitive diagnostic tests should be proposed to verify the actual infectious status and to guarantee a sufficient number of adequate donors. US and European GLs recommend that donors with a high risk profile should undergo frequent or extensive TTI screening.9,10
Another possible action for increasing blood safety that is currently not recommended by GLs is a recruitment strategy that can identify populations of low TTI-risk donors. No general recruitment criteria are reported in veterinary medicine, and appropriate surveys should be taken to identify the best strategy. Laboratory-reared cats could be considered the ideal donors, 6 being negative for all the microorganisms, but enrolment of these animals is open to possible ethical issues. 10 A recent survey on hospitals with blood-bank or transfusion services found that staff-owned cats are the donors enrolled most frequently, followed by colonies of feline donors and client-owned cats. 7 These sources of donors probably reflect different infection risks. Considering the central role of the owner in managing health prophylaxis, determining the lifestyle of cats and choosing to donate blood, it is possible that informed and motivated owners could be a key point for safer blood donors that reduces the possible exposure to TTI risk factors.
Conclusions
Since the GLs recommend different protocols and can classify cats differently as eligible or ineligible for blood donation, the harmonisation of recommendations would be advisable. This is especially important for the main TTI and for the choice of the most sensitive screening tests, with possible variations according to local epidemiological situations. These additional recommendations would improve the general level of transfusion blood safety. Screening costs and time may be reduced if appropriate tests are selected. Attention should be paid to identifying donors that were stray cats, with irregular or no ectoparasite treatments, travelling or with outdoor access. The use of biomolecular methods should be recommended, at least in the case of storage in blood banks, to identify proviral FeLV DNA, considering that rapid tests are not definitively discriminatory and haemoplasma DNA may be present in blood collected for donation. Moreover, issues raised by FCoV seropositivity and the possible presence of FCoV RNA in seronegative cats should be further considered.
Finally, appropriate recruitment protocols currently not considered in GLs, educational courses for owners, the possibility of establishing permanent groups of safe blood donors and questionnaire-based risk profiles could improve the identification of suitable donors with a low risk of harbouring TTI, reducing the necessity of performing extensive screening.
Supplemental Material
Click here for Supplementary Material
PCR test protocols used for the detection of transfusion transmissible infections of feline cat donors
Footnotes
Acknowledgements
We thank Mr Carlo Sanesi for his skilful technical assistance.
Supplementary material
PCR test protocols used for the detection of transfusion-transmissible infections of feline donors.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.