
Abstract
Objectives
Flow cytometry (FC) is becoming increasingly popular among veterinary oncologists for the diagnosis of lymphoma or leukaemia. It is accurate, fast and minimally invasive. Several studies of FC have been carried out in canine oncology and applied with great results, whereas there is limited knowledge and use of this technique in feline patients. This is mainly owing to the high prevalence of intra-abdominal lymphomas in this species and the difficulty associated with the diagnostic procedures needed to collect the sample. The purpose of the present study is to investigate whether any pre-analytical factor might affect the quality of suspected feline lymphoma samples for FC analysis.
Methods
Ninety-seven consecutive samples of suspected feline lymphoma were retrospectively selected from the authors’ institution’s FC database. The referring veterinarians were contacted and interviewed about several different variables, including signalment, appearance of the lesion, features of the sampling procedure and the experience of veterinarians performing the sampling. Statistical analyses were performed to assess the possible influence of these variables on the cellularity of the samples and the likelihood of it being finally processed for FC.
Results
Sample cellularity is a major factor in the likelihood of the sample being processed. Moreover, sample cellularity was significantly influenced by the needle size, with 21 G needles providing the highest cellularity. Notably, the sample cellularity and the likelihood of being processed did not vary between peripheral and intra-abdominal lesions. Approximately half of the cats required pharmacological restraint. Side effects were reported in one case only (transient swelling after peripheral lymph node sampling).
Conclusions and relevance
FC can be safely applied to cases of suspected feline lymphomas, including intra-abdominal lesions. A 21 G needle should be preferred for sampling. This study provides the basis for the increased use of this minimally invasive, fast and cost-effective technique in feline medicine.
Introduction
Lymphoproliferative malignancies are fairly common in dogs and cats. 1 In canine species, the diagnosis of lymphoma and leukaemia is nowadays easy, fast and minimally invasive thanks to useful tools like flow cytometry (FC). 2 FC is widely used in canine oncology, not only for the determination of neoplastic cell lineage, but also because of the increasing number of available leukocyte markers, which strengthens the chance of recognising different lymphoma subtypes.3,4 Moreover, in dogs FC allows assessment of the stage of the tumour or the minimal residual disease after treatment.5,6
In cats, the prevalence of lymphoma is believed to be high: in the 1970s and 1980s one third of feline neoplasms were estimated to be of haematopoietic origin, either lymphoid or myeloid, in association with a high prevalence of feline leukaemia virus (FeLV) infections. Since the late 1980s the situation has changed: the prevalence of FeLV-positive cats and associated forms of haematopoietic tumours decreased thanks to efficient diagnostic tests, vaccination and isolation of infected cats, whereas the number of non-FeLV-related forms of lymphoid tumours increased (mostly alimentary and cutaneous forms). 7
Cytology of suspected feline lymphomas is often heterogeneous and thus generally not conclusive for neoplasia. Histopathology and immunohistochemistry remain the gold standard for the diagnosis and immunophenotyping of feline lymphoma, 8 but these techniques are invasive, as they require a biopsy specimen, and are time-expensive, as some days are needed for results.
FC could overcome these limits, although only a single study has been published so far on this topic. 9 In spite of the high prevalence of lymphoma in cats, the application of FC for the diagnosis and characterisation of this tumour in feline species is still limited and considered challenging for several possible reasons. 10 First, because of the high prevalence of intra-abdominal forms, which are anecdotally reported to yield poor-quality samples because of sampling difficulties. Second, the availability of species-specific monoclonal antibodies (mAbs) binding to feline leukocyte differentiation antigens is restricted for FC application and only a few studies have been conducted for evaluation of cross-reactivity with monoclonal antibodies of other species.11,12
The general thought concerning the difficulty of obtaining good-quality samples from abdominal lesions in cats is unsubstantiated, and has never been documented (nor contradicted) in the scientific literature. Going the long way round, to our knowledge, there are no published studies concerning the quality of samples for FC analysis of feline lymphomas.
The aim of the present study was to evaluate if and which specific pre-analytical factor could affect the quality of feline lymphoma samples for FC and, as a consequence, the likelihood of being processed. Factors taken into account concerned both sampling and processing procedures. This might be an important assessment in order to provide useful indications for a good-quality sampling for FC in cats with suspected lymphomas.
The use of FC may improve the diagnosis and classification of feline lymphomas, raising it to the levels achieved in the dog. However, the assessment of the diagnostic accuracy of FC for feline lymphomas does not fall within the aims of the present study, as it has already been described in the literature. 9
Materials and methods
The database of the FC service of our institution (from January 2009 to February 2016) was interrogated and feline cases were extracted. Inclusion criteria were: (1) cases sent to the laboratory for suspected lymphoma; and (2) a request for FC immunophenotyping of the primary lesion, including effusions. Cases were excluded from the study if only peripheral blood and/or bone marrow samples had been sent to the laboratory.
For each case, data concerning the subject, the lesion, the sampling technique and the ancillary tests performed, as well as data concerning the clinician who collected the sample, were requested from the referring veterinarian, if not provided at the time of sample submission (Table 1). As no objective parameters exist to assess and quantify veterinarians’ clinical experience, this was evaluated with two parameters set for this study: the timespan between the veterinarians acquiring their licence and the sample collection (ie, years of expertise) and the presence of any postgraduate specialisation, irrespective of the type of specialisation and its specific field of application (whether clinical or not). If samples from multiple sites were available for a single animal, the data were recorded for each sample independently. Additional data were retrieved from the FC database (Table 1).
Pre-analytical data asked of the referring veterinarians or reported in the laboratory records for 97 samples of suspected feline lymphoma, sent to the laboratory for flow cytometry immunophenotyping

Italics indicate that the variable was included in the statistical analyses
FIV = feline immunodeficiency virus; FeLV = feline leukaemia virus
All FC data were reviewed by a single operator (VM) who was aware of the cytological diagnosis (when available) but was blinded to the previous FC report and to all other tests performed on the lesion.
Flow cytometry
FC was performed on tissue aspirates collected in a liquid medium (either saline solution or RPMI 1640) or on effusions collected in EDTA tubes with an adaptation of a previously published procedure. 9
Prior to labelling, all samples were counted via an automated haematology analyser (Sysmex XT-2000iV) to assess cellularity. Also, a visual inspection of the sample was made by the operator, to assess both the total volume of the sample and the presence of artefacts such as gross haemocontamination, clots, necrotic material or any other abnormality. Based on all these parameters, the operator dealing with each sample decided whether to admit it to FC or not, based on his/her subjective opinion and experience.
The antibody panel varied among samples; indeed, for samples processed between January 2009 and December 2010, a single-colour approach was used with the inclusion of a fluorescein isothiocyanate (FITC)-conjugated secondary antibody (rabbit anti-mouse IgG-FITC, polyclonal; Serotec), whereas a multi-colour approach was used for samples processed between January 2011 and February 2016 (CD5-FITC/CD21-phycoerythrin [PE]/CD18-AlexaFluor647; CD4-FITC/CD8-PE/CD18-AlexaFluor647). Antibody clones and source are listed in Table 2.
Antibodies used for flow cytometric analysis of suspected feline lymphoma samples

PE = phycoerythrin; FITC = fluorescein isothiocyanate
All samples were acquired with a FACScalibur flow cytometer (Becton Dickinson) and analysed with a specific software (CellQuest; Becton Dickinson).
Statistical analysis
Statistical analyses were performed to assess whether the cellularity of FC samples and the likelihood of samples to be finally processed for FC were influenced by any pre-analytical variable (Table 1).
To this end, continuous variables were arbitrarily categorised as follows: age of cat (⩽1 or >1 year); years of experience of the vet (ie, timespan between veterinarian licence acquisition and sample collection, <15 or ⩾15 years). The lesions were classified into five groups based on their site: peripheral lymph nodes (pLN), abdominal lymph nodes or masses (aLN), thoracic lymph nodes or masses (tLN), effusions (grouped altogether irrespective of their primary location, either thoracic or abdominal) and any other site.
Contingency tables were prepared for each of the investigated variables, and the Pearson χ2 test was performed to assess their possible association with the likelihood of samples to be processed for FC.
The Shapiro–Wilk test was performed to assess whether the FC samples cellularity was normally distributed. Then, Student’s t-test, Mann–Whitney test, ANOVA or Kruskal–Wallis test were performed to compare the mean sample cellularity among different categories, based on the data distribution (normal or not) and the number of groups (⩾2). The Kruskal–Wallis test was also performed to compare the mean cellularity among samples with different FC diagnosis (conclusive for lymphoma, negative for lymphoma, not conclusive): this analysis was restricted to samples finally processed for FC. When significant results were obtained, appropriate post-hoc tests were performed based on data distribution and homoscedasticity assessment (Mann–Whitney, Bonferroni or Dunnett test).
Initially, all samples were included in the analyses. Thereafter, samples were investigated according to the five lesion site groups.
All analyses were performed with SPSS v20.0 for Windows (IBM). Significance was set at P ⩽0.05 for all tests.
Results
In total, 105 consecutive suspected lymphoma samples were retrospectively extracted from the FC service’s database of DIVETLAB (Department of Veterinary Medicine, University of Milan). Eight were then excluded from the study for different reasons: three were delivered to the laboratory 48 h after sampling, three were sampled after the administration of chemotherapy, and in two cases the sampling was repeated twice because the first one had a low cellular concentration and had not been processed. In these two cases, only the first (poorly cellular) sample was included in the study. Thus, 97 samples were finally included in the present study, from 86 different feline patients: 73 (75.3%) of these samples were analysed for FC, while the remaining 24 (24.7%) were discarded by the operator. Thirty-one (32%) samples were collected before 2011 and were analysed with a single-colour approach while 66 (68%) samples were collected subsequently and analysed with a multi-colour approach. The proportion of samples finally processed for FC did not vary with year of sampling, nor with the FC approach used.
Total nucleated cell count (TNCC) was reported for 91 samples, with a mean of 12.96 ± 21.19 × 103 cells/µl (median 3.11 × 103 cells/µl; minimum–maximum 0.01–89.88 × 103 cells/µl). In particular, it was significantly higher in samples eventually processed for FC (mean 14.78 ± 22.12 × 103 cells/µl; median 4.09 × 103 cells/µl; minimum–maximum 0.16–89.88 × 103 cells/µl) than in discarded samples (mean 7.26 ± 17.20 × 103 cells/µl; median 0.54 × 103 cells/µl; minimum–maximum: 0.01–58.02 × 103 cells/µl; P = 0.000). None of the remaining variables significantly influenced the likelihood of samples being finally processed for FC.
In turn, TNCC was significantly influenced by the size of the needle and by the presence of postgraduate specialisation of the veterinarian performing the sampling. The 21 G needle gave the most cellular samples, with a statistically significant difference from the other needles (P = 0.045). The needle sizes with relative average cellular concentration are listed in Table 3. Of 37 samples for which this information was available, 33 (89.2%) were collected by veterinarians with postgraduate qualifications: veterinarians with postgraduate qualifications collected samples with an average cellular concentration of 9.42 ± 19.86 × 103 cells/µl (median 1.71 × 103 cells/µl; minimum–maximum 0.01–87.54 × 103 cells/µl), whereas other first-opinion veterinarians collected samples with an average cellular concentration of 33.16 ± 29.5 × 103 cells/µl (median 34.01 × 103 cells/µl; minimum–maximum 5.35–59.26 × 103 cells/µl). The difference was statistically significant (P = 0.027).
Cellular concentration of 52 samples of suspected feline lymphoma sent to the laboratory for flow cytometric immunophenotyping, according to the size of the needle used for sampling
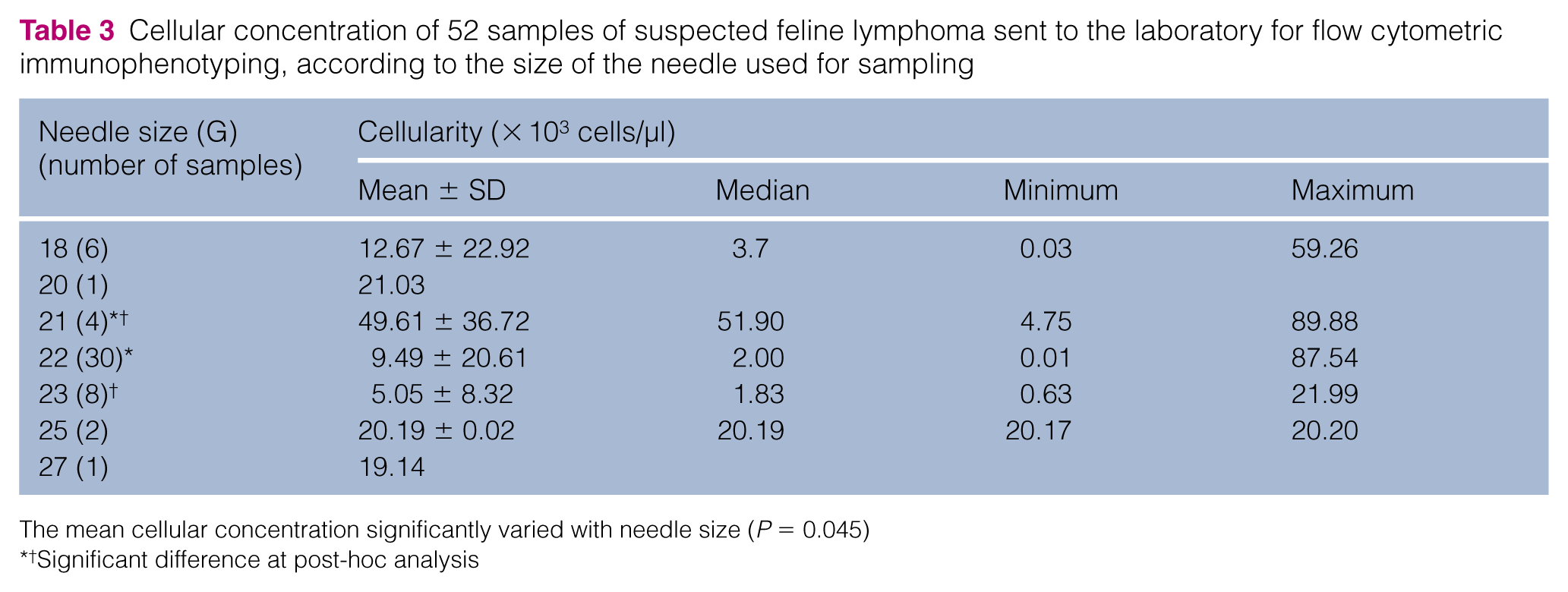
The mean cellular concentration significantly varied with needle size (P = 0.045)
†Significant difference at post-hoc analysis
None of the other variables (including lesion site and size) gave significant results. Raw results are listed below.
Breed was known for 75 cats: 64 (85.3%) were domestic shorthair, four (5.3%) were Maine Coon, two (2.7%) were British Shorthair, two (2.7%) were Chartreux, two (2.7%) were Persian and one (1.3%) was a Norwegian Forest Cat. Sex was known for 81 cats: 18 (22.2%) were intact females, 21 (25.9%) were neutered females, nine (11.1%) were intact males and 33 (40.7%) were neutered males. Age was known for 85 cats, which were aged from 5 months to 16 years, with a median age of 8 years. Feline immunodeficiency virus (FIV)/FeLV status was known only for 16 patients: seven (43.8%) were negative for both, seven (43.8%) were FeLV positive and two (12.5%) were FIV positive.
The site of the lesion was known for all 97 samples: 24 (24.7%) were pLN, 21 (21.6%) were aLN, 21 (21.6%) were tLN, 17 (17.5%) were effusions and 14 (14.4%) were located elsewhere, including skin, kidney, spleen, liver and urine. Lesion size was known for 49 samples: 13 (26.5%) were <2 cm, 22 (44.9%) were between 2 and 5 cm and 14 (28.6%) measured >5 cm.
Concerning cytology, 67 samples were received with a cytological report. Of these, 30 (44.8%) were conclusive for lymphoma, for 16 (23.9%) lymphoma was suspected with different confidence levels (diagnostic but not conclusive), for nine (13.4%) lymphoma was excluded, one (1.5%) was diagnostic for thymoma (for a total of 10 lymphoma-negative samples) and 11 (16.4%) were considered non-diagnostic because of poor cellular concentration, high haemodilution or poor quality of the preparation.
The method of sampling for FC was known for 66 samples: 16 (24.2%) were made by blind aspiration, 41 (62.1%) were ultrasound-guided, seven (10.6%) were CT-guided, one (1.5%) was obtained by surgical access and one (1.5%) by urethral catheterisation. Patient waking condition was known for 53 samples: 24 (45.3%) were awake, 17 (32.1%) needed mild sedation and 12 (22.6%) needed general anaesthesia.
Of the 44 cats for which this information was available, side effects of sampling were reported in one case only: this cat showed a transient mild swelling in the sampling region (submandibular lymph node).
Transport medium was known for 58 aspirates: six (10.3%) were collected in saline solution and 52 (89.7%) were collected in culture medium (RPMI or DMEM). All effusions were collected in EDTA tubes.
Concerning the experience of the clinician performing the sampling, the time span between graduation and sample collection was <15 years for 25 (46.3%) samples and >15 years for 29 (53.7%) samples.
As a second step, the statistical analyses were performed including samples according to the five different lesion sites (pLN, aLN, tLN, effusions and other sites). Results are reported in the supplementary material (Tables S1–S10). Significant differences were noted only within the tLN group: clinicians without postgraduate qualifications collected samples with a higher cellularity (P = 0.036).
Finally, cellular concentration was evaluated according to the FC diagnosis. TNCC was not recorded for four samples. The remaining 69 processed samples were divided in three categories: positive for lymphoma, negative for lymphoma and non-diagnostic. TNCC varied significantly among the three groups (P = 0.022; Table 4): in particular, non-diagnostic samples were less cellular than lymphoma and non-lymphoma samples (P = 0.009 and P = 0.040, respectively). The difference in TNCC according to FC diagnosis also remained significant within the pLN and effusion groups (P = 0.029 for both): the significant difference was between lymphoma and non-diagnostic samples for both groups (P = 0.016 for pLN and P = 0.036 for effusions). TNCC values are shown in Tables 5 and 6.
Cellular concentration of 69 samples of suspected feline lymphoma sent to the laboratory for flow cytometric immunophenotyping, according to the flow cytometric diagnosis
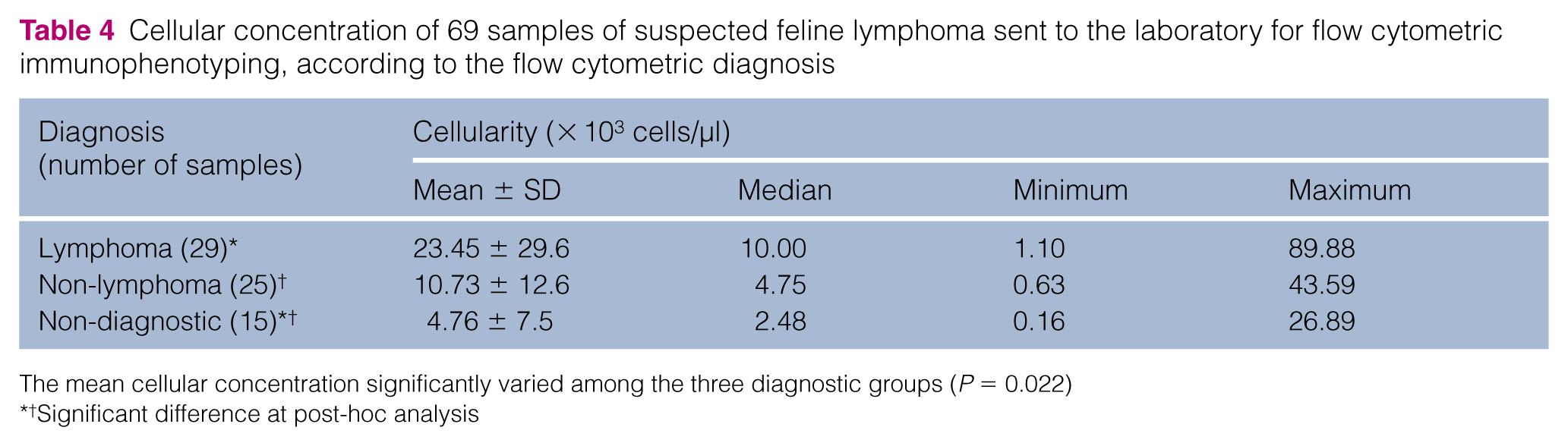
The mean cellular concentration significantly varied among the three diagnostic groups (P = 0.022)
†Significant difference at post-hoc analysis
Cellular concentration of 21 feline peripheral lymph node aspirates sent to the laboratory for flow cytometric immunophenotyping for suspected lymphoma, according to the flow cytometric diagnosis

The mean cellular concentration significantly varied among the three diagnostic groups (P = 0.029)
Significant difference at post-hoc analysis
Cellular concentration of 11 feline effusions sent to the laboratory for flow cytometric immunophenotyping for suspected lymphoma, according to the flow cytometric diagnosis

The mean cellular concentration significantly varied among the three diagnostic groups (P = 0.029)
Significant difference at post-hoc analysis
Discussion
FC is widely used in human medicine and its use in veterinary medicine has been increasing in recent years, especially for canine lymphoproliferative diseases. In canine species, this diagnostic tool turned out to be very helpful for a rapid and non-invasive lymphoma diagnosis. 2 Moreover, some studies have been published in recent years about the prognostic value of the flow cytometric immunophenotype in this species.5,13,14
Nevertheless, in feline species, FC is not commonly used; to our knowledge, it had not been described until last year, when Guzera et al published the first scientific study about the application of FC in the diagnosis of feline lymphoma, highlighting the diagnostic accuracy of this technique. 9
As most feline lymphomas are localised in the intra-abdominal region, reaching the primary lesion with a needle might be difficult for the clinician, and mild or general anaesthesia may be necessary. Based on this general thought, FC is not usually included in the diagnostic work-up for suspected feline lymphomas. The lack of confidence in this technique is confirmed by the fact that feline samples represent only about 2% of the samples included in our FC database in the past 7 years (2009–2016).
The study published by Guzera et al, 9 and the present study, dispute this common belief, because a high number of samples in both studies were likely to be processed and to be diagnostic. In the present study, 75% of samples were finally processed for FC; of these, only 20% were non-diagnostic and they had a lower cellular concentration than the diagnostic samples. In our laboratory, samples are usually admitted to be processed for FC only if they are suitable to be analysed with the whole antibody panel, irrespective of the FC approach used (single- vs multi-colour). The percentage of processed samples in the study by Guzera et al was slightly higher, 9 but only a limited antibody panel was applied to a subset of samples, which may explain this discrepancy between the two studies. Summarising the results of the two studies, we can state that 75–85% of feline samples are suitable for FC analysis. Samples with a low cellular concentration could still be investigated through a more limited panel of antibodies, although they are less likely to be of diagnostic usefulness.
Based on our results, cellular concentration is a key point in the discrimination between samples suitable or not for FC. Still, some poorly cellular samples were admitted to processing and, vice versa, some highly cellular samples were not. The choice of whether to process the samples or not was left to the operator dealing with the sample, and was likely also based on other features, resulting from the visual inspection of the sample, together with the TNCC. Unfortunately, these data were not reported in the FC records and their influence on TNCC and on the likelihood of samples of being processed could not be evaluated in the present study. Still, gross inspection of the specimen is recommended before admission to processing for FC.
In our case series, similar numbers of pLN, aLN and tLN were present, in spite of the higher prevalence of alimentary lymphoma reported in cats.15,16 One possible explanation for this discrepancy is the presence of many non-lymphoma cases. Another possible reason is that clinicians prefer not to sample hardly reachable lesions such as gastrointestinal lesions, spleen, liver or aLN, owing to a supposed poor quality of the sample. Still, our data support the application of FC even for intra-abdominal lesions, as these had the same likelihood of being finally processed for FC as aspirates taken from peripheral lymph nodes (which are expected to be more comfortably reached).
Although sedation or anaesthesia of the cat may be of aid to the clinician during specimen collection, these did not ensure higher-quality samples. Thus, they are not essential and the choice whether to use them or not should only be based on the cat’s character. The possible occurrence of side effects might also worry the operator. However, for the cases included in the present study, no side effects were reported following intrathoracic/abdominal fine-needle aspiration (FNA), but just one patient had a transient swelling after FNA of a pLN.
Among all the factors we evaluated, only two significantly affected the cellular concentration of samples: the size of the needle and the postgraduate qualification of the clinician.
The results showed that a 21 G needle, a medium-sized needle, is related to a higher cellular concentration of the sample. On one hand, smaller needles could damage the cells, that are more fragile owing to their neoplastic origin, and necrotic or clotted material or connective tissue could plug the needle. On the other hand, larger needles could be more traumatic to the tissue, producing bleeding and thus contamination of the sample with too much blood and other surrounding tissues (necrosis, connective, fat). Also, the small number of samples collected with different needle sizes may have influenced the statistical results. Still, following these results, the advice is to use a 21 G needle to obtain good-quality samples.
The fact that fewer cellular samples came from theoretically more qualified veterinarians is surprising: the most probable explanation for this result is a statistical artefact due to few samples coming from operators without postgraduate qualifications. 4 Most of these clinicians regularly send canine samples to our FC service, so they have a steady practical experience in sampling for this purpose. Otherwise, new, inexperienced operators may have to ask the FC service’s staff for instructions about sampling, transport, medium and sample storage prior to sampling. However, this result is of questionable value and should be better addressed by future studies.
One of the most important results from the present study is that the likelihood of processing the sample and the cellular concentration are not affected by size and site of the lesion, unlike what has been previously thought. This makes FC appropriate for application in feline species, even if lesions are intra-abdominal or thoracic.
In our case series, less than a half of the cytological preparations were conclusive for lymphoma: despite this poor diagnostic value of cytology alone for the diagnosis of feline lymphomas, this test remains a mandatory first step in the diagnostic work-up. In addition, a subset of samples in the present study suspicious for lymphoma, even in the face of a negative cytological report, was sent to our laboratory. Although the referring veterinarians have provided no clear explanation for this phenomenon, it may be considered proof of the scarce confidence of clinicians towards negative cytological reports, when a strong suspicion of neoplasia is present based on clinical signs and imaging. The diagnostic performances of cytology alone and cytology plus FC are still to be elucidated in a clinical set-up.
This is only the second paper published concerning FC as a diagnostic tool for feline lymphoma patients. Clinicians are only slightly familiar with this technique and there is the need to enhance their confidence, based on its promising large spread in the human and canine species. Thus, we support the contemporary sampling for FC and histopathology/immunohistochemistry in cases of suspected feline lymphomas: this would provide a rapid report (within 24 h) from FC and subsequent confirmation and more detailed classification from histology/immunohistochemistry.
The retrospective formulation of the present study is its main limitation: information collected was often incomplete and there was no standard sampling procedure. Confirmation will be necessary in the future, through prospective sample collection and a complete submission of the case. Another main limitation of the present study is the lack of a confirmatory test, as histology was available only for few cases (data not shown) and PCR for antigen receptor rearrangement (PARR) for none. This prevented us from assessing the diagnostic accuracy of FC for feline lymphomas; however, Guzera et al already evaluated this in their study, though on a small sample. 9
Conclusions
The results of the present study show how FC can be used for immunophenotyping in feline lymphomas, regardless of the site and the size of the lesion sampled. The use of 21 G needles may enhance the probability of obtaining highly cellular samples. This was a pilot study aimed at making FC more widely known in the feline medicine world, and future studies are necessary to make this tool as useful as it currently is in dogs, from both a diagnostic and a prognostic point of view.
Supplemental Material
Click here for Supplementary Tables S1–S10
Results obtained from the analyses within lesion-site groups
Footnotes
Supplementary material
Results obtained from the analyses within lesion-site groups are available as supplementary material (Tables S1–S10).
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.