
Abstract
Objectives:
The objective of this study was to quantify complications associated with external skeletal fixators (ESFs) in cats and to identify potential risk factors.
Methods:
A retrospective review of medical records and radiographs following ESF placement was performed.
Results:
Case records of 140 cats were reviewed; fixator-associated complications (FACs) occurred in 19% of cats. The region of ESF placement was significantly associated with complication development. Complications developed most frequently in the femur (50%), tarsus (35%) and radius/ulna (33%). Superficial pin tract infection (SPTI) and implant failure accounted for 45% and 41% of all FACs, respectively. SPTI occurred more frequently in the femur, humerus and tibia, with implant failure more frequent in the tarsus. No association between breed, age, sex, weight, fracture type (open vs closed), ESF classification, number of pins per bone segment, degree of fracture load sharing, and the incidence or type of FAC was identified. No association between region of placement, breed, age, sex, weight, fracture type (open vs closed), ESF classification, number of pins per bone segment, fracture load sharing and the time to complication development was identified.
Conclusions and relevance:
Complication development is not uncommon in cats following ESF placement. The higher complication rate in the femur, tarsus and radius/ulna should be considered when reviewing options for fracture management. However, cats appear to have a lower rate of pin tract infections than dogs.
Introduction
External skeletal fixators (ESFs) are used in a number of situations in orthopaedic surgery, including fracture stabilisation, joint immobilisation, and angular limb deformity and shear injury management. ESFs may be either a sole fixation device or used as adjunctive stabilisation, and are available in a variety of configurations including linear, circular, hinged, free form and hybrid forms.1–4 While ESFs remain a versatile and useful tool in orthopaedics, reservations regarding their use are based on high reported rates of fixator-associated complications (FACs), particularly pin tract infection (PTI) and implant failure.5–8
PTIs occur most commonly when there has been significant penetration of and disruption to the adjacent soft tissues. This allows bacterial contamination of the skin–pin interface, leading to superficial pin tract infection (SPTI), which can progress to deep pin tract infection (DPTI) with associated bone lysis and osteomyelitis.9–11 Implant failures include pin loosening, breakage or bending; clamp loosening; and connecting bar breakage. FAC rates in dogs of up to 100% have previously been reported;8,12 more recent studies in cats have reported lower complication rates, ranging from 26–65%.4,5,13,14
While individual studies have evaluated different ESF types at specific anatomical locations in defined groups of animals, it remains difficult to compare overall ESF complication rates. To the authors’ knowledge, there has been no comprehensive overview of complications arising from ESFs placed for feline orthopaedic conditions. The aim of this study was to review postoperative complications attributable to the ESF in cats, and to identify factors associated with complication development in a large number of clinical cases.
Materials and methods
Medical records of cats presenting to the Royal Veterinary College, with an ESF placed between January 2007 and March 2014, were reviewed. To be included in the study, clinical records needed to be present to the point of frame removal and/or fracture union. The following information was gathered for each patient where possible: signalment, ESF configuration, anatomical region, fracture type (open or closed), number of pins placed per bone segment (appendicular skeleton only) and FACs. ESF configuration was determined from clinical records and radiographs, and categorised into four groups: linear, free form, hybrid and circular. Long bone fracture load sharing was assessed as being load sharing, partial load sharing or non-load sharing, as previously described. 15 Additional ESF frame features were also assessed (see box). Each ESF was assigned to one of 10 anatomical regions (Figure 1).

Anatomical distribution of fixator placement
Categories of FACs
FACs were divided into the following four categories:
SPTIs were diagnosed by the presence of one or more of: (a) purulent discharge (with or without positive bacterial culture); (b) a positive culture result; or (c) at least one sign of infection (pain or tenderness, localised swelling, redness or heat) or a positive response to antimicrobial therapy. 16 DPTIs were diagnosed when these same criteria were met and, in addition, evidence of osteomyelitis or bone sequestrum was seen radiographically.

Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 23.0. Data were assessed for normality using the Shapiro–Wilk test. Categorical variables were analysed using χ2 or Fisher’s exact test, as appropriate. For evaluation of regional association with complication development and type, regions with fewer than six cases were excluded from analysis. Analysis of associations between age, weight and development of complications; fracture type (open vs closed); and time to complication development were assessed using the Mann–Whitney U-test. The Kruskal–Wallis test was used to identify associations between patient age, weight and type of complication, and associations between sex, ESF configuration, pin number, load sharing, fracture type (open vs closed) and region of placement with the time to complication development. Relationships between age, weight and time to complication were assessed by Spearman’s rank correlation. P <0.05 was considered significant.
Results
A total of 140 cats that had been managed with an ESF met the inclusion criteria. Age on presentation ranged from 3 months to 12 years (median 2 years). Body weight ranged from 1.2–8.6 kg (median 4.2 kg). Fifty cats were female (41 neutered) and 90 were male (80 neutered). Seventeen breeds of cat were represented, the most common being domestic shorthair (n = 101), followed by domestic longhair (n = 10) and Siamese (n = 7). Of the 140 cats, 74% (n = 104) had closed fractures and 26% (n = 36) had open fractures. Overall, the most common region of ESF placement was the tibia (24%, n = 34), as shown in Figure 1.
It was possible to identify the specific ESF configuration in 109/140 cats. The majority of ESFs (88%, n = 96 cats) were linear, of which 67% (n = 64) were type I, 31% (n = 30) type II and 2% (n = 2) type III. The remaining fixators were free form (9%; n = 10 cats) and hybrid (3%; n = 3 cats). The majority of constructs used clamps (86%, n = 94), with the remaining 14% (n = 15) using epoxy putty. The number of bicortical transfixing pins placed was identified in 94 cats; the total number of pins placed ranged from 2–9 (mean 6), with 1–4 (mean 3) in the proximal segment and 1–6 (mean 3) in the distal segment.
Additional ESF configuration results are summarised in Table 1.
Association between additional ESF frame features and FACs

FAC = fixator-associated complication; ESF = external skeletal fixator; IM = intramedullary
P <0.05
FACs occurred in 19% of cats (n = 27). Two cats each had two FACs over time, which were treated as separate complications, giving 29 distinct FACs in total. The time to diagnosis of complications ranged from 10–154 days postoperatively (median 43 days). Figure 2 shows the overall frequency and type of FACs that developed; the most common was SPTI, accounting for 45% of all complications seen (n = 13), followed by implant failure (41%, n = 12).

Distribution of fixator-associated complications
Complications occurred in eight of the 10 anatomical regions, as summarised in Table 2. Region of placement was significantly associated with FAC development (P = 0.001). The highest complication rate was seen in the femur (50%), followed by the tarsus (35%) and radius/ulna (33%). The lowest complication rates were in the tibia (3%), pes (5%), spine (0%) and stifle (0%). Region, however, was not significantly associated with complication type (P = 0.505). The regional distribution of complication types is shown in Figure 3. SPTI was the most frequent FAC in the femur and humerus (Table 3), with implant failure being the most common complication in the tarsus (Figure 3).
Fixator-associated complication development at each anatomical region

Type of fixator-associated complications by anatomical region

NC = no complications occurred at this region; PTI = pin tract infection

Regional distribution of fixator-associated complication types as a percentage of overall complications.
Of the 13 cats that developed an SPTI, four were managed successfully with antimicrobial treatment alone, three required pin tract care alone until planned ESF removal, and four required pin removal (details provided in the supplementary material). Two cats with SPTI required limb amputation; one due to non-union caused by pin loosening attributed to the infection, and the other due to unrelated wound complications. Of the 12 cats with implant failure, 50% experienced broken pins. In five cats, all of which had a transarticular tarsal ESF, pin breakages were in the distal bone segment; the sixth cat had a fixator placed on the pes. Loose pins accounted for 33% (n = 4) of implant failures; one cat suffered traumatic displacement of a pin from the femur, and one cat bent a pin in the manus. The cat with pin displacement also suffered clamp failure; no epoxy putty failures were reported (see supplementary material).
Load sharing of long bone fractures was assessed from the radiographs of 57 cats. Load sharing occurred in 12 cats (21%), partial load sharing in 10 cats (18%) and non-load sharing in 35 cats (61%). No significant association between the degree of load sharing and FAC development (P = 0.161) was identified. No significant association between breed, age, sex, weight, fracture type (open vs closed), fixator pins per bone segment and the incidence or type of FAC was identified. Similarly there was no association between ESF type and the incidence (P = 0.634) or type (P = 0.696) of FAC. Time to complication development was not significantly associated with any variable tested, including age, sex, weight, region of placement, fracture type (open vs closed), ESF classification, pin number, load sharing and complication type.
The only frame feature that was significantly associated with FAC development was the use of an intramedullary (IM) pin (Table 1). IM pins were placed in 36 cats, 44% of which developed an FAC. No specific complication type was significantly associated with IM pin usage. When assessed by region, 53% of IM pins (n = 19) were placed in the femur and 25% (n = 9) in the humerus.
Discussion
This is the largest review of ESF usage in cats to date. The most common type of ESF used was the linear ESF, of which the type I and II arrangements predominated. Unsurprisingly, male cats were over-represented in this series, with a young median age of 2 years. The tibia was the most common location for ESF placement. The predominance of the tibia probably relates to ease of placement, with the medial tibia providing safe corridors for pin placement. Despite being the location with the highest level of fixator usage, the tibia had one of the lowest complication rates.
The overall complication rate for cats having an ESF placed was 19%. The region of ESF placement was significantly associated with the development of FACs; the most common locations for complications being the femur (50%), followed by the tarsus (35%) and radius/ulna (33%). Complication type, however, could not be significantly attributed to a location. This may relate to the group sizes when complications were subdivided by type, preventing a significant result from being statistically shown (type II error). To reduce statistical errors, groups with fewer than six cats were excluded from statistical analysis. The majority of complications were SPTIs and implant failure (each with a 9% incidence rate), accounting for 45% and 41% of all FACs, respectively.
Superficial pin tract infection
SPTI is a well-documented complication following ESF placement and was seen in 9% of cats in this study. This is lower than previously reported SPTI rates in dogs, which range from 28–57%.17,18 It therefore appears that cats are less likely to develop PTIs than dogs, and this is something the authors have noted anecdotally. As a complication type, SPTIs accounted for 45% of all FACs, which is similar to the 41% reported in a previous investigation of feline tibial fixation. 6
While the results of the present study revealed no significant regional association with FAC type, the low levels of tibial SPTIs and high levels of femoral SPTIs are suggestive of a true or surrogate influence of anatomical region (Table 3). Studies in the dog have shown an absence of clear, safe corridors in the femur and humerus for transfixation of these bones due to complex regional anatomy, and only limited safe corridors in the radius.19,20 Interference with tendons and musculature in these regions may lead to discomfort, joint stiffness and decreased use of the limb, all of which may predispose patients to FACs due to tissue morbidity and patient interference. PTIs and pin loosening are associated with increased tissue penetration and disruption; hence bone segments with prominent adjacent muscle groups, such as the femur, are at risk.8,11
The reduced rate of PTIs in cats compared with dogs may be due to the fact that cats appear to have a relatively smaller soft tissue envelope, typically with significantly less proximal limb muscle mass and a more marginal subcutaneous fat layer. Potentially the reduced tissue volume associated with a pin tract could mean less soft tissue morbidity and a lower risk of pin loosening or PTIs. 11
It is known from animal studies that the technique of pin placement can influence the development of PTIs. Minimising the distortion of soft tissues is important,2,21 and penetrative stab incisions through the soft tissues of 2–3 mm are recommended. 2 Sufficient incision size can reduce the rubbing between the pin and the soft tissues that contributes to localised tissue reaction. Unfortunately, no such data were present on the sizes and methods used for establishing the soft tissue releasing incision. However, it is commonplace at the authors’ institution to make stab incisions of up to 6 mm in size and to use a small haemostat to open a tunnel through overlying musculature.
In people, PTIs remain a significant issue and numerous postoperative strategies for pin site care have been proposed. 22 However, a recent meta-analysis on pin site care revealed insufficient evidence to identify a strategy that minimises infection rates. 22 Adequately powered randomised trials are required to examine the effects of different pin care regimens prior to making further recommendations. 22
Other reported risk factors for small animal surgical site infection have included sex, increased body weight and duration of anaesthesia.23,24 In this study, however, no association was found between the development of PTIs and age, body weight or sex, although anaesthesia duration data were not available. A further consideration, beyond the scope of this study, are the differences in skin microflora in cats vs dogs, which may also influence infection development. 25
Despite the frequency of PTIs, albeit notably lower in cats than in the dog, these complications are usually manageable – ESF implants can be readily removed and minor short-term morbidity associated with SPTIs often resolves following antimicrobial administration and adequate pin care or implant removal.7,9,26 of the 13 cats with PTIs, only five required specific pin removal, with the remainder managed without surgical intervention until frame removal.

Implant failure
Implant failure had an overall incidence of 9%, representing 41% (n = 12) of all complications. It was the most common FAC in the tarsus (accounting for 63% of tarsal FACs).
Overloaded implants, either due to patient factors or inappropriate implant choice, are vulnerable to fatigue and failure.5,9,29 In this series, the pin was the weakest part of the ESF construct, with pin breakage occurring in six cats, two of which had multiple broken pins. Interestingly, five of these six cats had a tarsal ESF; thus the inclusion of transarticular tarsal ESFs in this study has given this complication a greater prominence. Other studies have also shown the tarsus to be a common region for the development of FACs.2,12,18 Tarsal ESFs are mechanically vulnerable, being subject to significant transarticular bending forces as they cross the flexed tarsocrural joint. Also, relatively small pins may have to be placed in the metatarsal bones, further increasing the construct’s vulnerability to mechanical failure. Interestingly there was a low rate of tarsal PTI (13% of tarsal FACs), possibly relating to the limited soft tissue envelope discussed above.
Load sharing between the bone and the fixator will undoubtedly alter the loading on the pins. Previous guidelines have advised that surgeons should aim to maximise load sharing between fixator and bone column. 21 A canine tibia study corroborated that pins holding unstable fractures exhibited increased loosening. 30 In the present study, the degree of load sharing was not associated with the development of complications; however, specific fracture configuration is likely to have influenced the surgeon’s choice of stabilisation and ESF construct to account for this. The majority of cats in this study had non-load sharing constructs and that is likely to have been a consideration at the outset when planning the fixation method. Activity will also have a bearing on implant loading; however, it was not possible to determine activity levels of each individual cat following discharge and this could have had an influence on complication rates. All animals were discharged with similar instructions regarding cage rest and restricted exercise for the first 6–8 weeks; however, exercise programmes thereafter may have varied.
It is notable that ESFs placed at the pes, manus and combined mandible/maxilla frequently suffered from implant failure. Mandibular fractures can be stabilised using free-form ESFs in cats, which have the added advantages of providing low weight versatile stabilisation.28,31,32 owen et al reported that in mandibular fractures stabilised with pins and either epoxy putty or acrylic, pin loosening was commonly observed at the time of ESF removal. 32 The low overall numbers of fixators placed at these regions in this series preclude meaningful conclusions. Interestingly, the IMEX SK clamp system was used over the study period, and only one connecting bar coupling failure was identified, supporting both its ongoing and versatile use in cats. However, it is acknowledged that mechanical degradation with clamp reuse is reported, 33 and the authors cannot comment on the extent to which that might have been a factor in this retrospective study.
This study showed that pin loosening without infection was a rare complication, occurring in only four cats. There are several important factors (as discussed on page 733) to consider when placing fixator pins to reduce pin loosening.
Bone fracture
Iatrogenic bone fracture was uncommon, occurring in only 1% of cats in this study series. This serious complication usually has contributing factors, such as multiple injuries, the presence of empty drill holes and inappropriate postoperative exercise restriction. 34
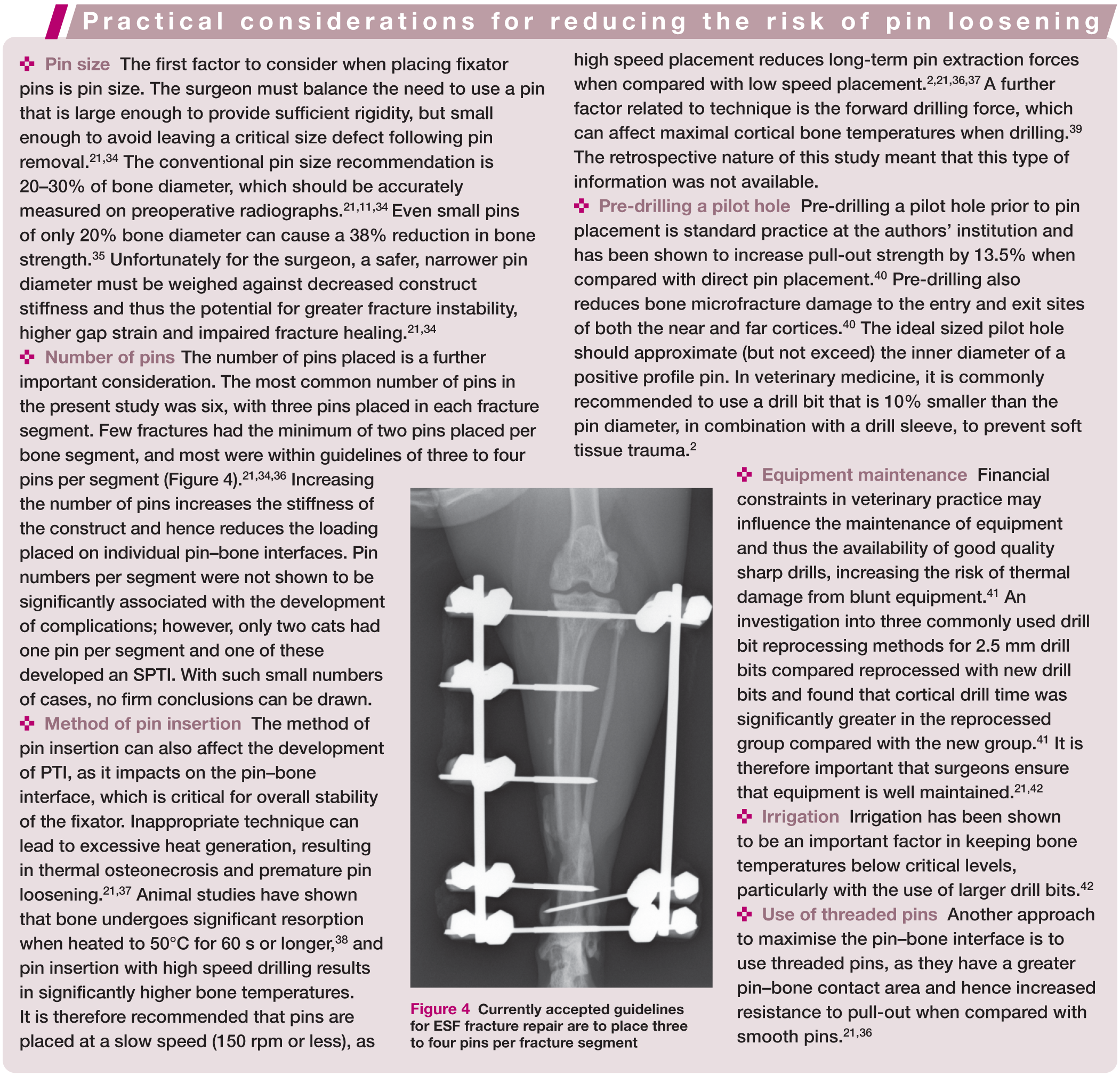
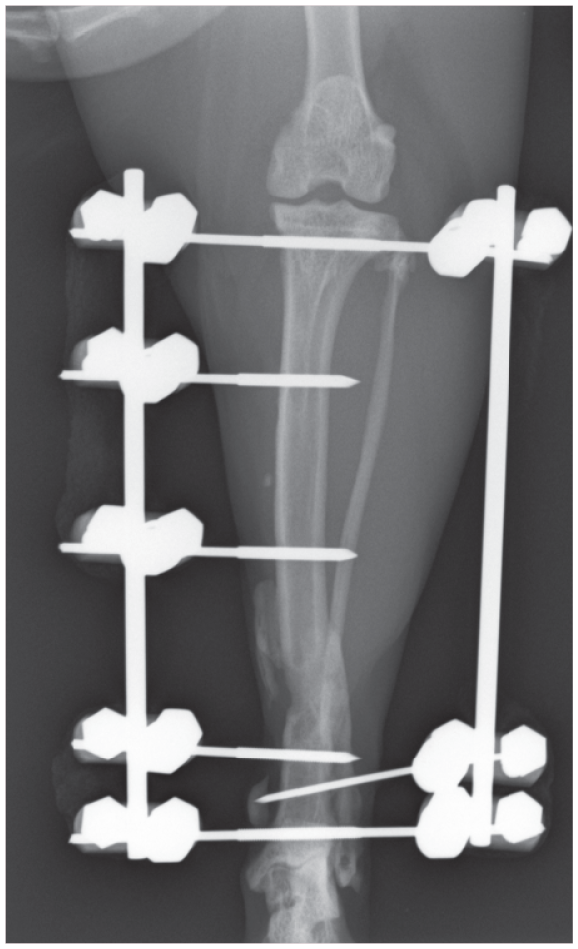
Currently accepted guidelines for ESF fracture repair are to place three to four pins per fracture segment
Influence of specific ESF frame features
A key feature of the ESF is its flexibility in design, and there are numerous frame configurations, implant types, sizes and materials available that can affect construct strength and stability. 43 The use of an IM pin was shown to be associated with postoperative complications; however, the vast majority of IM pins were used in the femur and humerus, which had a higher risk of FAC development. IM pins are commonly employed at these sites to help fracture alignment and to improve resistance to bending.27,44 Their location of use will also be influenced by regional anatomy, as some bones, such as the femur, humerus and tibia, lend themselves to adjunctive IM pin fixation. However, fracture configuration such as comminution will also be a consideration. It is important to note, therefore, that this association with postoperative complications may be a surrogate marker for IM pin usage in higher risk zones or higher risk fracture configurations.
No other ESF feature, including frame type or use of epoxy putty or clamps, was associated with FAC development. Complications have previously been shown to be more common when more complex ESF frames are used.5,6 However, in this study, no significant difference was seen between type I, II and III linear ESFs. Type I ESFs only utilise half pins in their frame configuration, compared with types II and III which contain full pins. As discussed, PTIs are more likely to develop when there has been significant soft tissue penetration, and the use of half pins may minimise disruption.11,45 An effect of full vs half pins was not shown here, whereas the effect of region was. Since the two most affected regions do not readily lend themselves to full pin usage, this may have influenced the impact of frame configuration type. The role of full vs half pins ideally needs to be compared in single anatomical regions, with sufficient case numbers, in a prospective manner.
A caveat when comparing frame configuration data from this study with other situations is the manufacturer of the ESF components; as differing systems have variable bar radius and clamp stability, leading to differences in frame stiffness and bending resistance. Furthermore, the retrospective nature of this study means that surgeons were intentionally selecting a particular frame configuration for a particular fracture, and therefore the association of frame configuration with complications has to be viewed carefully.
Study limitations
This study was retrospective in nature, and multiple surgeons contributed cases over the study period, creating variation in case management and case selection. Detailed evaluation of the initial injury was outside the scope of this study and is likely to have greatly influenced the choice of stabilisation and potentially FAC development. Likewise, intraoperative technical aspects of pin placement were not available for evaluation. The type and size of pins placed was also not consistently available for analysis. Furthermore, due to the referral nature of the caseload, under-reporting of minor complications could have occurred.
Key Points
This is the largest study, to date, reviewing ESF placement and fixator complications in cats.
The overall total complication rate in cats is moderate, at 19%; and lower than in dogs. The cat, therefore, may represent a better candidate for ESF placement.
Region of placement was significantly associated with complication development, with the femur being the most common site for FACs; the complications seen there were dominated by PTIs. The next most common site for FACs was the tarsus, where implant failures predominated. This distinction is attributed to inherent differences between these regions; the lateral femur has a bigger soft tissue mass and lack of safe corridors, whereas transarticular frames in the tarsus are subject to high biomechanical bending forces and a smaller soft tissue envelope.
Particular care should be taken with transarticular frames to ensure sufficient numbers and sizes of pins are used. Type II frames may also be preferable, but no firm conclusions can be drawn based on the present study.
In this study, where the recommended ‘rules’ of external skeletal fixation were followed, frame configuration, pins per segment, open vs closed fracture, and degree of load sharing did not appear to affect FACs.
Being a retrospective study, details regarding confounding influences and factors such as pin placement technique were not available and may need consideration. However, it is conceivable that, even when all the rules are followed correctly, there will be a finite level of complications, mostly pin tract infections, which relate to the nature of a transcutaneous implant.
A prospective evaluation of pin designs used for similar fracture configurations in the same anatomical location is needed. Feasibly other strategies such as silver- or hydroxyapatite-coated pins may be required to reduce these complications further.
On balance, ESF placement can successfully manage a range of complex injuries in a wide variety of anatomical locations.
The higher complication rate in certain locations, such as the femur and tarsus, should be considered when reviewing options for fracture management.
Supplemental Material
Click here for Supplementary Table S1
Fixator-associated complications – case details
Footnotes
Date accepted: 21 February 2017
Supplementary material
Table S1: Fixator-associated complications – case details.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.